
記住我


From January 2017 to September 2023, 688 patients in our hospital need to underwent PCN were preliminary selected. Scrutiny and record the basic information of all patients (gender, age, clinical symptoms, etc.). Criteria applied for patients’ inclusion to carry out UCA assisted US guided PCN group was shown in Table 1 and the basic information of the selected study sample was manifested in Table 2, respectively.
Table 1 Criteria for inclusion to performed UCA assisted US guided PCN groupTable 2 Basic information of the study populationFigure 1 delineates the screening procedure, whereby a total of 13 participants with non-hydronephrosis were included in the study sample. This sample comprised 5 male and 8 female individuals, with a mean age of 58.46 ± 17.35 years (range, 37–88 years). Furthermore, the study sample encompassed a total of 20 kidneys.
Fig. 1
The flowchart of patient screening procedure
Ultrasonography apparatus and probeUltrasound images were obtained utilizing the Philips EPIQ 7 system. Linear array probes and convex array probes were employed for ultrasonic examination. Specifically, the linear array probe operated at frequencies of 3–12 MHz and 5–18 MHz, while the convex array probe operated at a frequency range of 1–5 MHz.
Technique of UCA assisted US guided PCNAll procedures were performed by two urologists with more than 10 years of experience in performing PCN. Meanwhile, two sonographers with more than 7 years of experience in performing UCA assisted with administration of US guidance intervention.
Step 1 Perpetration of UCA solution—The UCA applied in this study is sulfur hexafluoride MBs (SonoVue, Bracco Suisse SA, Switzerland). Briefly, 5 mL of 0.9% sodium chloride solution was injected into a bottle of sulfur hexafluoride MBs and shake it slightly to make a dispersion solution [21]. Next, a 1 mL sample of the thoroughly agitated sulfur hexafluoride MB solution was extracted and subsequently injected into 100 mL of normal saline in order to produce a diluted UCA solution for future application.
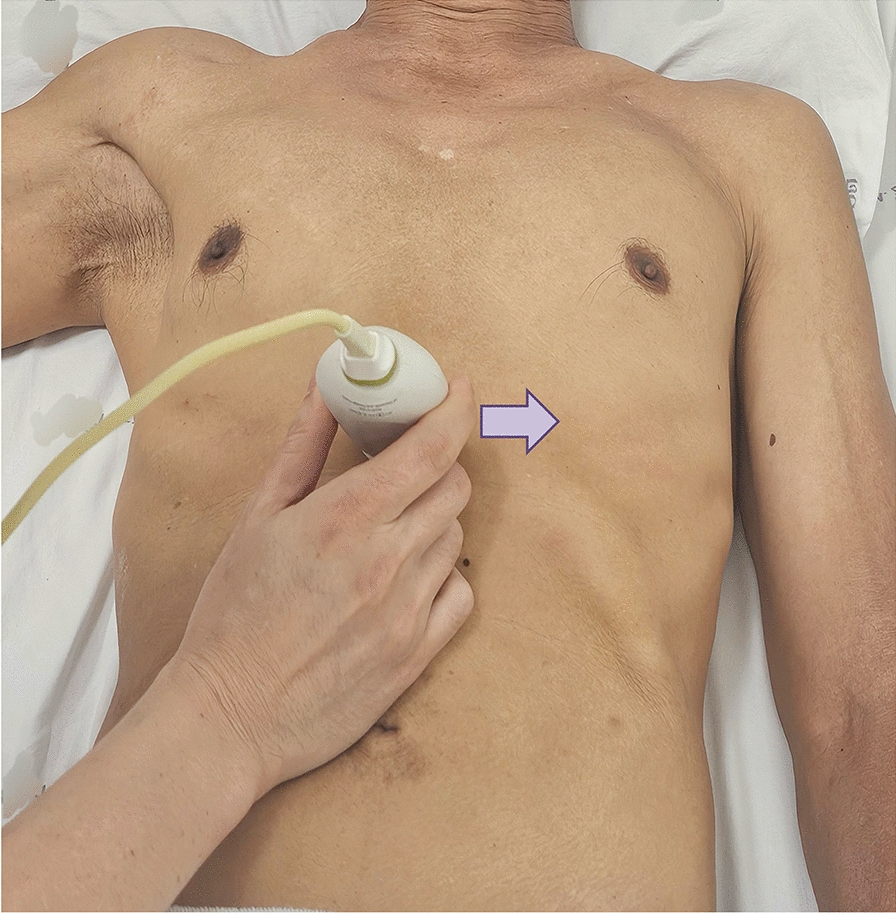
Step 2 Puncture needle insertion course and patients’ position—Based on the renal anatomical structure and vascular distribution, it is recommended that the needle be inserted perpendicularly at the puncture site, traversing the layers of skin, subcutaneous tissue, renal capsule, renal pyramid, and renal medulla. This approach aims to minimize the distance of needle insertion and mitigate potential harm, as Fig. 2a shown. Prior to needle insertion, it is imperative to conduct a Color Doppler ultrasound examination to ascertain the absence of any significant blood vessels at the intended site of insertion.
