
記住我



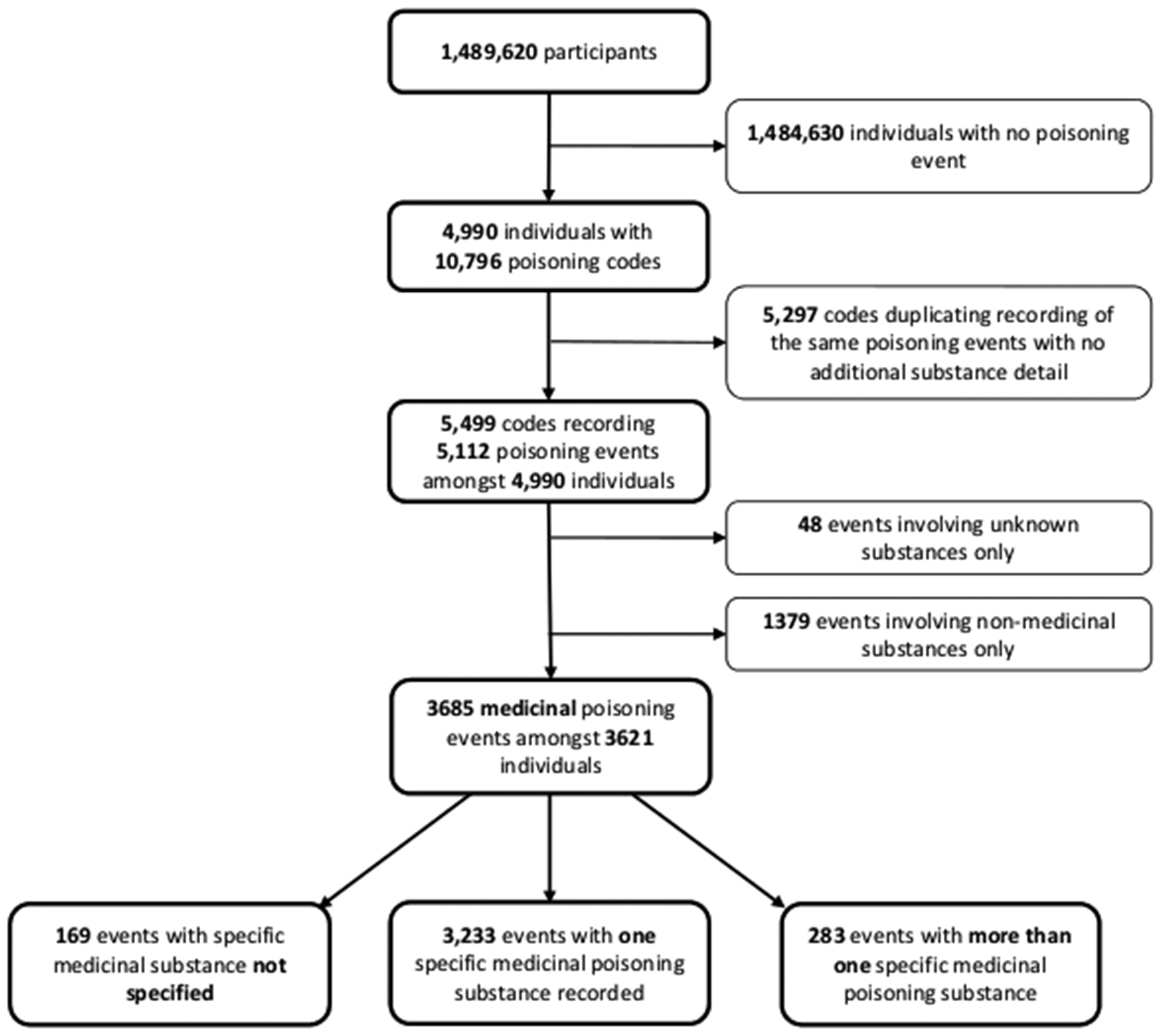
Articles that did not meet the criteria during screening were excluded with the reasons recorded in the PRISMA flowchart, which also reports the different phases of article selection [21] (Fig. 1).
