
記住我


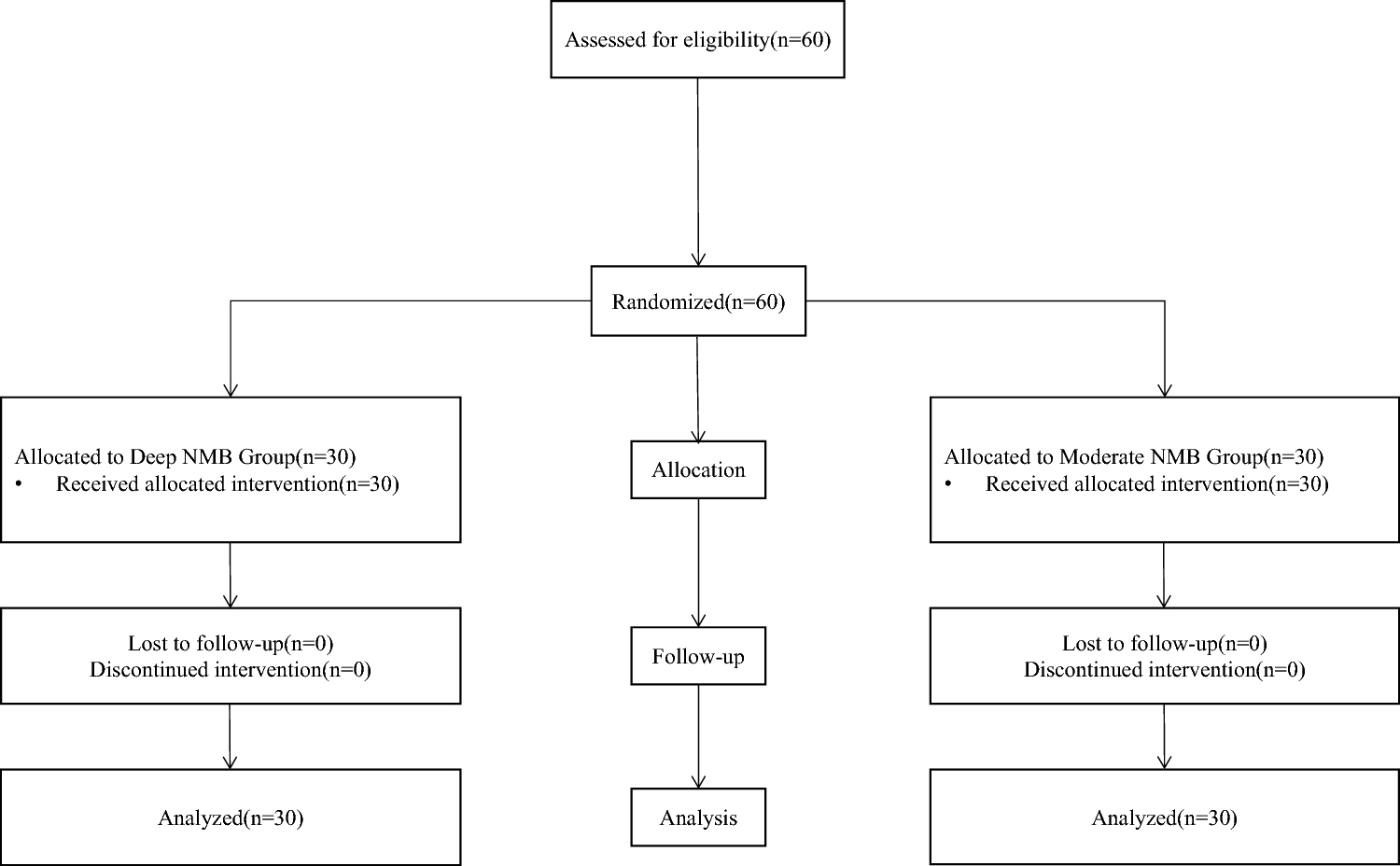
CROCuS (Children’s RSV Outcome Clinical Study; EudraCT Number: 2016-003642-93; ClinicalTrials.gov Identifier: NCT03656510) was a multicenter, double-blind, placebo-controlled, randomized, adaptive phase II study conducted at 176 sites in 22 countries (Fig. 1). The study was conducted from 3 December 2018 (first informed consent signed) to 18 April 2022 (last patient, last visit). The study was terminated prematurely, as the sponsor made a non-safety-related strategic decision to discontinue the development of rilematovir in view of the encountered operational and clinical development challenges.
