
記住我







Although the implantation procedure and management of venoarterial extracorporeal membrane oxygenation (VA-ECMO) is becoming progressively sophisticated, the decannulation process, on the other hand, is still in need for optimization. Until recently, only surgical decannulation1 or manual removal and compression were the primarily used options.2 However, the introduction of new percutaneous closure devices designed for large bore access sites, such as the Manta device (Teleflex, Morrisville, NC) made it possible to facilitate the decannulation process.3,4 Although complication rates are low with novel closure devices like Manta and ProGlide (Abbott Vascular, Clonmel, Tipperary, Ireland), problem-solving in these critically ill patients can be challenging.3 The Manta closure device is specifically designed for large bore femoral arterial access site closure,5 and previously, we reported a thrombus rate of 27.3% at the location of the closure device.6
Here, we present a case of a problematic VA-ECMO explantation and the following problem management.
Case ReportA 70-year-old patient was admitted to our intensive care unit (ICU) after intra-hospital cardiac arrest, requiring postresuscitation care. In terms of recent medical history, the patient had been admitted to our hospital with ST-elevation myocardial infarction complicated further by cerebral infarction 2 days afterward. Before this admission, the patient had no relevant comorbidities documented.
In the succeeding 24 hours after cardiac arrest, the patient suffered a severe cardiogenic shock with a cardiac index of 1. 0 L/min/m². After insufficient response on maximal pharmacologic support with progressing multiorgan failure, the patient was put on VA-ECMO support by ultrasound-guided percutaneous cannulation of the left femoral vessels. After 7 days, weaning of the VA-ECMO was completed with a blood flow of 1.5 L/min, and the patient was stable and scheduled for decannulation.
When ready-to-wean criteria2 are met, two different decannulation approaches are used at our center depending on the blood supply to the limb with the arterial ECMO cannula. In patients without the need for an antegrade limb perfusion cannula, ECMO decannulation is performed in the ICU with the Manta device as described earlier.6 The same strategy is used in patients with antegrade limb perfusion cannula when the systemic blood pressure (as taken from the right arm) closely matches the blood pressure taken from the antegrade perfusion cannula (situated in the superficial femoral artery [SFA]).
However, in this patient, the blood pressure taken in the antegrade limb perfusion cannula was linear, with a mean arterial pressure dropping below 30 mmHg when the ECMO blood flow is paused for the limb perfusion cannula. Therefore, an arterial occlusion distal to the arterial ECMO cannula was suspected, and interventional decannulation was performed. The technique used successfully in our center will be described in detail below; see also Figures 1 and 2.
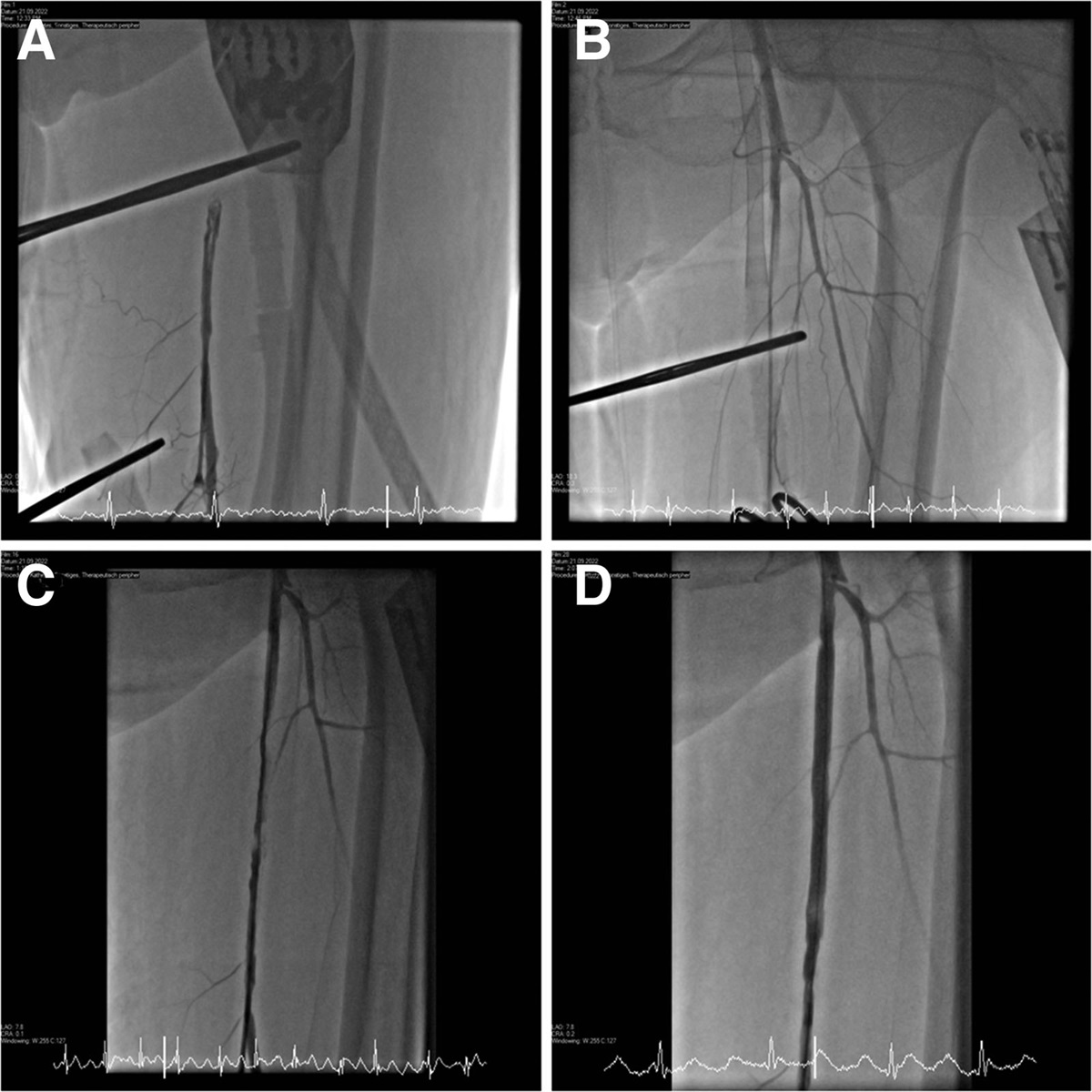
 Figure 1.:
