
記住我







Amniotic fluid embolism (AFE) is a potentially lethal complication of pregnancy that results from disruption of the maternal–fetal interface and occurs as frequently as one in every 8,000 deliveries.1 When AFE is complicated by cardiovascular collapse, the Society of Maternal-Fetal Medicine (SMFM) recommends against routine use of veno-arterial extracorporeal membrane oxygenation (V-A ECMO) in AFE due to a lack of robust evidence of benefit and the potential risk for anticoagulation to worsen bleeding in patients with coagulopathy.2
Despite advances in maternal mortality in the 20th century, since 2000, maternal mortality has been rising.3 The outcomes of AFE are frequently catastrophic, with coagulopathy, respiratory failure, and cardiac arrest being common. Historically, the mortality rate for AFE was as high as 86%, whereas contemporary data show mortality from 13% to 23%.1
Early V-A ECMO centrifugal pumps and oxygenators caused significant blood trauma. Since the mid-2000s, improved pump and oxygenator technology has lowered bleeding complications and allowed V-A ECMO without systemic anticoagulation, renewing interest in extracorporeal support in AFE.4,5 To estimate the survival rate and complications of AFE patients undergoing V-A ECMO, we assessed the outcomes of all cases of AFE managed with V-A ECMO in the ELSO registry.
Materials and MethodsAll patients from the ELSO Registry with AFE receiving V-A ECMO from 2016 to 2021 were included. Baseline patient demographics, including age, ethnicity, and country of hospitalization, were included. The primary diagnosis, duration of V-A ECMO support, the reason for discontinuation, in-hospital complications, and discharge location were recorded.
The variables were summarized using counts (%) for categorical and medians (interquartile range [IQR]) for continuous variables. The incidence of complications was compared using Fisher’s exact tests. The analysis was performed in R 4.1 in RStudio 2022.07.1 environment (RStudio PBC).
ResultsA total of 34 patients received V-A ECMO for AFE. The median age was 32.5 years (IQR 29.5–37.3). Two-thirds of patients received care in the United States. The most common ethnicity was white (53%), followed by Asian (24%), black (15%), and Middle Eastern, North African, and Native Pacific Islander (2.9% each) (Table 1).
Table 1. - Baseline Characteristics and Outcomes Variable N = 34* Baseline characteristics Age 32.5 (29.5, 37.3) Female 34 (100) BMI 31 (26, 35) Ethnicity Asian 8 (24%) Black 5 (15%) Middle Eastern or North African 1 (2.9%) Native Pacific Islander 1 (2.9%) Unknown 1 (2.9%) White 18 (53%) Location The United States 22 (65%) Non-United States 12 (35%) Reason for discontinuation Died or poor prognosis 10 (29%) ECLS complication 3 (8.8%) Expected recovery 21 (62%) Survived 21 (62%) Discharge location N = 21* Transfer to LTAC or Rehab 7 (33.6%) Home 10 (48%) Transferred to another hospital 1 (4.8%) Other/unknown 3 (14%) Outcomes Died (n = 13) Survived (N = 21) p CPR required 1 0 0.806 Inotropes while on ECLS 1 1 0.691 Thrombus in V-A ECMO circuit 1 0 0.806 Tamponade 1 1 0.691 Canulation site bleeding 0 1 0.806 Disseminated intravascular coagulation 1 0 0.806 Moderate or severe hemolysis 0 2 0.691 Brain death 3 0 0.092 Diffuse CNS ischemia 2 0 0.270 Renal replacement therapy 5 5 0.600*Median (IQR); n (%).
BMI, body mass index; CNS, central nervous system; CPR, cardiopulmonary resuscitation; ECPR, extracorporeal cardiopulmonary resuscitation; ECLS, extracorporeal life support; IQR, interquartile range; LTAC, long-term acute care; V-A ECMO, veno-arterial extracorporeal membrane oxygenation.
