
記住我

The psycho-neuro-endocrine-immune (PNEI) system should play a major role in medical and surgical diagnosis and treatment. This is based on the “holistic” approach, which takes into consideration both the body and the psyche of the patient. The term “holistic” comes from the ancient Greek word όλος (holos), which means “all” or “the whole.” This means that the physician should not just treat the part of the body that appears to be diseased but look more deeply into the etiology of the disease, using an interdisciplinary approach [1,2,3].
Coloproctologists should be prepared to deal with (i.e., at least diagnose) both anterior and middle compartment disorders, which may be controlled by (and exert feedback on) the PNEI system.
PNEI, which is valid for all organs and systems of the body, can be applied to the tricompartmental procto-uro-gynecological system. This proposal of the PNEI approach in procto-uro-gynecology is, to the best of my knowledge, original, as there is nothing in the literature concerning this topic.
Figure 1 shows the procto-uro-gynecological system surrounded by a rhombus, with psyche/mind (P), nerves (N) endocrine glands (E), and immune system (I) at the vertices. This rhombus indicates that P, N, E, and I influence the function and morphology of the various tissues and organs in the tricompartmental system, as indicated by the arrows pointing from each vertex of the rhombus to the center. The arrows pointing in the opposite direction, from the center to each vertex, indicate that the diseased rectum, bladder, and other organs/tissues can influence the P, N, E, and I. There is thus bidirectional feedback.
Fig. 1
The PNEI rhombus with the procto-uro-gynecological system at the center. P psyche, N nerves, E endocrine glands, I immune system
The importance and clinical implications of PNEI-based management of patients can be clarified by considering the following specific cases/data. These are cases of anorectal/colorectal disorders because the focus of this journal is coloproctology.
P for Psyche
The patient was a primiparous 45-year-old woman with severe lower abdominal pain, dysuria (i.e., frequent voiding or pollachiuria and stress urinary incontinence), constipation (i.e., obstructed defecation with need for straining at stool, daily laxatives, and weekly enemas). On procto-uro-gynecological examination, a hystero-colpo-cystocele was found anteriorly, and proctoscopy revealed a second-degree (i.e., reaching the dentate line on straining) rectal internal mucosal prolapse (RIMP) plus a 3-cm-wide rectocele.
The patient had experienced two extremely stressful events 6 months prior to the onset of symptoms: loss of her husband and a financial crisis. Subsequently, she became severely depressed and anxious, but neither her family doctor nor specialists suggested that she see a psychologist.
As the gynecological symptoms were more stressful than the others, she went to a gynecologist, who performed a hysteropexy. She went to a urologist, who managed the urinary incontinence with medical treatment and sent her to a physiotherapist for urinary bladder and voiding rehabilitation.
As the constipation worsened, a proctologist performed anorectal manometry, showing low resting tone and voluntary contraction plus a degree of rectal hyposensitivity (i.e., first sensation, desire to defecate, and maximal urgency were elicited with endorectal balloon inflation with < 20, 60, and 120 ml of air, respectively). Moreover, on proctological examination, the anal reflex was slightly impaired, perineal descent was 2.5 cm on straining, and both rectocele and internal mucosal prolapse were detected. Defecography did not show any anismus, but just recto-rectal intussusception plus a small rectocele.
The proctologist reported in the clinical notes that the patient was depressed but did not suggest a psychological evaluation. He performed hydrocolontherapy, which did not improve the constipation. Then he proposed rectocele repair and performed an anterior levatorplasty using Prolene.
It should be noted that the indications for surgery in case of rectocele are as follows: (i) rectocele wider than 3 cms and (ii) need for manipulation or self-digitation to extract the stool from the rectum. In the case under discussion, neither indication was present.
Following surgery, the patient experienced intense anoperineal pain, with a visual analog scale (VAS) score of eight out of ten for a week, and was still constipated. Therefore, she agreed to undergo a RIMP excision, and the same surgeon performed an internal Delorme. Unfortunately, both constipation and rectal pain increased. The patient went to see a general surgeon, who performed a colectomy and ileo-lower sigmoid anastomosis, without having investigated the intestinal transit times with radiopaque markers.
After 2 months, the patient still had severe constipation, with proctalgia and tenesmus, plus urgency and occasional fecal incontinence.
Fortunately, the uro-gynecological symptoms had markedly improved.
Finally, a gastroenterologist suggested magnetic resonance (MR) defecography and a psychological consultation, hypothesizing that both ano-recto-pelvic surgical adhesions and mental distress had a major role in the etiology of her symptoms.
Some reactive graphic tests were then carried out, including the Draw-the-Family test [4], the Rorschach test, and the Minnesota questionnaire. Moreover, the anxiety pattern was investigated with the State-Trait Anxiety Inventory (STAI), aimed at evaluating both state and trait anxiety. All tests were positive for mental distress, thus suggesting that the mental component of her symptoms was relevant.
