This is the first study that assess by Bayesian approach the minimum effective dose of acetaminophen for patent ductus arteriosus in extremely preterm infants at 23–26 weeks gestation. This minimum effective dose was estimated to be 25 mg/kg followed by 10 mg/kg QID for 5 days. This is in agreement with a previous study that suggested that 10 mg/kg/6 h should be enough to treat PDA with no need to increase further the dose in preterm infants at 26 weeks gestation [12].
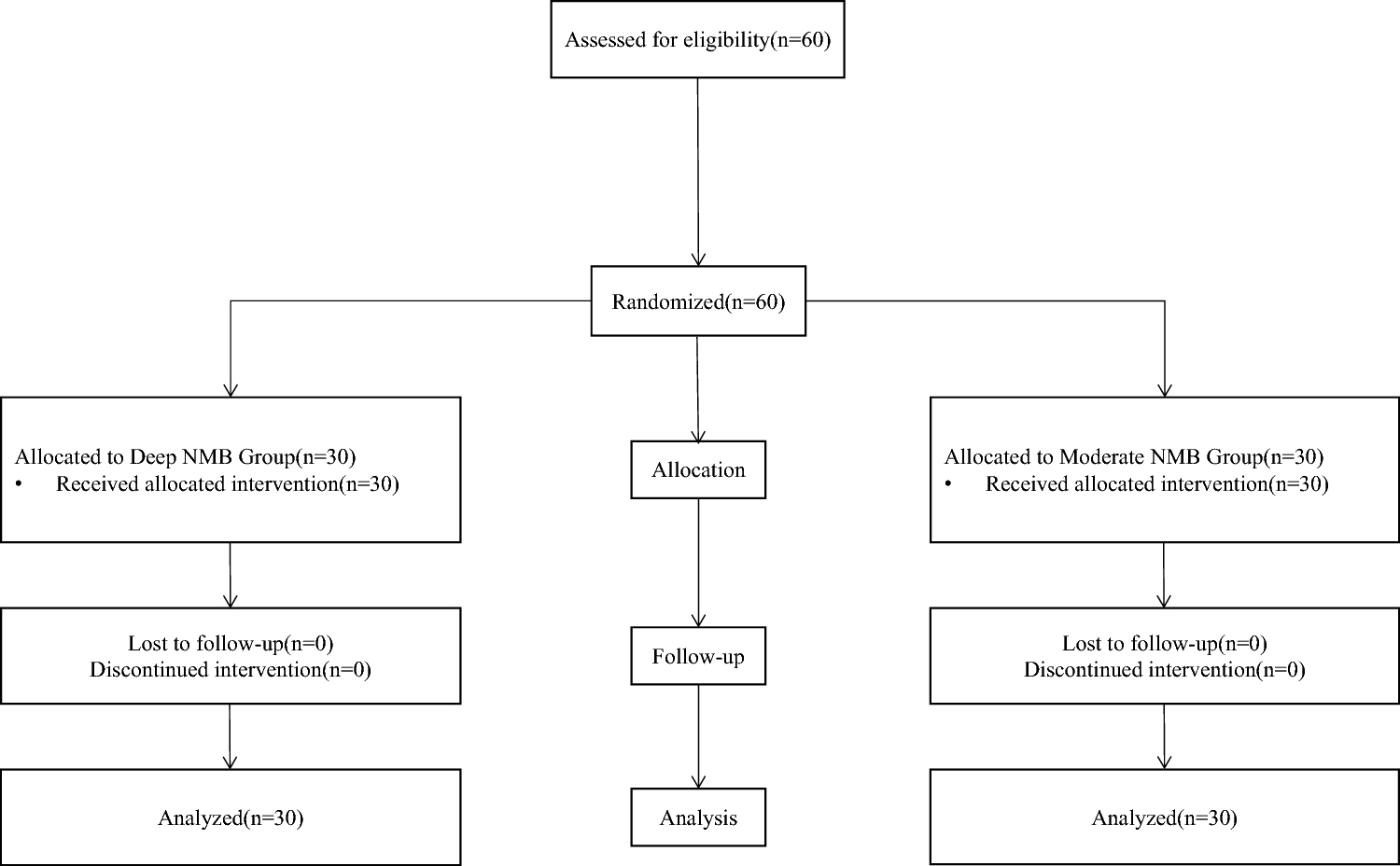
The continual reassessment methodology was preferred over a parallel group design because of the multiple advantages of this design especially in such vulnerable population. This sequential dose increases the approach to avoid unnecessary overexposure of these at-risk patients. This approach allows also the enrollment of fewer patients to determine the minimum effective dose response without requirement of a placebo group. Furthermore, a suboptimal range of acetaminophen doses can be pointed out earlier. Additionally, rather than considering each dose level as independent conditions, this approach allows for enriched data observation using prior beliefs and accounts for pharmacological assumption that each dose is interdependent. Due to the small sample size, considering that each dose level is not interconnected would lead to a range for the second dose level with a large uncertainty regarding the primary endpoint rate—33% with a wide 95% confidence interval, from 7.5 to 70.1%. The continual reassessment design allows for incorporation of overall cumulated successes in the trial, assuming a monotonic increase of the probability of success as dose level increases. This Bayesian inference allows for a posteriori estimate of success rate probability, along with its credibility/probability interval (PI) incorporating contextual information (see Supplementary Material text) with more informative estimations. The 95% PI estimation of success rate for the second dose level was narrower from 51.5 to 77.9%. A slight misbalance in gestational age, birth weight, and use of mechanical ventilation was observed between the two dose levels. However, none of these variables were significantly associated with treatment success, suggesting that no confounding effects of these variables should be considered in this extreme preterm cohort.
