
記住我








Diffusion magnetic resonance imaging (dMRI) tractography enables the in vivo visualization and quantification of major white matter tracts within the brain, primarily by leveraging the diffusion phenomenon of water molecules within white matter fibers.1 Given that dMRI tractography is among the few noninvasive tools that can construct 3-dimensional representations of white matter fibers in the brain, the collaboration between radiology and neurosurgery has resulted in successful clinical applications, particularly in preoperative planning for neurosurgery.2,3
Within presurgical planning in neurosurgery, dMRI tractography is used to map the functionally crucial white matter tracts near the lesion to be resected or the surgical path. As surgical harm to white matter tracts can result in permanent functional disability, tractography must accurately reproduce the actual white matter tracts. In the almost 25 years since tractography was initially proposed, there have been significant advancements in imaging, fiber direction estimation, and tracking methods, leading to a remarkable improvement in the precision of reproducing actual white matter tracts.4 In the field of neurosurgery, dMRI tractography has been widely used in preoperative planning for the resection of brain lesions (such as gliomas), epilepsy surgery, and functional neurosurgical procedures such as deep brain stimulation (DBS).5–7 Furthermore, tractography applications have demonstrated alterations in the normal white matter and structural connectivity of the entire brain, extending beyond the lesion site. Tractography also plays a significant role in optimizing stimulation sites and parameters to maximize therapeutic efficacy in functional neurosurgical areas such as DBS. Furthermore, recent evidence has observed the potential of white matter fiber tract segmentation using tractography as a direct target for DBS. These observations present novel avenues for the clinical implementation of tractography and can enable risk stratification and prediction for patients in the future.
This review intends to elaborate on cutting-edge tractography methodologies, encompassing acquisition, fiber direction estimation, tracking methods, and other related techniques, as well as their recent applications in preoperative planning. In addition, it will discuss the present challenges and future prospects for the use of state-of-the-art tractography in preoperative planning.
Diffusion MRI TractographyIn this section, we provide a brief overview of the data acquisition process, mathematical models used to estimate fiber distribution, and tracking algorithms necessary for dMRI tractography. Numerous comprehensive literature reviews can be accessed, encompassing recent publications specifically focused on the field of neurosurgery; so, we focus on the important issue of tractography reproducibility and limitations for its use in neurosurgery.
AcquisitionDiffusion-weighted imaging (DWI) is a technique that uses diffusion-sensitizing gradients to measure the diffusion of water molecules within a single voxel.8 Diffusion sensitization involves incorporating diffusion gradients into a pulse sequence, thereby reducing the MR signals in all spin diffusion that align with the gradient directions. Recent studies have indicated that the precision and reliability of tractography are significantly affected by the acquisition methodology and image quality, particularly the gradient strength (ie, the b-value), variation of b-values, and the number of gradient directions.9,10
The choice of diffusion sampling scheme is an important consideration in DWI acquisition because it impacts the estimation of the applicable fiber tracking model. Generally, more gradient directions, higher b-values, or the use of multiple b-values improves the angular resolution and accuracy of the fiber tracking estimation.11 One commonly used method in the clinical setting is the single-shell scheme, which acquires multidirectional diffusion signals using only a single b-value. The most typical imaging techniques that often assume for single-shell acquisition are diffusion tensor imaging (DTI),12,13 which requires at least 6 diffusion directions, and high angular resolution diffusion imaging,14 which can be accurately estimated with diffusion sampling along 20–30 axes at minimum.11 In contrast, a multishell scheme that samples multiple shells with different b-values or a q-space sampling scheme, as typified by diffusion spectrum imaging (DSI),15 is becoming the preferred choice, as it can methodologically distinguish different restricted diffusion and estimate the diffusion spectrum. Although these imaging settings can provide high angular resolution and signal-to-noise ratio (SNR), they experience long acquisition durations.
Single-shot echo planar imaging (EPI) is an imaging sequence in which all k-space data are collected after a single radiofrequency excitation pulse. Single-shot EPI has been commonly used in clinical practice; however, it induces spatial distortion due to B0 inhomogeneity and T2* decay.16 Multishot EPI differs from single-shot EPI because it collects data by dividing a region of k-space by multiple shots (ie, segments). Multishot EPI can improve the SNR and spatial resolution and reduce blurring and susceptibility distortions as it has less time for phase errors to accumulate. However, the high sensitivity of multishot DWI to the subject bulk motion associated with a relatively longer acquisition time causes severe ghosting artifacts without phase error correction,17 which prevents accurate tractography estimation. Parallel imaging, multislice or multiband imaging for EPI, and imaging techniques combining them have been developed to increase slice acceleration, improve SNR efficiency, and achieve reliable tractography reconstruction.18–20 These advanced strategies have largely improved the acquisition time and realized the use of the above approaches with a clinically realistic scan time. As these developments can bring about high angular and spatial resolution in DWI, they are expected to provide a novel technique and new insights into the field of brain tumors.