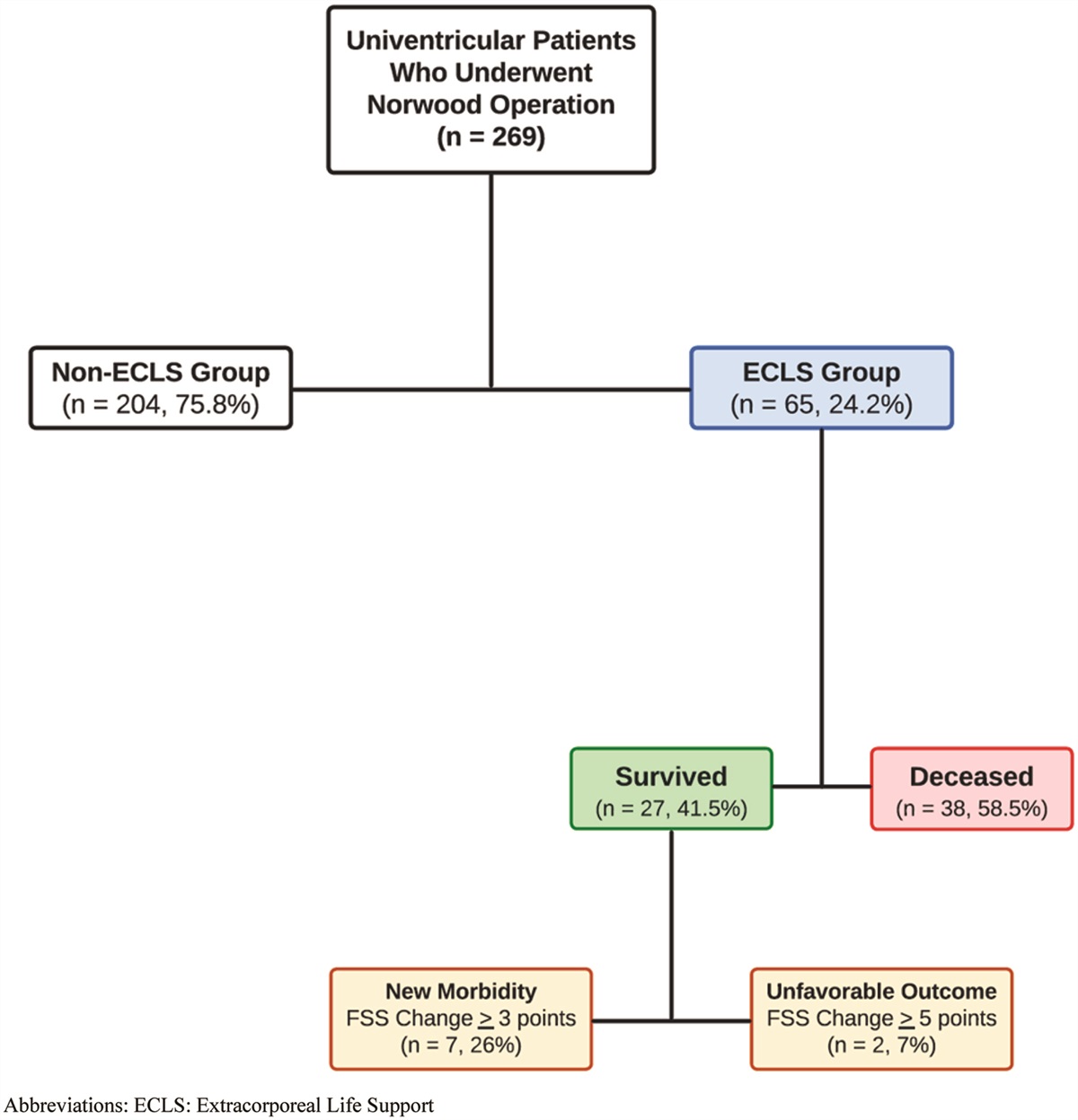
Thirteen patients (38%) died, and 21 patients (62%) survived to discharge. There was no difference in the mortality rate between the US and non-US patients (66.7% vs. 59.1%, p = 0.950). There were no differences in the incidence of complications between patients that survived and those that died. Among the surviving patients, 33.6% were transferred to a rehab facility, and 48% were discharged home (Figure 1).
 Figure 1.:
Figure 1.: Study design and results. V-A ECMO, veno-arterial extracorporeal membrane oxygenation.
DiscussionMaternal mortality in the United States is rising, and morbidity and mortality for AFE remain high.1 As cardiac arrest is a hallmark of AFE and current guideline recommendations support prompt multidisciplinary attention to hemodynamic support, V-A ECMO is an option for refractory cardiovascular collapse.
AFE involves thromboplastin activation, which induces hemostasis. This can cause microvascular thrombosis in the pulmonary vascular bed leading to increased pulmonary vascular resistance and cardiogenic shock. Simultaneously, consumptive coagulopathy and fibrinolysis can cause disseminated intravascular coagulation (DIC) and increase the bleeding risk.