The rates of PDA in preterm infants at day 7 after birth was reported to be 68% in infants with gestational ages 25–26 weeks and rising to 87 % for 24-week-old infants [11]. Regarding these previous reported findings, the use of intravenous acetaminophen appears to decrease the PDA rate in these extremely premature infants. Interestingly, our results also show that prophylactic acetaminophen use allowed for patients to be considered as a “failure” (with the study primary criterion), with values close to the success patients for left pulmonary artery end-diastolic velocity and left atrium/aorta ratio. Additionally, the mean left atrium/aorta ratio was below 1.5 during the treatment time course for both success and failure patients (value considered as a cutoff to discriminate hemodynamically significant PDA) [13]. These observations strengthen the benefits of this prophylactic dose regimen on overall patients.
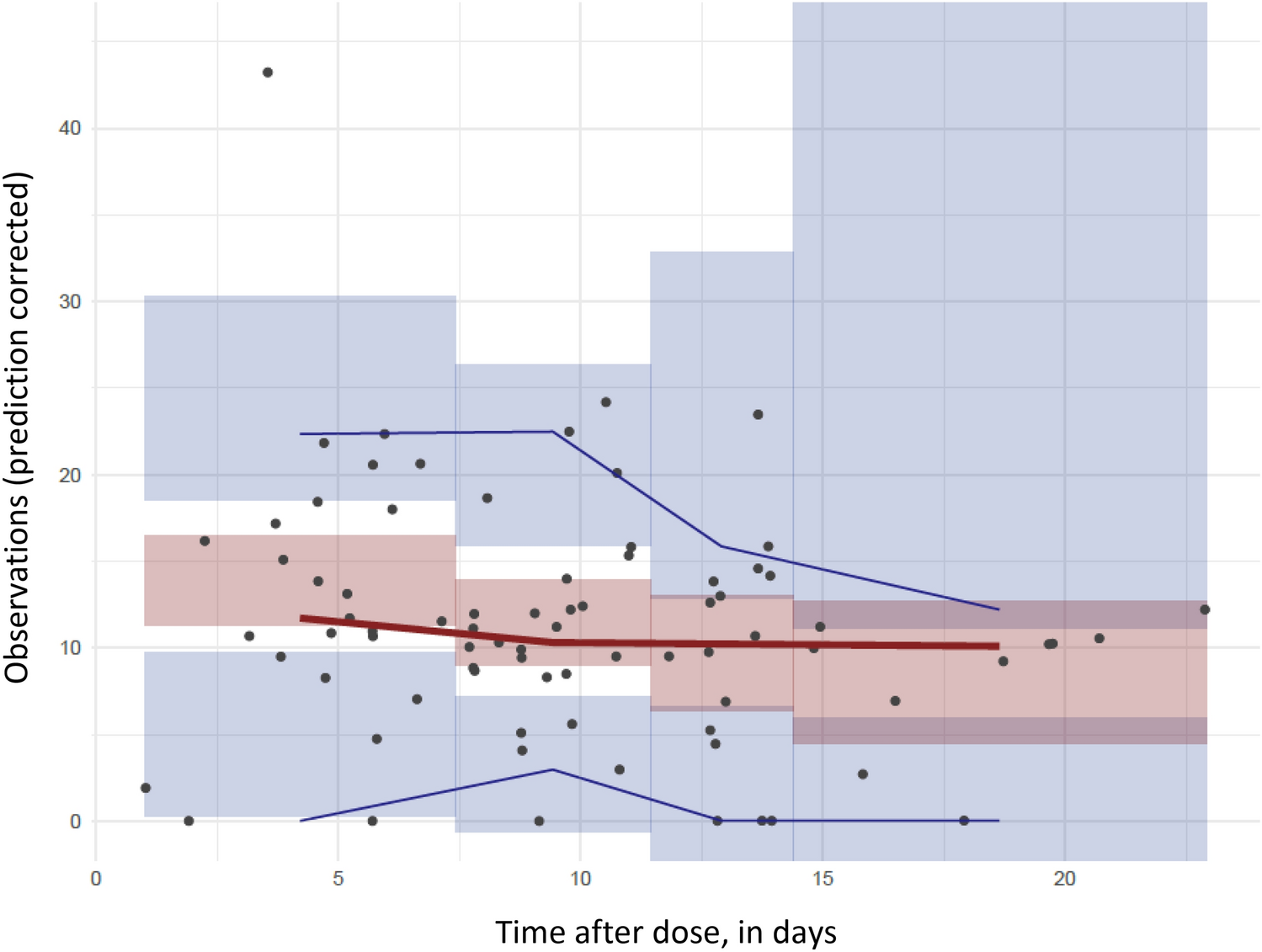
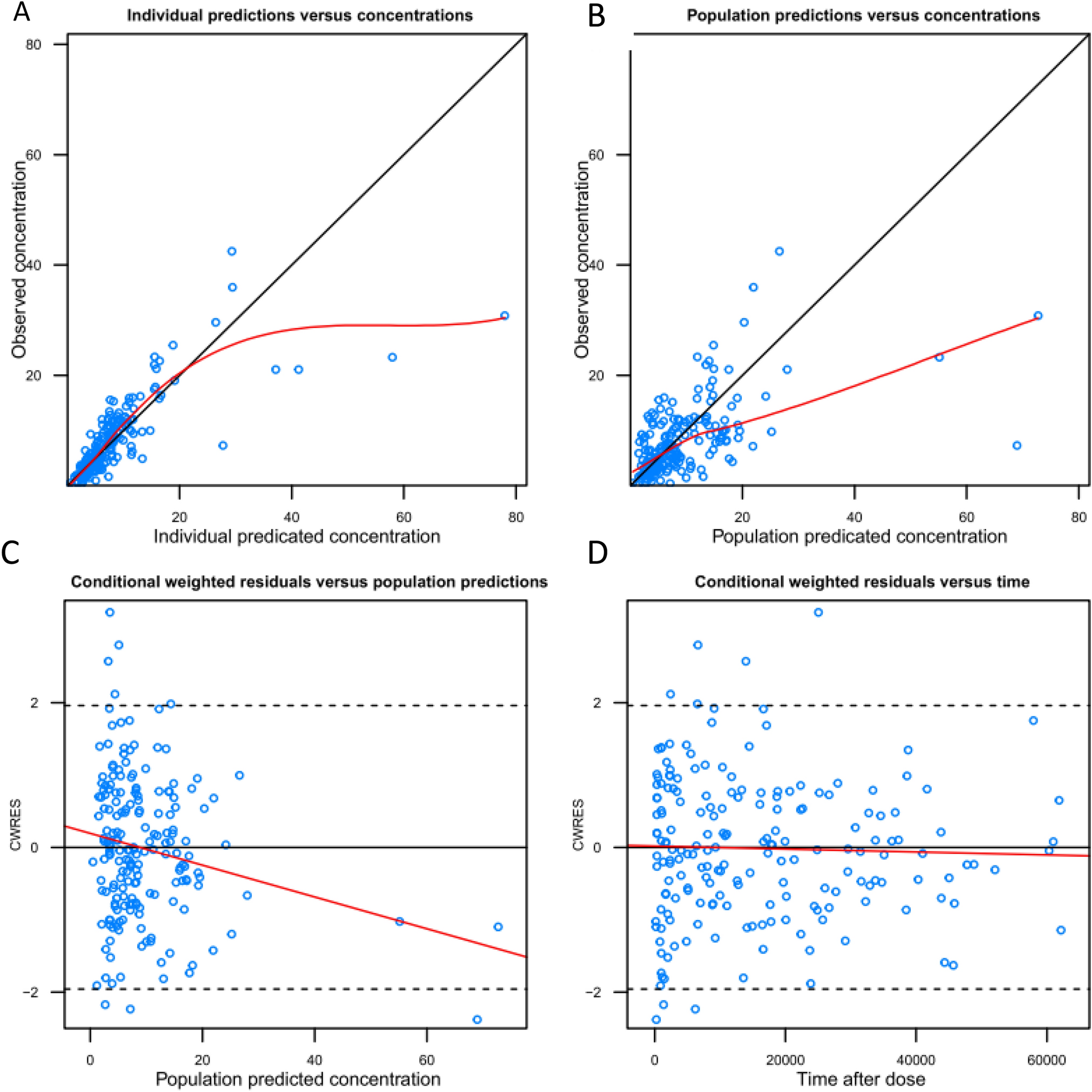
A marked variability of plasma acetaminophen and concentrations of its metabolites was observed between subjects after the loading dose. This is in agreement with a previous pharmacokinetic studies performed in a preterm population that reported high interindividual variabilities on both acetaminophen elimination clearance and volume of distribution [8, 14]. Plasma inactive metabolite levels measured after end-of-loading dose were higher in preterm infants in whom ductus closure was not observed, which can support also the use of the higher dosage proposed in dose level 2 overdose level 1. However, further specific pharmacokinetic studies are needed to better characterize the distribution and elimination of acetaminophen in these extremely preterm infants along with the association between drug exposure and the ductus diameter time course.