Estimation of Fiber DirectionIn the context of brain structure, the estimation of the white matter fiber trajectory through DWI is based on tractography, which involves the tracing of “virtual” fibers. By using DWI-based fiber tractography, it is possible to segment white matter bundles, enabling a detailed evaluation of individual white matter tracts.21 Growing evidence has indicated the anatomical accuracy of tractography techniques compared with tract-tracing connectivity data.22 Tractography involves the utilization of a microstructural model that accounts for the diffusion of water molecules, primarily restricted anisotropically by the axonal microstructure, including myelin, glial cells, and extracellular free water within a voxel. One significant drawback of DWI tractography is that it relies on indirect information and various assumptions to characterize axonal pathways. Therefore, it is crucial to always complement tractography with neuroanatomical expertise. Furthermore, the tensor model that fits the diffusion of water molecules for an ellipsoid estimates the direction of the densest fiber running in the focused voxel. However, in cases where fibers are heterogeneously aligned within a single voxel (ie, crossing, kissing, fanning, and bending fibers), the accurate estimation of tractography can be technically challenging with DTI. This is because a single ellipsoid model is unable to represent the complex fiber distribution within a voxel.23
Beyond technical limitations, the fiber orientation distribution function (fODF) was proposed as a robust approach to improve neurosurgical planning with tractography estimations. Compared with DTI, the fODF models methodologically have the advantage of more accurately depicting crossing fibers, making them more effective tools for visualizing complex fiber arrangements. The approaches to estimating the fODF include model-free approaches, such as DSI,15 q-ball imaging,24 and generalized q-sampling imaging,25 which account for the observed heterogeneous fiber geometry by directly estimating the empirical distribution of diffusion within a single voxel, and model-based constrained spherical deconvolution (CSD)26 assumes that the diffusion signals are represented as the spherical convolution of a single-fiber response function and fODF. Figure 1 shows that the fODF derived from CSD can delineate the complex fiber running at the areas where multiple fibers are intersected. This observation implies the potential advantage of fODF model-based tracking over the DTI-based tracking in capturing fiber crossings. Moreover, model-free methodologies, which typically require the acquisition of multiple diffusion directions, offer the advantage of being independent of specific model assumptions. Although the CSD method can represent fibers that do not actually exist due to the model fitting process, CSD can provide accurate fiber estimation within a clinically acceptable acquisition time,26,27 which is also applicable for dMRI acquired with b-value = 1000 s/mm2 and 20 diffusion sampling directions.28 Currently, there is a wide variety of tractography software suites available for these tracking models.27Table 1 presents a list of the widely used software tools along with their respective tracking models.
 FIGURE 1:
FIGURE 1: The results of fiber tracking using 2 fiber distribution models and 2 tracking methods. A, A coronal b0 image overlaid with tractography based on the fiber orientation distribution function (fODF) with constrained spherical deconvolution (CSD) combined with a probabilistic method (left panel) and the fODF models used on the tracking (right panel). B, A coronal b0 image overlaid with the tractography based on diffusion tensor imaging (DTI) combined with a probabilistic algorithm (B, upper left) and a deterministic algorithm (C, lower left) and ellipsoids of the DTI model used on the tracking (right panel).
TABLE 1 - Typical Softwares for Tractography Estimation and Their Overview DTI Software Available Tracking Models Main Purpose URL MRtrix3The tracking algorithm, an important step in the fiber tractography process, involves choosing between deterministic and probabilistic tractography based on how the fiber running direction from a starting point for tracking, the so-called seed location is determined.