Historically, the combination of cardiovascular collapse and high bleeding risk made AFE a unique challenge for extracorporeal support, resulting in SMFM’s recommendation against its routine use. However, second-generation circuits are heparin-coated, which decreases the need for anticoagulation altogether.4,5 No anticoagulation is acceptable in specific clinical scenarios, such as AFE.6 One systematic review of overall bleeding incidence while on VV or V-A ECMO without anticoagulation found an overall bleeding incidence of 33%. The incidence of circuit thrombosis during anticoagulation-free ECMO was 13%, similar to historically reported rates with systemic anticoagulation.7
Regardless of the reason for extracorporeal support, patients requiring V-A ECMO in the peripartum period are a high-risk cohort. One study of all peripartum patients on V-A ECMO for any reason found a survival to discharge of 70%; a previous study of the ELSO Registry found that 64% of patients with peripartum cardiomyopathy undergoing V-A ECMO survived to discharge.8,9
Historical data on the maternal mortality rate for AFE vary widely. One national registry of 46 patients showed 61% maternal mortality, with neurologically intact survival in only 15% of women.10 The largest previously published case series on extracorporeal support for AFE supported its use, showing a 70% survival to discharge despite severe hemodynamic instability and DIC among 10 patients undergoing V-A ECMO for AFE.11 In our study, the incidence of tamponade, cannulation site bleeding, DIC, and hemolysis were all less than 20%. One patient had an intracircuit thrombus. We found a 62% survival to discharge for patients receiving V-A ECMO for AFE. Among survivors of AFE, 48% were able to discharge directly home.
Our study has important limitations. First, our power to detect differences in clinical outcomes for those who received V-A ECMO for AFE is limited due to our sample size. Second, the observational nature of our study increases the risk of selection and confounding bias. The degree of illness is a clear confounding variable. Patients undergoing V-A ECMO for AFE are more likely to be critically ill; therefore, the mortality found in our study is not generalizable to all comers with AFE. Third, one-third of our cohort received treatment outside the United States. Though there was no statistical difference in the mortality for patients who received care inside versus outside the United States, the impact of geographical differences in practice patterns and their impact on complications is unknown. Finally, our data only addressed the duration and complications of V-A ECMO support; data on the specific circuit settings and use of concomitant anticoagulation were unavailable. Our results, therefore, should be considered hypothesis-generating rather than definitive.
To our knowledge, this is the largest case series involving V-A ECMO use for AFE. We found a 62% survival to discharge for patients receiving V-A ECMO for AFE. Further studies addressing predictors of adverse outcomes in AFE patients undergoing V-A ECMO will help determine candidates for the omission of systemic anticoagulation and patients likely to benefit from extracorporeal support.
AcknowledgmentsWe thank the Amniotic Fluid Embolism Foundation and the Minneapolis Heart Institute Foundation for their support.
References 1. Kaur K, Bhardwaj M, Kumar P, Singhal S, Singh T, Hooda S: Amniotic fluid embolism. J Anaesthesiol Clin Pharmacol. 32: 153–159, 2016. 2. Pacheco LD, Saade G, Hankins GDV, Clark SL; Society for Maternal-Fetal Medicine (SMFM). Electronic address: [email protected]: Amniotic fluid embolism: diagnosis and management. Am J Obstet Gynecol. 215: B16–B24, 2016. 3. Neggers YH: Trends in maternal mortality in the United States. Reprod Toxicol. 64: 72–76, 2016. 4. McQuilten Z, Aubron C, Bailey M, et al.: Low-dose heparin in critically ill patients undergoing extracorporeal membrane oxygenation—the Help-ECMO pilot randomised controlled trial. Blood. 128: 3822–3822, 2016. 5. Wood KL, Ayers B, Gosev I, et al.: Venoarterial-extracorporeal membrane oxygenation without routine systemic anticoagulation decreases adverse events. Ann Thorac Surg. 109: 1458–1466, 2020. 6. Conde-Agudelo A, Romero R: Amniotic fluid embolism: An evidence-based review. Am J Obstet Gynecol. 201: 445.e1–445.13, 2009. 7. Olson SR, Murphree CR, Zonies D, et al.: Thrombosis and bleeding in extracorporeal membrane oxygenation (ECMO) without anticoagulation: A systematic review. ASAIO J. 67: 290–296, 2021. 8. Lankford AS, Chow JH, Jackson AM, et al.: Clinical outcomes of pregnant and postpartum extracorporeal membrane oxygenation patients. Anesth Analg. 132: 777–787, 2021. 9. Olson TL, O’Neil ER, Ramanathan K, Lorusso R, MacLaren G, Anders MM: Extracorporeal membrane oxygenation in peripartum cardiomyopathy: A review of the ELSO Registry. Int J Cardiol. 311: 71–76, 2020. 10. Clark SL, Hankins GDV, Dudley DA, Dildy GA, Porter TF: Amniotic fluid embolism: Analysis of the national registry. Am J Obstet Gynecol. 172: 1158–1167; discussion 1167, 1995. 11. Aissi James S, Klein T, Lebreton G, et al.: Amniotic fluid embolism rescued by venoarterial extracorporeal membrane oxygenation. Crit Care. 26: 1–8, 2022.
留言 (0)