Hepatic toxicity of acetaminophen has been reported when plasma concentrations exceeded largely the therapeutic levels. This complication is attributed to the production of highly reactive metabolites by hepatic cytochrome P (CYP)-450, primarily by the CYP2E1 [15]. In our study, no significant variation in ALT levels was pointed out during acetaminophen treatment in dose level 1 nor in dose level 2. Regarding AST values, we observed a significant decrease as a function of time during treatment towards normal values with postnatal age. In this cohort of patients, no hepatic alteration was suspected during or after the 5 days of treatment.
The hemodynamic effect of acetaminophen was previously studied and only a very modest decrease in heart rate and mean arterial blood pressure was reported on prospectively collected observations in 72 neonates with no clinical relevance [16]. This agrees with our findings, as no significant alteration in hemodynamic parameters were observed based on systolic and diastolic blood pressure measured before and 30, 60, 90, 120 min after end of each drug infusion.
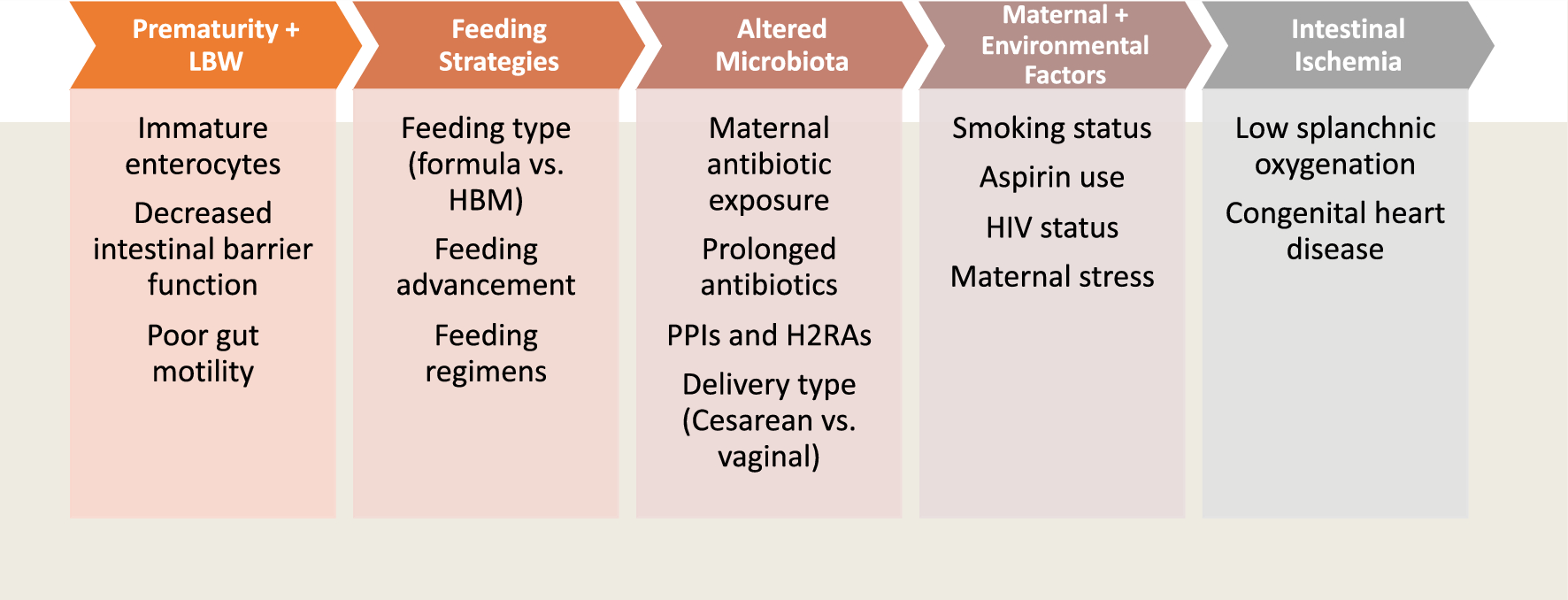
A total of 27 SAE occurred in 13 patients. The most affected organ was the gastrointestinal system, including eight patients with either necrotizing enterocolitis or gastrointestinal perforation. In a recent study, general incidence of spontaneous intestinal perforation was estimated around 8% in infants < 29 weeks gestational age. In our study, we observed specifically gastrointestinal