The deterministic algorithm reconstructs the most plausible single fiber by tracing fixed directions of the maximum eigenvectors in DTI (ie, the fiber assignment by continuous tracking algorithm) or the peaks of each lobe in the fODF model from a seed voxel. Although deterministic tractography produces relatively fast results with high specificity due to the simplicity of its algorithm, it is limited by the complex neural architecture within a voxel, resulting in uncertainty.29 Conversely, probabilistic tractography involves randomly drawing streamlines based on the distribution of fiber orientations. This algorithm enables the depiction of more streamlines that possibly exist from a seed point30 and is usually considered superior for reconstructing individual white matter pathways.31
Deterministic and probabilistic tractography are 2 commonly used methods for reconstructing white matter pathways. Despite several studies comparing these methods using simulated data, anatomical tracing, and verification of the validity of patient data, pinpointing the superior method between the 2 remains debatable.32–35 Notably, one of the major challenges is the tradeoff between the increase of false-positives and false-negatives due to the reconstruction method choice. False-positives refer to the identification of connections that do not actually exist, whereas false-negatives represent the failure to detect true connections. Generally, although the deterministic approach produces relatively fewer incorrect connections, the probabilistic approach provides a more complete reconstruction of the correct connections. However, it should be noted that the probabilistic nature of probabilistic tractography based on the previously described fiber distribution models induces an increase in false-positive pathways, which can interfere with presurgical planning. Moreover, the accuracy of tractography can depend on the choice of process, including tracking parameters (eg, step size, angular threshold, terminating threshold, and interpolation method), seeding strategies, and the size and locations of the seed region of interest (ROI). The technical description of the tracking parameters is omitted in this study; however, many of these factors contribute to the sensitivity-specificity tradeoff of tractography (for more details, see Jeurissen et al36). Studies using tractography in neurosurgery have reported variability across the used algorithm and emphasized the need to account for the uncertainty associated with a choice of tracking parameters.37
Recently, attempts were made to achieve an apparently higher spatial resolution of white matter tracts near brain tumors by quantifying the density of estimated tractography, called track density imaging (TDI). Track density imaging potentially has a higher spatial resolution of fiber density and orientation and improves white matter visualization in patients with brain tumors (Fig. 2).38
 FIGURE 2: A case study of a patient in whom the directionally encoded color (DEC)-TDI map was the preferred choice over the DEC-FA map, with the most significant difference observed in raw rater scores (A, full axial view; B, zoomed-in peritumoral view). The resolution of the DEC-TDI map was found to be particularly useful in establishing a goal margin of resection. This indicates that the visualization of the tumor margin was the most important factor leading to the preference for the DEC-TDI map among the raters. The figure also illustrates the case of the only patient in whom the DEC-FA map was generally preferred over the DEC-TDI map (C, full axial view; D, zoomed-in peritumoral view). This preference was driven by the visualization of clinically relevant tracts in the peritumoral region; that is, areas of T1/T2 signal change, as demonstrated by the DEC-FA map. Adapted with permission from Sullivan et al.38ROI-to-ROI Tractography for Presurgical Planning
FIGURE 2: A case study of a patient in whom the directionally encoded color (DEC)-TDI map was the preferred choice over the DEC-FA map, with the most significant difference observed in raw rater scores (A, full axial view; B, zoomed-in peritumoral view). The resolution of the DEC-TDI map was found to be particularly useful in establishing a goal margin of resection. This indicates that the visualization of the tumor margin was the most important factor leading to the preference for the DEC-TDI map among the raters. The figure also illustrates the case of the only patient in whom the DEC-FA map was generally preferred over the DEC-TDI map (C, full axial view; D, zoomed-in peritumoral view). This preference was driven by the visualization of clinically relevant tracts in the peritumoral region; that is, areas of T1/T2 signal change, as demonstrated by the DEC-FA map. Adapted with permission from Sullivan et al.38ROI-to-ROI Tractography for Presurgical Planning
The primary application of tractography in neurosurgery is to visualize the anatomy of the white matter tracts adjacent to the target lesions during surgery. The typical seeding approach involves whole-brain seeding, which randomly starts tracing from voxels in the brain parenchyma without the ROI. However, this may not always be reasonable for clinical use, given the increase in processing time and the inability to estimate tractography with target-specific parameters such as tract length, location, and pathology.39 ROI-to-ROI tractography enables experts to improve the processing time and to impose anatomical constraints on tractography delineation with strategically defined expert ROIs based on a priori knowledge (Fig. 3, eg, when delineating the tractography of the corticospinal tract [CST]), the seed and the target ROIs are generally defined on the cerebral peduncle and sensorimotor cortex, respectively, and the exclusion ROIs are placed on a midsagittal slice to remove the false-positives that run across the midline.40 However, note that the variability of the reproducibility induced in the manual placement of ROIs. It is particularly difficult to reproduce tractography reconstruction in the presence of brain tumors because the white matter integrity is compromised. One study demonstrated the relatively low reliability for ROI placement (κ = 0.300) by assessing the interrater reliability by 3 raters with different competence levels.41 This result suggests that the reproducibility of fiber tracking might be dependent on the expert's technique. To improve reproducibility, some techniques have been proposed to automatically extract tractography corresponding to target white matter tracts or the seed/target ROIs42,43; however, no criterion standard has yet been established for presurgical guides due to the presence of tumors. In addition to the ROI-to-ROI approach, other techniques are used for reconstructing white matter fiber bundles. These techniques are discussed under tractography in the DBS section.