Fig. 1
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flowchart of searches and documents included in the qualitative systematic review of factors influencing participation in personalized breast cancer screening, until March 2022
Characteristics of studiesMain characteristics of included studies are reported in Table 2 [18, 22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38]. Of the 18 studies, 17 were qualitative and one had a mixed methods design. No studies were excluded based on their quality.
Table 2 Characteristics of the studies included in the qualitative systematic review of factors influencing participation in personalized breast cancer screening, until March 2022All papers were published between 2017 and 2022, with the majority published in the last three years. Nine studies were conducted in Europe (five in the United Kingdom, one from Spain, one from Germany, and two multicenter studies conducted with women from the United Kingdom, the Netherlands and Sweden). Outside Europe, four studies were conducted in Canada, three in Australia and two in the United States. Eleven were nested in breast cancer personalization projects: Breast Cancer Predict and PRISMA (UK), PERSPECTIVE (Canada): DECIDO (Spain) and RISIKOLOTSE (Germany).
The models and factors included for risk prediction varied slightly across the different studies: the Decido study calculated the 5-year risk using The Breast Cancer Surveillance Consortium v2.0 (BCSC v2.0), which included age, race/ethnicity, first-degree family history of breast/ovarian cancer, personal history of benign breast disease, breast density, and PSR [7]. In PROCAS/BC-Predict, UK they used the Tyrer-Cuzick model (v8), which in addition to the abovementioned factors, took into account body mass index and height. In the PERSPECTIVE project, they calculated risk using the BOADICEA model, in which various lifestyle factors were added [4]. With the exception of the DECIDO project, the risk estimates were calculated at 10 years.
Nine studies included only women and aimed to explore the acceptability, views and perceptions of risk-based screening. Nine studies included HCPs and were focused on the exploration-description of determining aspects in the future implementation of personalized screening strategies. Eleven authors of selected studies were contacted to complete missing information. Three of them facilitated data, which accounted for five studies (Table 2).
Characteristics of participantsWomen: In total, 478 women participated in nine included studies. All, except one, included women under 50 years of age. Most women were from developed countries, white, and of medium–high socioeconomic and educational level. Two studies included women from ethnic minorities living in Western countries [22, 37].
In four studies [23,24,25, 37], women had participated in personalized screening programs: in one study, women were purposively selected who were estimated to be at low risk [23], in a second, only at high risk [37]. In the other two studies [24, 25], 34% were classified as high risk (Table 3).
Table 3 Characteristics of the women participating in the studies included in the qualitative systematic review of factors influencing participation in personalized breast cancer screening, until March 2022HCPs: Overall, 162 HCPs participated in nine studies. Most were female (70%). The professional profiles were diverse, including physicians and nurses, policy makers of breast cancer screening, and Public Health programs. Three studies included genetic counselors and one included academic experts. The studies were performed in Primary Care contexts [3], and specialized centers of Breast Cancer Early Detection Programs [4] (Table 4).
Table 4 Characteristics of heath care professionals participating in the studies included in the qualitative systematic review of factors influencing participation in personalized breast cancer screening, until March 2022ThemesThe findings of the studies were classified, synthesized and organized into major themes and sub-themes, generated from: i) deductive analysis of the contrast with the levels of the MICCC model, ii) inductive analysis of findings not considered in the MICCC model, from which three sub-themes emerged. In a first analysis, 6 themes, 21 sub-themes and 85 findings were identified; these were synthesized into 3 themes, 14 sub-themes and 43 findings (Table 5).
Table 5 Themes, findings, and authors of each study included in the review of factors influencing participation in personalized breast cancer screening, until March 2022The results are presented through a model showing the factors for and against women’s participation in personalized breast cancer screening programs. We also included the perspectives and opinions of HCPs on these factors. The opinions of HCPs are derived from the relationships established with women who have participated and/or allegedly participated in a personalized screening program (Fig. 2).
Fig. 2
Factors for and against women’s participation in personalized breast cancer screening programs obtained from the systematic review
Theme 1. Factors related to womenBeliefs about breast cancer, risk, and personalized early detection of breast cancerHCPs reported a strong social perception of women’s susceptibility and severity of breast cancer [26, 27]. They identified fatalistic beliefs expressed by women: it is a common and “omnipresent” disease, which appears randomly [28], without reason or pattern, and cannot be avoided. Therefore, all women are at risk and vulnerable to suffer from it no matter what they do to avoid it [37].