Fig. 2
Diagram of puncture needle insertion course and patients’ potion. a the insertion course (black arrow) should avoid the blood vessels of renal calyx. The schemes were powered by Figdraw; b Patients lies prone in the prone position. This diagram was draw by author
Step 3 Puncture—Patients were placed into prone position, as Fig. 2b shown. Injected 5 mL of 1% Lidocaine Hydrochloride solution (Harvest Pharmaceutical, CO., LTD, Shanghai, China) for infiltration anesthesia. Cut skin with a No.11 sharp knife to the level of half the blade. Under the guidance of US, the 18-gauge × 15 cm PTC needle (Hakko Sonoguide, Japan) was placed into the puncture guide groove. It is of great necessity to exhort patients to hold their breath and slowly insert the needle along the direction of the puncture frame. When the image displays the precise location where the puncture needle penetrates the tip of the renal pyramid, the needle core should be withdrawn. Subsequently, the prepared UCA media should be injected into the patients. By injecting the diluted UCA solution, the structures of the renal calyx and renal pelvis can be clearly visualized in the resulting images.
Step 4 Dilating catheter —A 0.035 inch × 80 cm guidewire (Radifocus, Terumo Corporation, Tokyo, Japan) was insert into the renal pelvis through the PTC needle sheath. Withdraw the needle sheath, inserting the arterial sheath (Radifocus Introducer II, Terumo Corporation, Tokyo, Japan) along the guidewire direction for dilation. Retracted the inner core and withdraw the urine could suggested that the dilating catheter progress was accomplished. Then, retracted the sheath, place the BARD drainage catheter (Bard Access System, USA) into the renal pelvis along the guidewire. Remove the guidewire and the fixed soft core of the drainage catheter gently when the part of the drainage catheter enters the kidney. Tighten the tip of the catheter to secure the wire and close the latch, fixing the drainage catheter and stick a sterile dressing to the wound at the puncture point and connecting Discofix (Braun Melungeon, Germany) and anti-reflux drainage pack.
Assessment of complicationsAll patients were prospectively monitored to document the 24 h urine drainage volume of the fistulectomy catheter, the incidence of complications, and the amelioration of clinical symptoms, among other variables. Patients were contacted daily throughout their hospital stay. Upon discharge, follow-up was limited to subsequent visits for medical attention.
Data collectionRecord the significant images of the operation process. The success ratio is measured through whether the drainage catheter is successfully placed into the destination renal calyx and whether the urine can be successfully extracted or not. Meanwhile, the total dose of used UCA solution for each patient was recorded to calculate the mean value and the complete operation time were noted. All data were analyzed through GraphPad Prism software (version 8.0.2, San Diego, United States). Mean ± standard deviation was utilized to describe quantitative variables.
留言 (0)