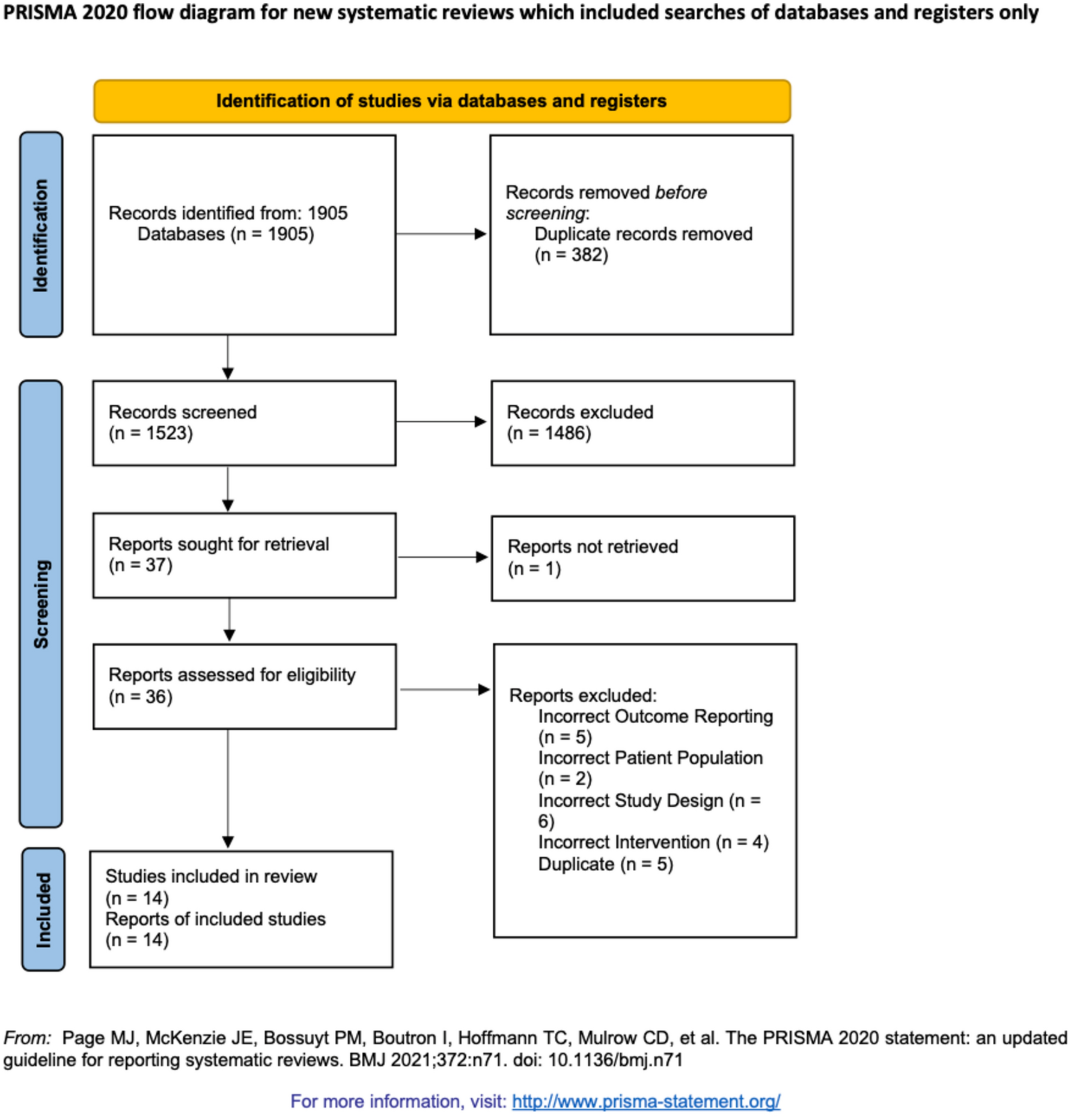
Inclusion process
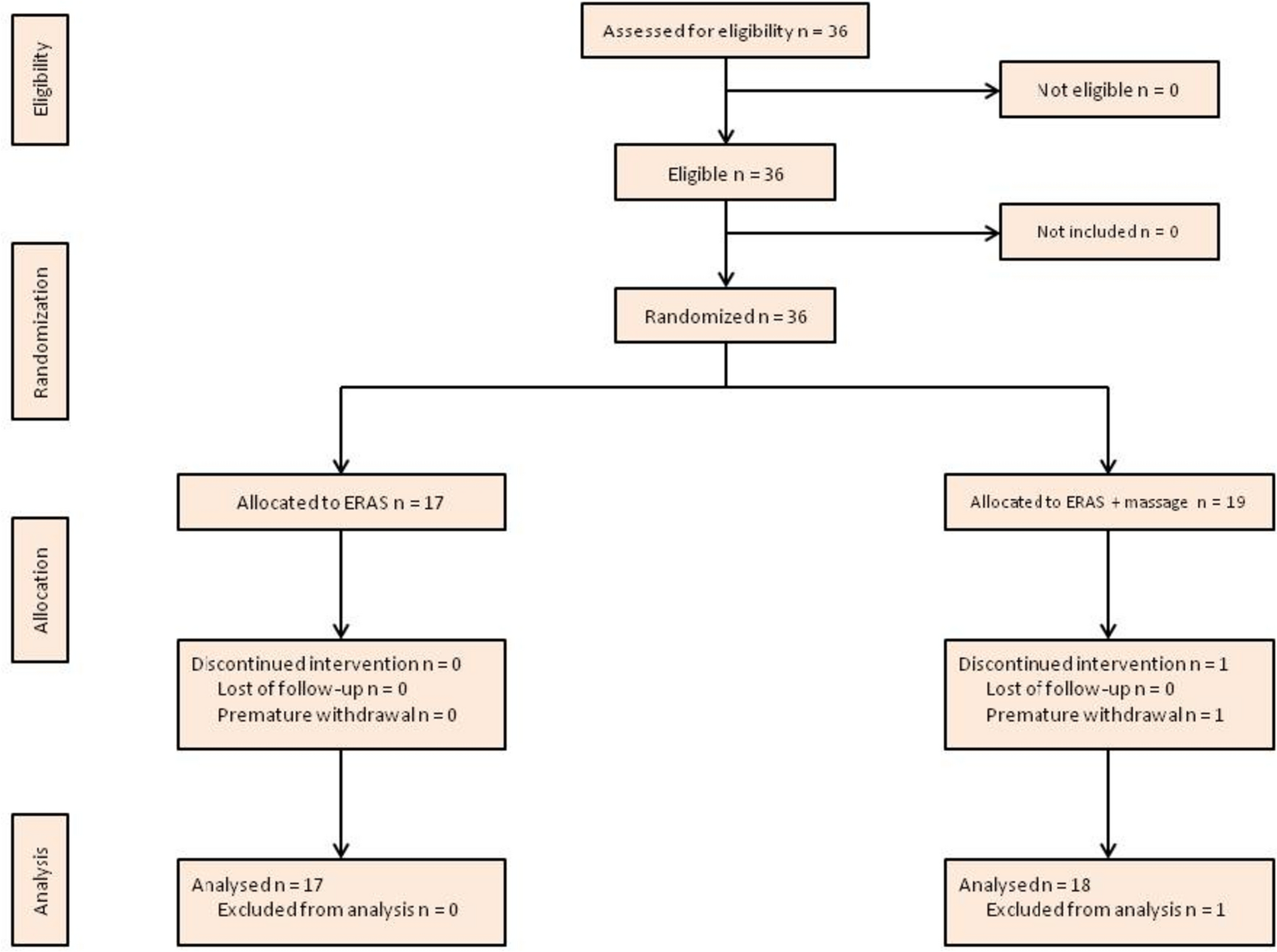
The literature search strategy identified 800 eligible studies. Five-hundred and eighty-three studies were identified in Medline, 34 in Embase and 182 in the Cochrane Central Register of Controlled Trials. Six-hundred and eleven articles were excluded after title and abstract screening. From the 188 full text articles assessed for eligibility, 179 studies were removed for not fulfilling inclusion criteria and/or meeting at least one of the exclusion criteria. From the nine studies left, all fulfilled the inclusion criteria, respected the exclusion criteria and were eligible for the qualitative analysis (Fig. 1).
Characteristics of included studies
Five studies were performed in Europe [19,20,21,22,23], two in the United States [2, 24] and two in Korea [25, 26]. First patient recruitment began in 2000. Four studies were monocentric [21, 22, 25, 26], four were multicentric [2, 20, 23, 24] and one used original data from other publications [19]. Scores included the Colon Leakage Score [22], the modified Colon Leakage Score [25], the REAL score [23], www.anastomoticleak.com [27] and the PROCOLE score [19]. Four studies (44.4%) included more than 1000 patients [2, 20, 23, 24]. Four studies included all types of colorectal surgery procedures [2, 19,20,21] and three only included patients with left-colorectal surgery with left hemicolectomy, sigmoid colectomy, high anterior resection and low anterior resection. [22, 24, 25]. Two studies only included colorectal anastomosis with low anterior resection [23, 26]. A clear and specific definition of AL was detailed in six studies (66.6%) [2, 20,21,22, 25, 26]. The incidence of AL ranged from 3.2 to 14.5% among included studies [2, 21].