 FIGURE 3:
FIGURE 3: Schematics of tracking strategies depict the approach of using regions of interest (ROIs) to perform ROI-to-ROI tractography. The illustration features 4 distinct white matter tracts, each in a different color, with intricate fiber arrangements that include overlapping, crossing, and kissing patterns as shown in panel A. To reconstruct the white matter tract highlighted in blue as an example of the corticospinal tract, ROIs that assume the seed or target masks (orange) and multiple exclusion masks (gray) are strategically defined based on a prior anatomical understanding of all 4 white matter tracts as shown in panel B.
Clinical Applications of Tractography in NeurosurgeryBesides safeguarding the eloquent cortex, it is crucial to shield the subcortical white matter connections against surgical harm to avert neurological harm after neurosurgery. Diffusion MRI tractography confers preoperative planning of surgical interventions with a noninvasive 3D visualization of white matter tracts. In the domain of neurosurgery, dMRI tractography is extensively used for the preoperative planning of the resection of brain lesions such as gliomas, vascular anomalies, and epilepsy surgery. Moreover, in recent times, tractography has been shown to be beneficial for the preoperative planning of functional neurosurgery, including DBS and focal ultrasound. This chapter reviews the latest developments in the clinical implementation of tractography in glioma, epilepsy, and functional neurosurgery (DBS), emphasizing patient prediction and its correlation with clinical functional assessments.
Conversely, it is essential to acknowledge the significance of conventional structural MRI sequences and functional MRI in preoperative planning. Conventional structural MRI sequences, such as T1-weighted, T2-weighted, gadolinium contrast-enhanced T1-weighted images, and fluid-attenuated inversion recovery images, play a crucial role in understanding the relationship between the lesion and adjacent brain normal structures. These images provide insights into the extent of the lesions and presence of surrounding edema and approximate proximity of the lesion to relevant brain regions. Furthermore, they are instrumental in assessing tumor characteristics, such as cysts, hemorrhage, and calcification, and identifying pathologically high-grade tumor components with gadolinium-enhanced contrast.
In addition, task-based functional MRI offers advantages in identifying eloquent cortical areas implicated in language and sensorimotor systems. Indirect measurement of task-induced neuronal activity via blood oxygen level-dependent signal during the performance of specific tasks compared with baseline conditions enables the detection of individual differences in brain functional anatomy and reorganization of functional anatomy caused by lesions.44–47 This is particularly relevant regarding delineation of the white matter tract anatomy, including any disruptions or deviations from the original trajectory of the tract near the lesion. Altogether, it is important to note that both conventional structural MRI sequences and fMRI are essential for preoperative planning, although they face significant challenges in accurately delineating the anatomy of the white matter tracts.
Tractography in Surgical Planning for GliomasAs the total removal of visible lesions is the most significant prognostic factor after glioma surgery, preoperative planning must prioritize the safe maximization of the extent of resection. Tractography is a noninvasive tool that visualizes the trajectories of functionally critical white matter fiber tracts near the tumor, enabling the identification of the safest pathways for maximal resection while preserving these tracts.48 In other words, tractography balances functional preservation and resection extent in glioma surgery and has demonstrated its utility in preoperative planning. For example, Romano et al49 investigated the usefulness of tractography in 28 patients with gliomas near the pyramidal tract (motor), optic radiation (visual), and arcuate fasciculus (AF; speech) using the ROI-to-ROI method with DTI-based deterministic tractography. Their results demonstrated that visualizing the 3-dimensional relationship between the tumor and tractography location changed the surgical approach to cortical incision in 6 patients (21%) and impacted intraoperative resection margin determination in 18 patients (64%) without exacerbating symptoms in most cases (96%).49 Also, in a recent report, 5 neurosurgeons scored the effectiveness of TDI and traditional color-coded FA maps on items such as the identification of white matter tracts near the tumor, the establishment of tumor resection margins, and the determination of the planned surgical route. The color-coded TDI map scored significantly higher than the traditional color-coded FA map for both questions, with the largest effect size being in the score for establishing target resection margins.38
The identification of the invasion of indistinct white matter tracts distant from the lesion in glioblastoma poses a challenge to the determination of the extent of resection.50 The recognition of such invasions is crucial as they can lead to recurrence; however, the accurate identification of their extent is often challenging.51 Tractography has demonstrated potential in identifying invasion.5 For example, Kis et al5 evaluated the effectiveness of preoperative probabilistic tractography using various thresholds in predicting the site of postoperative recurrence in 20 patients with high-grade glioma (Fig. 4). Their findings revealed that probabilistic tractography can predict the site of recurrence, with 81% sensitivity and 90% specificity.5 Moreover, Wei et al52 used probabilistic tractography and connectome analysis to demonstrate that glioblastomas result in impairments of normal-appearing white matter beyond focal lesions and that these impairments are associated with poor preoperative performance, cognitive dysfunction, and worse survival.52 These results suggest that tractography may prove useful in facilitating more precise treatment planning and patient stratification.