perforation at rate of 13% (95% CI, 3.6–29%). Regarding the association between GI SAEs and treatment failure, no statistical difference was pointed out regarding the gastrointestinal SAE rate among patients in failure or not (33% versus 14%, respectively p = 0.39). However, the low sample size may limit interpretation of these results.
Among the eight patients with either necrotizing enterocolitis or gastrointestinal perforation, three were assessed as possibly related to the study drug by investigators. Interestingly, all eight patients received hydrocortisone that might have increased the risk of spontaneous gastrointestinal perforation [17]. A suspicion of safety concern was raised, and these cases were reviewed with members of the DSMC. However, the DSMC estimated that extremely premature infants are a high-risk population with many expected complications and that the pattern of events we observed was consistent with what might be observed in these infants. Interestingly, most of the patients presenting a gastrointestinal SAE received prophylactic treatment by hydrocortisone, known to have gastrointestinal adverse events. In most of the cases (seven out of eight cases of GI event), acetaminophen administration had been completed or stopped several days before the occurrence of GI events, while hydrocortisone treatment was still ongoing in most of the cases (six cases out of eight cases of GI event). Thus, and given the known pharmacologic properties and half-life of acetaminophen in neonates (around 4 h) [8], chronology seems more compatible with an effect of hydrocortisone. Moreover, the proportion of patients treated by hydrocortisone was unbalanced between dose level 1 