Figure 1.: Venoarterial extracorporeal membrane oxygenation (ECMO) cannula removal. This figure depicts the angiography during cannula removal. A, Distal femoral access was established, and angiography revealed occlusion with dissection of the superficial femoral artery (SFA). B, Introduction of a guide wire through the distal femoral access and its advancement into the common femoral artery, followed by removal of the arterial ECMO cannula using the Manta device. Subsequently, a catheter was advanced over the wire and demonstrated a persistent occlusion distal to the removed arterial ECMO cannula. C, Reopening of the SFA using the AngioJet Peripheral Thrombectomy System, leading to restoration of blood flow to the limb. D, The result after stenting.
 Figure 2.:
Figure 2.: Schematic illustration of the anatomy of the cannulation site. This figure presents a schematic illustration of the anatomy of the cannulation site, including the limb and puncture sites. The distal femoral access is introduced during venoarterial extracorporeal membrane oxygenation (ECMO) decannulation to aid vascular access and retrograde recanalization of the superficial femoral artery.
To perform distal femoral access, a 0.035’ J-tip guide wire is advanced through the antegrade perfusion cannula to precisely locate the SFA. Using x-ray guidance, the artery is then punctured approximately 15 cm distal to the end of the cannula. Finally, a 5-Fr retrograde sheath is inserted into the distal antegrade perfusion cannula. Before removing the arterial cannula, blood in the ECMO system is retransfused.
The arterial ECMO cannula is explanted using the previously described technique.6 In brief, a regular 0.035’ J-tip guide wire is advanced over a puncture of the ECMO cannula. Then, the antegrade perfusion cannula is disconnected, the ECMO is clamped, and the arterial ECMO cannula is removed. Next, the Manta system is deployed over the wire, with an estimated implantation depth of 6–7 cm, as recommended by the manufacturer.
The blood pressure in the retrograde cannula introduced into the distal SFA is recorded, followed by a peripheral angiography. If blood flow is restored to the limb, the antegrade limb perfusion cannula is removed using an 8-Fr AngioSeal device (Terumo Europe N.V., Leuven, Belgium). Another angiography is performed before decannulating the retrograde cannula using a 5-Fr EXOSEAL vascular closure device (Cordis, Miami Lakes, FL).
If the femoral artery becomes occluded after Manta device implantation, an angiography through the retrograde cannula can identify the cause of obstruction. In our patient, a thrombotic occlusion with dissection was detected. The SFA was reopened using a 0.035’ J-tip guide wire. Thrombus aspiration was performed using the AngioJet Peripheral Thrombectomy System (Boston Scientific, Marlborough, MA) and a Solent Omni 6-Fr catheter (Boston Scientific, Marlborough, MA), followed by stenting of the dissection as described before.7 The antegrade limb perfusion cannula and the retrograde cannula from step 1 were explanted as described previously.
After an extended stay at our center after decannulation, the patient was transferred to a rehabilitation clinic. No complications were observed at the decannulation site, and the patient was able to ambulate shortly after decannulation.
DiscussionHere, we describe a novel approach for VA-ECMO decannulation.