 FIGURE 4: The primary tumor, the recurrence tumors along with the overlap between different tumor connections (TCs), and the tumor recurrence mask for patient 20. A, The preoperative contrast-enhanced T1-weighted image showing 2 small tumors with ring-shaped contrast enhancement in the right frontal region. B, The size and location of tumor recurrence. C–E, The 1%, 5%, and 40% TCs (in red, blue, and red-yellow, respectively), respectively, overlapped on the tumor recurrence mask (in green). These images correspond to the preoperative T1 images. Notably, the TCs show complete overlap with the tumor recurrence mask, resulting in 100% specificity at every threshold. However, the recurrence significantly exceeds the border of the TCs, leading to low (as low as 1%) sensitivity. It is worth mentioning that the recurrence direction is in line with that of the TCs, and the low sensitivity is attributed to the fast tumor progression. Adapted with permission from Kis et al.5
FIGURE 4: The primary tumor, the recurrence tumors along with the overlap between different tumor connections (TCs), and the tumor recurrence mask for patient 20. A, The preoperative contrast-enhanced T1-weighted image showing 2 small tumors with ring-shaped contrast enhancement in the right frontal region. B, The size and location of tumor recurrence. C–E, The 1%, 5%, and 40% TCs (in red, blue, and red-yellow, respectively), respectively, overlapped on the tumor recurrence mask (in green). These images correspond to the preoperative T1 images. Notably, the TCs show complete overlap with the tumor recurrence mask, resulting in 100% specificity at every threshold. However, the recurrence significantly exceeds the border of the TCs, leading to low (as low as 1%) sensitivity. It is worth mentioning that the recurrence direction is in line with that of the TCs, and the low sensitivity is attributed to the fast tumor progression. Adapted with permission from Kis et al.5The implementation of appropriate tractography techniques is crucial in preoperative planning for neurosurgery. Advanced tractography models and methods have demonstrated potential in improving the depiction of white matter fiber bundles surrounding tumors compared with traditional deterministic tractography based on DTI, which has traditionally been used for preoperative planning. For instance, CSD-based probabilistic tractography has been shown to accurately depict the fanning of CST from the brainstem to the anterior central region in patients with gliomas compressing CST, surpassing DTI-based deterministic tractography.53 In addition, it has been reported that CSD-based probabilistic tractography can better assess CST damage than DTI-based deterministic tractography in patients with gliomas experiencing postoperative motor deficits.54 Furthermore, the bicompartmental free water modeling algorithm can now exclude the effects of edema from the tissue by estimating the quantity of extracellular free water in the voxel using a bicompartmental model.55 This technique can precisely delineate tractography even when edema is strong in the peritumoral white matter.56 However, there is limited research on the practical application of such technology, and there is a paucity of evidence of its use in real-world neurosurgical practice.
Tractography in Epilepsy Surgical PlanningTemporal lobe resection is an effective surgical intervention for refractory temporal lobe epilepsy (TLE). However, it entails the potential hazard of postoperative visual and linguistic dysfunction in operated patients.6 In the preoperative planning of epilepsy, dMRI tractography is frequently used to avert such complications.
Precisely, it is crucial to avoid any injury to the Meyer loop and optic radiations to forestall any visual field deficits. It has been documented that contrasting the Meyer loop/optic radiations (as delineated by tractography) with the extent of resection can anticipate the risk of postoperative visual field deficits.57–60 For instance, Taoka et al58 used deterministic tractography based on DTI to visualize the Meyer loop in 14 patients who underwent temporal lobectomy for TLE. They found that the distance from the temporal tip to the anterior edge of the Meyer loop differed significantly among individuals (30.0–43.2 mm).58 Furthermore, the distance between the anterior edge of the Meyer loop and the posterior limit of temporal lobectomy correlated significantly with the severity of visual field deficits.58 In addition, Yogarajah et al59 reported that the distance from the tip of the Meyer loop to the temporal pole was a significant predictor of postoperative visual field loss.