and 2 (91% versus 56%), which might explain the lower observed gastrointestinal disorder incidence rate in dose level 2. Besides, preterm infants with slightly higher birth weight and lesser use of mechanical ventilation in dose level 2 might explain also in part the lower SAE rate. Gastrointestinal complications were considered as special-interest events and will be carefully monitored in phase III. In the same way, the safety in the long term is yet to be proven. The more patients exposed to acetaminophen, especially those at lower risk, the higher the chance it will alter the benefit. This will be considered and investigated in phase III. The benefit–risk balance was the basis of this dose escalation phase II study with the aim to avoid unnecessary overexposure to acetaminophen in this vulnerable population.
The survival rate in the study was relatively high given the gestational age included in this study. A total of four deaths (12.9%; 95% CI 3.6–29.8%) were observed, all corresponding to birth < 25 weeks gestation. Interestingly, the mortality rate observed in this study appears substantially lower than those reported in two previous French studies, the PREMILOC interventional study [18] and the EPIPAGE observational study [24].
In conclusion, according to the present phase II study, the minimum effective dose included 25 mg/kg loading dose, followed by 10 mg/kg/6 h for 5 days for extremely preterm infants. Acetaminophen was well tolerated in this study. Phase III, the second part of the TREOCAPA project, is ongoing to evaluate the interest of acetaminophen using a clinically relevant endpoint such as survival without severe morbidity compared with placebo.



留言 (0)