MR-defecography showed the presence of a misdiagnosed enterocele, which most likely caused the lower pelvic pain after abdominal surgery. Regarding the other postoperative disturbances, the rectal pain might well have been caused by the suture with Prolene of the highly sensitive levator muscles during the rectocele correction. A levatorplasty with very slow absorbable stitches (i.e., polydioxanone) would have been more appropriate. The colectomy should have been avoided. It has been reported that a significant number of patients who undergo colectomy and ileorectal anastomosis for either megacolon or slow transit constipation may experience depression and embarrassment after surgery. This is probably due to postoperative disorders of anal continence, experienced by nearly half of patients following total colectomy [5].
A psychological evaluation, if performed prior to surgery, would have focused the treatment on the mental–functional and not on the organic aspect, and the stressful postoperative course and lack of recovery could have been avoided.
The PNEI tricompartmental approach should therefore be kept in mind when dealing with patients who have obstructed defecation, as there is often more than one occult cause of symptoms due to urogynecological diseases, such as hystero, colpocele, and cystocele, as shown by the iceberg diagram [6].
N for Nerves
The patient was a 25-year-old man with severe chronic constipation. A stapler-friendly proctologist attributed the constipation to recto-rectal intussusception without conducting in-depth diagnostic studies, and performed a stapled transanal rectal resection (STARR). STARR, which has been associated with severe complications, such as peritonitis, recto-vaginal fistula, and even death, has been defined as the classic example of a technological innovation introduced into clinical practice without adequate experimentation [7]. The procedure never obtained US Food and Drug Administration (FDA) approval.
The surgeon focused all his attention on the organ involved, the rectosigmoid, instead of using a holistic approach and considering possible PNEI elements. The constipation persisted.
The patient then went to his uncle, a thoracic surgeon, who performed an operation outside of his area of competence. He resected the transverse and descending colon and created an anastomosis between the cecum and sigmoid. The constipation persisted.
Then the patient came to our clinic. We used the PNEI approach. Since he had had chronic constipation all his life, we wondered whether he had a deficit of the nerve plexus in the rectum resulting in the absence of peristalsis and difficulty evacuating. Anorectal manometry showed that the rectoanal inhibitory reflex was impaired and delayed. A full-thickness rectal biopsy revealed rectal hypoganglionosis. We proposed a Duhamel procedure, but the patient was tired of surgery and preferred to continue with laxatives and enemas.
E for Endocrine Glands
This is a case from 30 years ago, before we were aware of PNEI; however, the same approach was ultimately used to treat the patient.
A 60-year-old woman with severe chronic slow transit constipation underwent colectomy with ileorectal anastomosis. In the following weeks, she had diarrhea and urgency, normal sequelae of the surgery. We expected the distal ileum and the rectum to dilate, but this did not occur. Months later, she still had diarrhea and hypokalemia (2.0 mmol/L). One member of the team with extensive knowledge of gastrointestinal hormones suggested that the problem might be due to peptide YY (PYY), also called the “ileal brake,” because it slows down the passage of chyme from the terminal ileum into the cecum.
PYY is produced by the enteroendocrine L cells in the terminal ileum, colon, and rectum. Perhaps, after the colectomy, the chyme passed from the terminal ileum directly into the rectum, without the ileal brake, causing diarrhea. Testing revealed that the postprandial levels of PYY in the patient were the same as preprandial levels.
Although Hopman et al. [8] found that colectomy, i.e., removal of the major source of PYY-secreting cells, does not induce major impairment of PYY in slow transit constipation, the long duration (i.e., decades) of constipation in our patient might well have caused a lack of production of postprandial PYY at the ileorectal anastomosis. A variation (i.e., increase) of the peristaltic drive of the terminal ileum in our patient might well explain this discrepancy.
It seems that the condition of the target organ (in this case, the colon) had, over the years, modified the production of PYY in the intestine (feedback from the center of the PNEI rhombus to the E vertex).
The next step was reintervention. We constructed an ileal reservoir above the ileorectal anastomosis, to slow down the flow of chyme. We also performed a postanal repair of the pelvic floor (Parks’ method) to improve continence. (At that time, in our experience, this operation was effective in more than 50% of patients at 3 years.) The diarrhea resolved almost entirely, and the patient was no longer hypokalemic.
The integrity of the nerve fibers that relay sensory and motor information between the brain and the anorectum is essential for anorectal function [9]. The importance of modulation by sensory input explains why sacral neuromodulation can provide better results in patients with fecal incontinence than a procedure involving plication and reattachment of markedly denervated sphincter muscles [10].
I for Immune System
A 52-year-old man came to our clinic because of recurrent anal sepsis, i.e., a mid-transsphincteric fistula and ischiorectal abscess. He had undergone two unsuccessful attempts at surgical management.