It has become increasingly evident that the choice of tracking algorithm plays a crucial role in the accurate depiction of the Meyer loop using tractography. The arduous nature of the task of reproducing Meyer loops with substantial curvature using DTI-based deterministic tracking often results in an underestimation of their actual extent.61 In contrast, probabilistic tractography has been found to represent Meyer loops with greater precision compared with DTI-based deterministic tractography.62,63 Among various probabilistic methods, CSD tractography has been reported to be both quicker and more accurate than ball-and-stick tractography and to exhibit a superior correlation with established anatomical landmarks.63
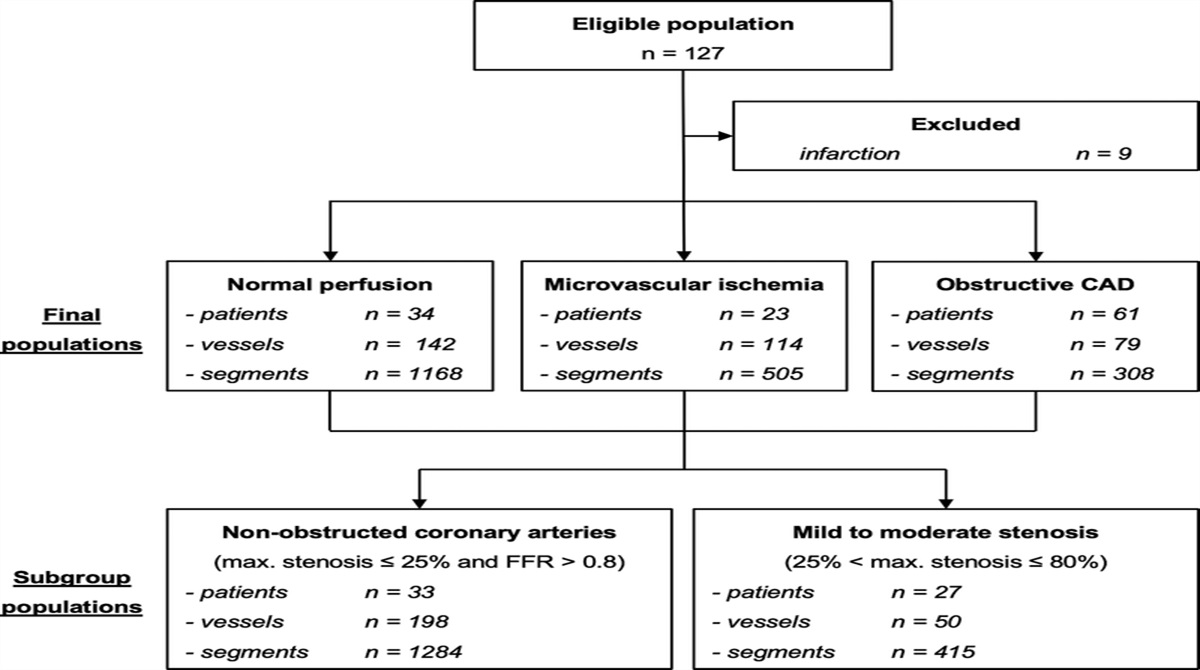
The relationship between language function and white matter tracts is intricate as there exist multiple white matter structures linked to language function. Nonetheless, the prediction of postoperative language dysfunction is crucial because patients whose language-dominant hemispheres are resected have a substantial risk (ranging from 30% to 50%) of experiencing a decline in their language-related function after the surgical procedure. For instance, Binding et al64 used probabilistic tractography to map language-related white matter tracts (such as the AF, uncinate fasciculus, inferior longitudinal fasciculus, middle longitudinal fasciculus, and inferior fronto-occipital fasciculus) in 127 patients undergoing TLE surgery to explore the correlation between postoperative language function assessment and the percentage of white matter tracts impaired by the surgery. According to their findings, in language-dominant hemispherectomy, the greater the surgical damage to the AF and inferior fronto-occipital fasciculus, the worse the language function at 3 months. Moreover, Caverzasi et al65 reported that AF preservation, which was mapped by tractography, was significantly associated with the absence of postoperative language deficits. Furthermore, there is already evidence suggesting a functional language outcome benefit of performing tractography as part of the preoperative planning for epilepsy surgery.
The use of tractography in clinical settings for patients diagnosed with TLE not only facilitates the identification of crucial white matter tracts that require surgical protection but may also help to identify network abnormalities across the brain beyond the hippocampus and temporal lobe.66,67 Notably, studies have demonstrated that a more pronounced alteration in the whole-brain structural network constructed via dMRI tractography corresponds to a greater likelihood of seizures persisting after TLE surgery.68 In addition, the entire cerebral structural network is found to be larger and more extensively altered in patients diagnosed with TLE, who experience focal-to-bilateral tonic-clonic seizures, which represent the most severe form of epileptic seizures and serve as a poor prognostic factor for seizure freedom after temporal lobectomy.68 Structural network evaluation using tractography has also demonstrated greater predictive power for memory impairment in TLE than the hippocampal volume or other clinical measures.69 Furthermore, studies have revealed compromised short-range white matter network connections in patients with epilepsy. Lower U-fiber counts obtained with probabilistic tractography were found in patients with epilepsy than in healthy controls.70 Among children diagnosed with benign epilepsy with centrotemporal spikes, abnormal maturation characterized by increased FA was observed in perirolandic U-fibers, which was correlated with poorer fine motor performance.71 Based on the findings of these studies, a structural network assessment using tractography could serve as a valuable marker for patient stratification and prediction.
