Tuberous sclerosis complex is an autosomal dominant genetic disorder characterized by the formation of hamartomas in various organs such as the skin, brain, heart, lungs, kidneys, and liver [1]. It occurs sporadically in around two-thirds of patients [3]. De novo mutations result in the inactivation of the TSC1 gene located on chromosome 9q34.3 and the TSC2 gene located on chromosome 16p13.3, which are responsible for tuberin and hamartin production [3].
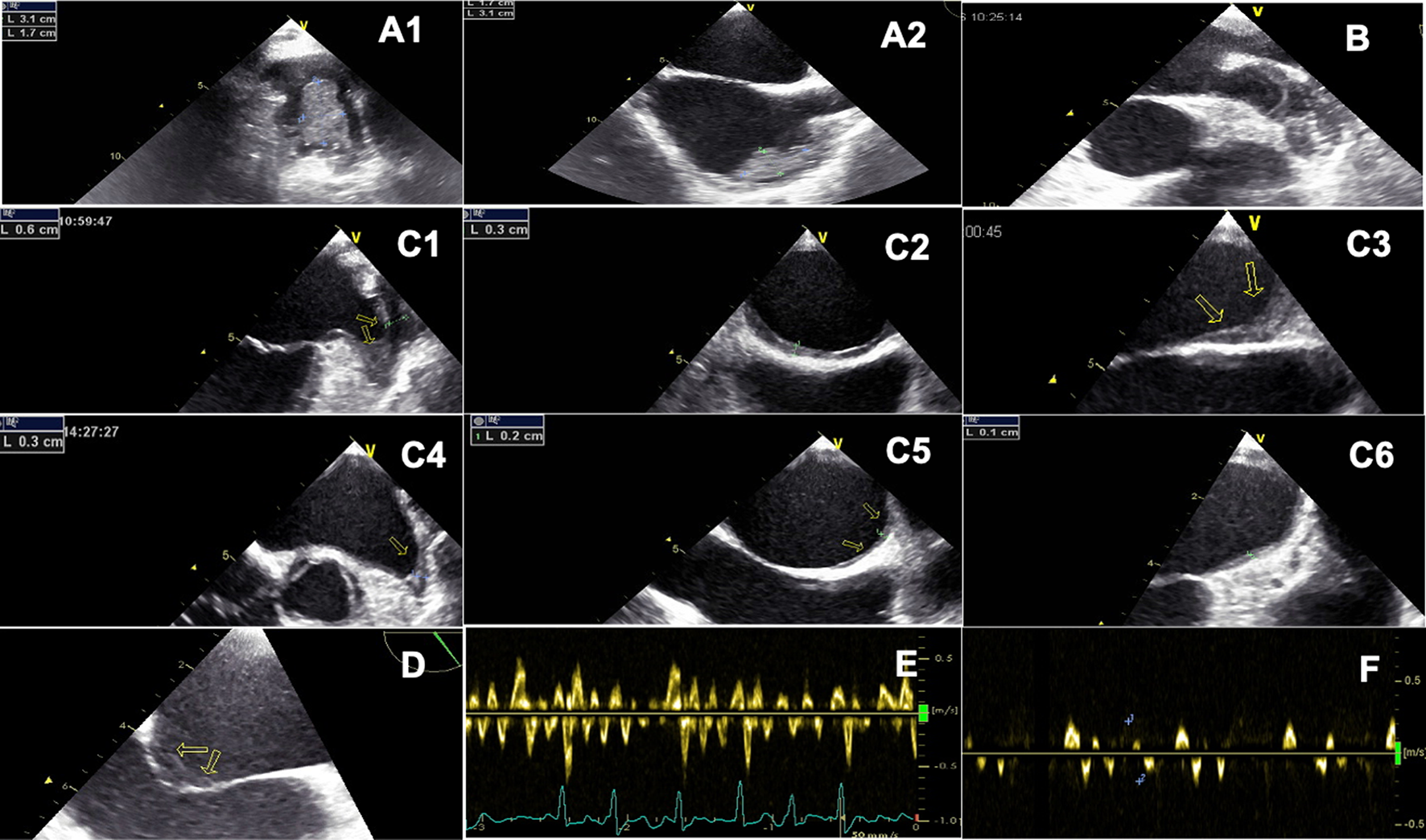
With a rare incidence of 0.2% [8], CRs are the most common type of benign cardiac tumors. CRs can occur spontaneously, in association with other congenital heart diseases, or in association with TSC [8], with approximately 60–80% of cases being linked to TS [2, 6, 9]. Józwiak et al. [4] examined 154 patients with TS and discovered that 74 (48%) of them had multiple CRs. These tumors were located in the right ventricle (35%), interventricular septum (33%), left ventricle (22%), left atrium (5%), and RA (5%). In our case, the RA, a rare location, contained a 25 × 20 mm rhabdomyoma (Fig. 2) that was later associated with TSC.