Variables included in the scores
Studies included the following pre-operative variables in their scores for prediction of AL: distance from the anal verge (eight studies, 88.8%) (2, 20, 22–27), sex (seven studies, 77.8%) (2, 20–21, 23–25, 27), ASA score (six studies, 66.6%) (2, 20, 22–23, 25–26), age (four studies, 44.4%) (20, 23, 25, 27), neo-adjuvant treatment (four studies, 44.9%) (20, 23–25), BMI (three studies, 33.3%) (20, 21, 23), smoking (three studies, 33.3%) (20, 23, 25), alcohol consumption (three studies, 33.3%) (20, 23, 26), steroid consumption (three studies, 33.3%) (2, 20, 26), diabetes (two studies, 22.2%) (2, 20), respiratory comorbidity (two studies, 22.2%) (2, 20), hematocrit (two studies, 22.2%) (20, 25), anticoagulant medication (one study, 11.1%) (21), cardiovascular comorbidity (one study, 11.1%) (20), liver comorbidity (one study, 11.1%) (20), weight loss (one study, 11.1%) (2), total proteins (one study, 11.1%) (20), WBC (one study, 11.1%) (20), albumin (one study, 11.1%) (20), hospital size (one study, 11.1%) (21), bowel preparation (one study, 11.1%) (25) and indication for surgery (one study, 11.1%) (20) (Table 3).
Table 3 Preoperative variables selected in scoresStudies included the following peri-operative variables in their scores for prediction of AL: duration of surgery (six studies, 66.6%) (2, 20, 22–23, 25, 27), blood loss/transfusion (five studies, 55.6%) (20, 22–24, 27), additional procedure (three studies, 33.3%) (20, 23, 26), emergency surgery (two studies, 22.2%) (20, 23), operative complication (two studies, 22.2%) (20–21), surgical approach (two studies, 22.2%) (2, 25), wound contamination class (one study, 1.11%) (21), mechanical anastomosis (one study, 1.11%) (20) and experience of the surgeon (one study, 11.1%) (20) were specifically used (Table 4).
Table 4 Intraoperative variables selected in scoresDiscriminating ability of scores
Six studies reported the area under the ROC curve (AUC) [19, 21,22,23, 25, 26]. Arezzo et al. [23] with the REAL score (Rectal Anastomotic Leak) reported an AUC of 0.597 (95% CI 0.585–0.608). Pasic et al. [21] announced an AUC of 0.973 (95% CI 0.934–0.992). Yang et al. [25] with the mCLS (modified Colon Leakage Score) outlined an AUC of 0.831 (95% CI 0.767–0.896). Rojas-Machado et al. [19] with the PROCOLE (Prognostic Colorectal Leakage) score reported an AUC of 0.82 (95% CI 0.75, 0.89). Kim et al. [26] documented an AUC of 0.753 (95% CI 0.690–0.816). Finally, Dekker et al. [22] with the CLS (Colon Leakage Score) published an AUC of 0.95 (95% CI 0.89–1.00) (Table 5).
Table 5 Selected studies with AUC, CI, p-value and validation cohort with size of validation population if presentValidation of scores
Four scores (44.4%) (22–24, 26) included a validation set. For instance, Yang et al. [25] used a 170 patients validation cohort and the predictive performance of the modified Colon Leakage Score was similar in the training and in the validation cohorts (AUC: 0.838 vs 0.803, p = 0.724). Pasic et al. [21] had a small size validation cohort with only 40 patients, with an AUC for the score of 1.0. Dekker et al. [22] reported a 121 patients validation cohort and later performed a validation study to evaluate the effectiveness of the AL prediction [28]; Yu et al. evaluate the clinical utility of the colon leakage score (CLS) in predicting the risk of AL and reported an AUC of 0.965 (IC: 0.913–1.00). Arezzo et al. [23] proposed a large validation cohort with nearly 3000 patients with 77.8% of sensitivity and 35.2% specificity for determining the risk of AL.

留言 (0)