Some beliefs associated to an increased risk of breast cancer included: having a family history of breast cancer [23, 28, 29, 37, 38], large breasts, not having children [23, 30, 37], have undergone in vitro fertilization treatments [24, 28], being in poor health, and lifestyle factors (unhealthy diet and smoking) [37]. On the other hand, it is believed that the risk decreases with increasing age and menopause [26, 28], no family history of breast cancer in the first line of con-sanguinity, and healthy lifestyle behaviors [28]. In relation to personalized screening, it was believed that more screening tests were better and fewer tests allowed early diagnosis to be missed [18, 28], genetic testing could accurately predict a diagnosis and when there is a family history, the onset of the disease skipped a generation [25].
Knowledge on personalized early detection of breast cancerWomen’s knowledge of personalized screening showed mixed results, overall, a low general knowledge prevailed [18]. Genetic testing was considered strange, an incomplete, unknown, or future science, rather than a currently useful information and technology. There was concern about the overemphasis on genetics in the algorithm for risk calculation [30]. Personalized screening was considered a diagnostic procedure and ongoing risk estimation was necessary because of the modifiable nature of breast cancer and some lifestyle-related risk factors (body mass index, alcohol consumption, physical activity); and others such as the use of hormonal contraceptives [28, 31, 37]. In general, there was not sufficient knowledge and understanding of the risk and the probabilities of developing breast cancer according to the estimated risk [37].
HCPs considered that lack of knowledge had negative consequences by making it difficult to understand the benefits of personalization [27], increasing the chances of misinterpreting risk (low risk as no risk) [23, 26], and overestimating and/or denying it [32].
Two studies reported that women had adequate knowledge of this strategy, in a context where they were aware of risk due to family history of breast cancer: early detection decreased the likelihood of breast cancer being fatal [37], and risk estimation could save the lives of women at high risk and those with breast cancer family history offering early detection and prevention [29].
Reasons women reported to know their risk included: (i) general curiosity, knowledge is considered “power”; (ii) to learn more about breast cancer, be aware of the disease and detect it early; (iii) to help future generations (daughters and young women in the family) in the early detection of the disease [37]; (iv) to decide on the use of hormone replacement therapy during menopause [23]; (v) to accept screening frequency recommendations [25, 29, 37].
Psychological reactions to breast cancer risk estimationPsychological reactions were not homogeneous and vary according to the real or hypothetical estimation of breast cancer risk.
In two studies where women participated in a personalized early detection program, the estimation of a low risk produced a sense of relief and peace of mind, as they did not consider the disease a direct and immediate threat to their lives and could thus reduce the frequency of screening [23, 25]. However, in another group, knowing that they were at low risk did not have much impact [23, 25]. In contrast, HCPs felt that a low risk generated anxiety and uneasiness due to the change in screening strategy [30], with longer mammography intervals and fear of a late stage diagnosis [26, 33].
A high risk also generated anxiety and uneasiness, but for other reasons: the perception of breast cancer as a burden in women’s lives related to the feelings of guilt and stigma generated by the disease [25]. It also caused helplessness and fear by feeling that cancer is “inevitable” [25, 31, 38]. Likewise, because of the generation of contradictory feelings: at the same time that they offload on themselves the responsibility for their breast health, it is not their responsibility if they develop breast cancer [25].
However, for other women worrying about high risk was considered unnecessary because it did not mean they would develop breast cancer, and they only needed to be diligent with early detection of the disease. Also, because having a family history of chronic diseases, such as diabetes and hypertension, were perceived as more immediate threats that diminished concern for high risk of breast cancer [37].
HCPs did not agree with women on the negative impact that a high risk could have, stating that it could be reassuring and decrease anxiety, especially for those who have a reason to worry about a diagnosis of breast cancer [27, 34]. However, HCPs in a Canadian study considered that a factor generating anxiety would be the possibility that women at high risk could be treated differently by health insurers [
留言 (0)