The clinical features of TSC consist of seizures, hydrocephalus, mental retardation, rhabdomyomas, renal angiomyolipomas, developmental delay, spine malformations, and skin angiofibromas [10]. CRs are usually multiple in more than 90% of cases [8], especially in the presence of tuberous sclerosis [11] and are typically asymptomatic. Nevertheless, arrhythmias, fatal outflow obstruction, and rarely myocardial infarction can occur in the womb [1]. ECGs can present a spectrum of different conduction defects, including tachycardia, bradycardia, ST segment changes, Wolff–Parkinson-White pre-excitation, and aberrant atrial or intraventricular conduction [12]. The prognosis depends on the size, location, and associated complications of the tumor [5]. Fetal cardiac tumors larger than 20 mm in diameter carry a higher risk of prenatal death [9]. In our scenario, the patient exhibited symptoms of irregular arrhythmias characterized by PACs in the presence of a solitary atrial mass; however, there were no signs of hemodynamic instability.
The diagnosis of rhabdomyoma can be determined through prenatal ultrasound or MRI during the third trimester of pregnancy or in the early neonatal period [1, 13]. Ultrasound findings typically show a round, uniform, hyperechogenic mass, primarily located in the ventricles [3]. Our echocardiography findings matched typical rhabdomyoma features. When considering the differential diagnosis, other potential conditions to consider are pericardial teratoma, fibroma, hemangioma, myxoma, and echogenic cardiac focus. The absence of pericardial effusion and prominent internal vascularity excludes teratoma and hemangioma. Differential diagnosis between the other tumors using ultrasonography alone is difficult [14]. However, given the patient’s family history and extracardiac findings that matched TSC, CR was the ideal clinical diagnosis.
The diagnosis of TSC relies on clinical criteria that are categorized as major and minor (Table 1) [15].
Table 1 Clinical criteria for diagnosing of tuberous sclerosis (2012)To confirm the diagnosis, at least two major criteria or one major and two minor criteria must be present. A probable diagnosis can be made with one major criterion or two or more minor criteria [15]. Our case fulfilled two major criteria: cardiac rhabdomyoma and subependymal brain lesions, and one minor criterion, renal cysts. However, genetic analysis was not conducted in our case. Our diagnosis was obtained after birth. It is crucial to prenatally diagnose rhabdomyomas in order to investigate any association with TSC and plan appropriate treatment early on.
Regarding the treatment and management of TSC, significant progress has been made with mechanistic target of rapamycin complex 1 (mTORC1) inhibitors leading the way [16]. If the tumor obstructs normal cardiac outflow or leads to intractable arrhythmias, surgical intervention becomes a necessity [11, 17]. Typical rhabdomyoma cells lose their ability to divide and gradually regress during early childhood [11]. Postnatal echocardiograms should be done for at least a year to monitor the regression phase of rhabdomyomas and ensure there are no additional health risks for the infant [9]. In our patient, the tumor did not restrict blood flow, and further examination after 9 months revealed a hemodynamically stable patient with a normal ECG, and echocardiography demonstrated tumor regression.

留言 (0)