Although reported complication rates are low, for example, dissection rates of approximately 5.3% for percutaneous closure devices in this setting,3 it is crucial and necessary to take into account possible complications and to prepare the appropriate means of treatment.
This novel technique may be particularly well-suited for patients with thrombotic occlusion of the access vessel, especially in the region between the arterial ECMO cannula and the antegrade leg perfusion cannula. In these patients with thrombotic occlusion of the femoral artery, surgical explanation had been the preferred method. Recent data of VA-ECMO patients decannulated using the Manta device demonstrate more than 15% of patients had to be converted to surgical repair, mostly for occlusion or bleeding.8 Using this technique, thrombotic occlusions can be revascularized, and device failure leading to bleeding can be overcome by covered stent implantation, especially in combination with other devices like the AngioJet Peripheral Thrombectomy System. Here, we describe our approach on treatment of the thrombotic occlusion with the help of the AngioJet Peripheral Thrombectomy System as a possible alternative therapeutic option.
A notable drawback of this technique is the requirement for an extra arterial puncture. Access of the distal AFS, located deep in the thigh, poses risks of complications such as bleeding, ischemia, exposure to radiation, and infections. We cannot comment on costs of this intervention compared to a surgical cutdown for VA-ECMO decannulation.
To the best of our knowledge, available literature regarding VA-ECMO explantation with percutaneous devices predominantly concentrates on the sole part of sealing the direct puncture site, and no further detail on the management of the reported complications is described.3,9 Different devices are in use today to achieve hemostasis of the arterial puncture site, for example, preclosure devices like the Perclose ProGlide system or percutaneous closure devices for large bore access site like the Manta device.3,9 Vascular closure devices carry notable risks, such as persistent bleeding in 48.8% and vessel occlusion in 29.6% after deployment, as reported in the manufacturer and user facility device experience (MAUDE) registry.10 The technique described here offers the advantage of offering access to endovascular treatment for both occlusion and bleeding through the distal access cannula. In case of failure of the endovascular intervention, a surgical cutdown as bailout should be available.
In case of the need for early recannulation of the common femoral artery, either access to the vessel at least 2 cm proximal to the Manta device (using the radiopaque marker of the Manta device as guidance) or a contralateral cannulation should be considered.
ConclusionsDistal femoral access is an easy and promising technique for rapid and safe complication management during VA-ECMO explantation.
References 1. Chan YM, Lazaravicuite G, Renwick B. Surgical decannulation of veno-arterial extracorporeal cardiopulmonary resuscitation (VA-ECPR): a technical note. J Anesth Crit Care open access. 10: 97–99, 2018. 2. Bishop MA, Moore A. Extracorporeal Membrane Oxygenation Weaning, in: StatPearls. Treasure Island (FL): StatPearls Publishing, 2022. 3. Au S, Chan K-S, Fong K, et al.: Comparing the outcomes of bedside percutaneous VA-ECMO decannulation by ProGlide and Manta in a high-ECMO-volume center in Hong Kong. Artif Organs. 46: 1382–1388, 2022. 4. Hwang J, Yang JH, Sung K, et al.: Percutaneous removal using Perclose ProGlide closure devices versus surgical removal for weaning after percutaneous cannulation for venoarterial extracorporeal membrane oxygenation. J Vasc Surg. 63: 998–1003.e1, 2016. 5. Wood DA, Krajcer Z, Sathananthan J, et al.; SAFE MANTA Study Investigators: Pivotal Clinical Study to Evaluate the Safety and Effectiveness of the MANTA Percutaneous Vascular Closure Device. Circ Cardiovasc Interv. 12: e007258, 2019. 6. Bemtgen X, Heidt T, Zotzmann V, et al.: Venoarterial extracorporeal membrane oxygenation decannulation using the novel Manta vascular closure device. Eur Heart J Acute Cardiovasc Care. 9: 342–347, 2020. 7. Ierardi AM, Xhepa G, Piffaretti G, et al.: Clinical experience with Angiojet: a comprehensive review. Int Angiol. 34: 1–14, 2015. 8. Dalén M, Settergren M, Kastengren M, Ullström P, Fux T: Percutaneous decannulation of extracorporeal membrane oxygenation using a plug-based closure device. Catheter Cardiovasc Interv. 99: 1945–1952, 2022. 9. Martin-Tuffreau A-S, Bagate F, Boukantar M, et al.: Complete percutaneous angio-guided approach using preclosing for venoarterial extracorporeal membrane oxygenation implantation and explantation in patients with refractory cardiogenic shock or cardiac arrest. Crit Care. 25: 93, 2021. 10. Megaly M, Sedhom R, Abdelmaseeh P, et al.: Complications of the MANTA closure device: insights from MAUDE database. Cardiovasc Revasc Med. 34: 75–79, 2022.
留言 (0)