His wife had died in a traffic accident 2 months before he developed anal sepsis. He was aware that he required surgery for the third time and was worried about the risk of fecal incontinence. The patient appeared to be extremely distressed. After an evaluation that included the State-Trait Anxiety Inventory (STAI) TX-1 and TX-2, the psychologist on our team diagnosed severe anxiety. The Draw-the-Family test, which is useful for identifying psychosomatosis underlying anorectal disease [4], revealed a series of altered parameters. Psychotherapy was recommended.
Before performing surgery, we decided to investigate whether the patient’s anal sepsis was induced or facilitated by deficits in his immune system. Laboratory tests revealed vitamin deficiencies and low levels of C-reactive protein and immunoglobulins. The patient was a nonsmoker (smoking can damage sutures after fistulectomy) [11]. He reported insomnia and excessive alcohol consumption, both of which can weaken immune defenses. We prescribed medical and diet therapy to strengthen his immune system (no alcohol, undercooked meat, dry fruit, black currants, apple vinegar, green vegetables, and above all propolis- and echinacea-based supplements with vitamins A, B, C, D, and E, as well as zinc and iron).
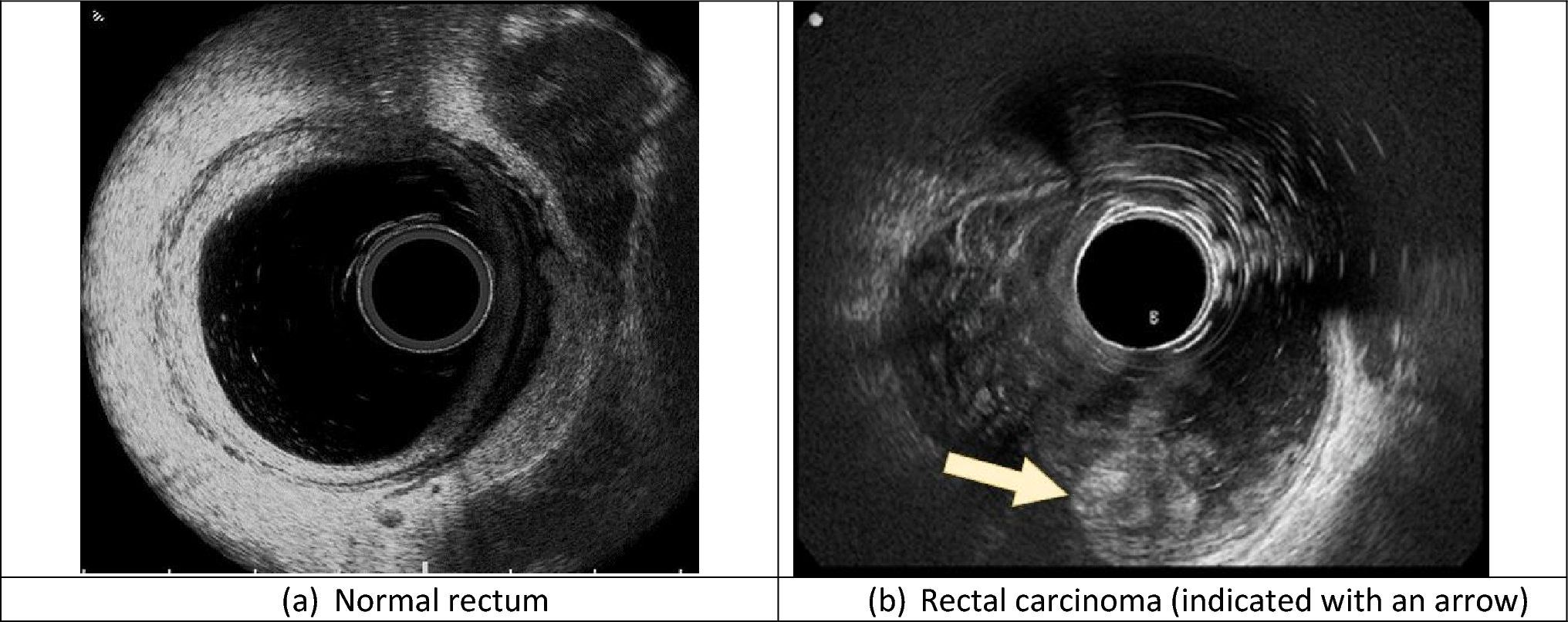
Two weeks later, we performed sphincter-sparing surgery (fistulectomy and abscess removal with rectal advancement flap). The postoperative course was uneventful. After 1 month, the surgical wound had healed and transanal ultrasound with a 12-mHz rotating probe showed uniform healing.
Three years later, the patient had not experienced recurrence. He had continued to see a psychologist, maintaining the P of PNEI as stable as possible, and continued the medical and dietary therapy to strengthen his immune responses.
It has been shown that elevated levels of anxiety play an important role in the pathogenesis of anal fistula [12] (once again, the P of PNEI.) Moreover, it is well known that psychological stress is linked to dysregulation of the immune system [13]. A recent study [14] on the pathogenesis of cryptoglandular anal fistula found a specific immunological profile associated with anal fistula.
留言 (0)