Tractography in Deep Brain StimulationDeep brain stimulation is a well-established neurosurgical procedure that entails the insertion of electrodes targeting specific brain regions and the administration of continuous or periodic electrical impulses from an implanted battery-powered device. Deep brain stimulation has emerged as a treatment option for patients with motor circuit disorders, such as Parkinson disease (PD), dystonia, and essential tremor, or psychiatric disorders (ie, obsessive-compulsive disorder [OCD] and major depressive disorder) who are not responding to other forms of treatment.72
Adverse effects may emerge over time and negatively impact DBS treatment outcomes, likely due to suboptimal electrode placement and the current spread to adjacent structures. Tractography presents a promising methodological opportunity to optimize electrode implantation and stimulation parameters for DBS.7 Although early views suggested that DBS solely inhibited the neural activity in the region that was stimulated,73 it is currently widely acknowledged that DBS can have intricate effects on extensive brain areas.74 Previous research indicates that DBS primarily stimulates axons rather than cell bodies.75 Hence, white matter tracts in close proximity to the deep nuclei (Fig. 5A) may hold greater significance for the therapeutic effects of DBS, increasing the focus on targeting white matter bundles visualized using tractography.
 FIGURE 5: A, This image displays directionally colored diffusion MRI tractography of the dentatorubrothalamic tract (DRT), which connects several regions, including the dentate nucleus of the cerebellum, the red nucleus, the ventral intermediate thalamus, and the motor cortex. It is worth noting that there is no midline crossing in the midbrain, which is a drawback of the DTI technique. B, The tract proximity analysis involves measuring the distances between the DRT (blue) and the deep brain stimulation (DBS) electrode (red) to evaluate treatment outcomes. C, Tract activation modeling generates fiber tracts (yellow) from a region of interest surrounding the DBS contacts (red). D, Direct tract targeting (DTT) utilizes the diffusion tractography model of the DRT (red) for preoperative DBS electrode targeting. Adapted with permission from Calabrese.76
FIGURE 5: A, This image displays directionally colored diffusion MRI tractography of the dentatorubrothalamic tract (DRT), which connects several regions, including the dentate nucleus of the cerebellum, the red nucleus, the ventral intermediate thalamus, and the motor cortex. It is worth noting that there is no midline crossing in the midbrain, which is a drawback of the DTI technique. B, The tract proximity analysis involves measuring the distances between the DRT (blue) and the deep brain stimulation (DBS) electrode (red) to evaluate treatment outcomes. C, Tract activation modeling generates fiber tracts (yellow) from a region of interest surrounding the DBS contacts (red). D, Direct tract targeting (DTT) utilizes the diffusion tractography model of the DRT (red) for preoperative DBS electrode targeting. Adapted with permission from Calabrese.76There are a few common methods used in the application of tractography to DBS patients. Specifically, tract activation modeling, tract proximity analysis (TPA), and direct tract targeting (DTT) were used (Fig. 5). A detailed review of these methods has been presented before.76 In brief, TPA (Fig. 5B) involves analyzing the placement of DBS contacts in relation to a particular tract of interest retrospectively.76 This technique can be used to determine whether the proximity of a contact to a specific tract is associated with treatment effectiveness and also to look back on the accuracy of electrode targeting. Tract activation modeling (Fig. 5C) combines tractography and electric field models to predict direct axonal activation in response to specific DBS parameter settings in the patient. This method helps identify stimulation sites and parameters at the individual patient level. It achieves this by seeding tractography from the region surrounding previously implanted DBS electrodes, called the volume of tissue activated (VTA) that triggers critical fiber tracts known to mediate treatment response based on the stimulation parameter settings and the anatomical structures within the target area. Finally, DTT involves the direct placement of DBS electrodes on specific target tracts identified through tractography.76
The subthalamic nucleus (STN) has been the primary target for DBS in PD as it is a crucial structure that plays a role in the development of PD motor symptoms.77 The globus pallidus internus (GPi) is also a commonly used target in PD. However, STN stimulation has been shown in previous studies to have a more significant impact on the reduction of motor symptoms and also the reduction of the dose of dopaminergic agents.78,79 According to a recent meta-analysis, STN-DBS also has a considerable positive impact on several PD nonmotor symptoms, such as sleep disturbances, memory impairment, and urinary symptoms.80 Some recent studies suggest cortico-subthalamic pathways, particularly those associated with superior frontal structures, as potential neuromodulation targets that could be beneficial for the management of PD.81,82 Vanegas-Arroyave et al82 investigated the distinct connectivity patterns that characterize effective electrodes in patients with PD treated with STN-DBS. They used VTA as an ROI and applied probabilistic tractography to determine the number of tracts from each VTA at entry voltage to GM ROIs. The study revealed that the white matter tracts surrounding STN, which are connected to the superior frontal gyrus and the thalamus, are crucial in the mechanism of action of STN-DBS for PD. There are various ways in which antidromic spikes can contribute to the therapeutic benefits of STN-DBS. One way is by activating motor targets of cortical neurons through the branching point and traveling down axon collaterals. Another way is by affecting the local circuitry, including inhibitory neurons, through the invasion of antidromic spikes into projection neurons.81 Indeed, it has been shown that STN-DBS has a direct effect on intracortical neurons, which can alter the balance between excitation and inhibition.83 Furthermore, using TPA, Said et al84 found a tendency for contact voltage tolerance thresholds to increase as the distance from the CST increases. The CST was segmented using the posterior limb of the internal capsule and cerebral peduncle as seeding regions. Sweet et al85 also found a tendency toward better tremor control in patients with PD when the DBS electrodes were placed closer to the dentatothalamic tract (obtained using ipsilateral subthalamic and red nuclei) and contralateral cerebellar hemisphere as seeding ROIs.
In cases of intractable dystonia, the posteroventral lateral GPi has now become the most widely recognized target for DBS. Although GPi stimulation has been shown to significantly improve various dystonia symptoms with minimal adverse effects, it is most effective in isolated dystonia and not in combined dystonia.86,87 Furthermore, Rozanski et al88 proposed the pallidothalamic tracts, a major efferent fiber bundle of the GPi,89 as a DBS major target in dystonia. In this study, the pallidothalamic tract was reconstructed via probabilistic tractography using GPi and thalamus masks obtained via the use of FSL atlas tools as ROIs.88 Their results indicated close anatomical proximity of clinically efficient DBS electrodes placed in the GPi and the pallidothalamic tracts, particularly the ansa lenticularis, in patients with dystonia.88
Deep brain stimulation treatment in patients with essential tremors targets the ventral intermediate nucleus (VIM) of the thalamus.90 The posterior subthalamic area was also indicated as a potential target to suppress tremors with lower stimulation amplitudes.91 Moreover, dentatorubrothalamic tract (DRT) stimulation is an effective treatment modality for tremors.92,93 The DRT is a fiber bundle connecting the dentate nucleus of the cerebellum to the contralateral red nucleus, VIM, and motor cortex, which is involved in coordinating somatomotor function. It has been demonstrated that by stimulating the DRT at various points located above and below the midcommissural point, tremors caused by different factors (ie, PD, essential tremor, dystonic tremor, and multiple sclerosis) can be effectively relieved.94 To segment the DRT, a deterministic tracking approach was used, which involved using the midbrain as the starting seed region and the primary motor cortex and the dentate nucleus of the same side of the cerebellum as the inclusion ROIs.94 Calabrese et al95 used manual ROIs to reconstruct the DRT in postmortem human brains using the probabilistic tracking method. These ROIs consisted of the superior cerebellar peduncles, the red nucleus, and VIM, and a human brainstem atlas based on histology was used as a reference. Based on TPA, they found a significant association between treatment efficacy and contact proximity to DRT.
The stimulation of the anterior limb of the internal capsule was first suggested for treating OCD, making it one of the earliest psychiatric indications for DBS.96 A recent study demonstrated that bilateral DBS of the bed nucleus of the stria terminalis, which is a part of the limbic system, was effective in reducing symptoms in patients with severe, treatment-resistant OCD.97 A reduction in OCD symptoms was also observed after DBS in the associative/limbic part of the STN.98 Baldermann et al99 observed that white matter connectivity, reconstructed using VTA and a deterministic fiber tracking algorithm, from DBS electrodes to medial and lateral prefrontal cortices was related to a more pronounced relief of OCD symptoms. Furthermore, the neuromodulation of white matter fiber bundles connecting dorsal anterior cingulate and ventrolateral prefrontal cortices to the anterior medial STN was consistently associated with long-term clinical outcome improvement in 4 cohorts of patients with OCD treated with the anterior limb of the internal capsule–DBS or STN-DBS (Fig. 6).100 In line with the findings of previous research, Li et al100 also used the VTA as the starting point to create structural connections and considered all other regions of the brain as parts of a normative connectome. Furthermore, the tract calculated in one cohort could be used to cross-predict clinical improvement in another cohort.100
留言 (0)