Fig. 1
Study design. C1 Cohort 1, C2 Cohort 2, RSV respiratory syncytial virus. aStudy sites were located in Argentina, Belgium, Brazil, Bulgaria, France, Germany, Hungary, Italy, Japan, Malaysia, Mexico, Poland, Russia, Taiwan, Thailand, South Africa, South Korea, Spain, Sweden, Turkey, UK, and the USA. bScreening and treatment could have occurred on the same day. cThe original estimated sample size for C2 was N = 150, or 50 patients per treatment group. The sample size in C2 was allowed to be increased to a maximum of 300 (100 per treatment group) based on a pre-planned sample size re-estimation after interim analysis 3. dPrior to Protocol Amendment 4, study treatment was administered once daily. After Protocol Amendment 4, study treatment was administered twice daily, with the total daily dose remaining unmodified. eRilematovir dosing and volume of placebo were based on weight (mg/kg) and age group for both cohorts. fC1 after discharge and C2. gIn case of ongoing adverse event(s)
The study design included pre-planned interim analyses (IAs) and adaptive design elements (Table 1 of the Electronic Supplementary Material [ESM]). An independent data monitoring committee was commissioned to review unblinded safety data on a regular basis, as well as data from the IAs, and to make recommendations to the Sponsor Committee. At any point during the study, the independent data monitoring committee had the authority to recommend modifications to the study conduct and/or to safety assessments, including the recommendation to halt a dose arm because of safety concerns.
2.2 Eligibility CriteriaChildren aged ≥ 28 days and ≤ 3 years with laboratory-confirmed RSV disease who were otherwise healthy or had a risk factor for severe RSV disease were eligible, provided they could be randomized within 5 days after RSV symptom onset. Laboratory-confirmed RSV disease was defined as RSV positive by molecular or antigen-based testing with one or more symptoms of upper respiratory tract infection (nasal congestion, rhinorrhea, pharyngitis, or otitis media), one or more symptoms of lower respiratory tract infection (increased respiratory effort [as evidenced by subcostal, intercostal, or tracheosternal retractions; grunting; head bobbing; nasal flaring; or tachypnea], abnormal breathing sounds [such as wheezing, rales, or rhonchi], cyanosis, apnea, or cough [cough or wheezing should have been accompanied by one or more additional lower respiratory tract infection sign/symptom]), and one or more systemic/general symptom (feeding difficulties, defined as a < 75% intake of normal food amounts; dehydration; fever; or disturbed sleep or disturbed activity level, including irritability, restlessness, agitation, and decreased responsiveness). Examples of risk factors for severe disease and key exclusion criteria are provided in the ESM.
2.3 Study ProceduresChildren presenting to a healthcare facility with symptoms of an acute respiratory illness supporting a diagnosis of RSV infection (e.g., nasal congestion, rhinorrhea, pharyngitis, increased respiratory effort, abnormal breathing sounds [wheezing, rales, or rhonchi], cyanosis, cough, apnea, fever, feeding difficulties, dehydration) were screened. A nasal swab was taken to test for RSV infection if nasal swabs were not taken as part of the standard of care. Enrolled patients who were hospitalized were included in Cohort 1, while those who were treated on an outpatient basis were included in Cohort 2. Within each cohort, patients were centrally randomized (1:1:1) to receive either a low or high dose of rilematovir or placebo, stratified by the time since symptom onset (≤ 3 days, > 3 days to ≤ 5 days) and the presence of risk factors for severe RSV disease. Study treatment was initiated ≤ 4 h post-randomization. Following IA3, a population-enrichment decision was made and enrollment in Cohort 2 was limited to only patients with ≤ 3 days since symptom onset.
Study treatment was administered as a flavored oral suspension (rilematovir active powder reconstituted to 23 mg/mL) for 7 consecutive days, with the total daily dose based on weight (mg/kg) and age group (age group 1: ≥ 28 days and < 3 months; age group 2: ≥ 3 months and < 6 months; age group 3: ≥ 6 months and ≤ 3 years) for each cohort to achieve target exposures established by a phase Ib pharmacokinetic analysis [18]. Analysis of interim data from CROCuS (n = 62; once-daily dosing) yielded exposure metrics (maximum observed concentration at steady state, trough concentration at steady state, and AUC up to 24 h post-dosing at steady state) that confirmed population pharmacokinetic modeling, and simulations predicted exposures indicating that study drug exposure was consistent across the different age groups. Dosing frequency was changed from once to twice daily (Protocol Amendment 4) to mitigate the potential risk of QT interval prolongation, while maintaining the highest potential antiviral effect and minimizing the risk of developing antiviral resistance. While the dosage per administration was reduced by half with the change in dosing frequency, the unmodified total daily dose was expected to result in similar exposures. Patients in the high-dose group received total daily doses of 5.0 mg/kg (0.300–2.2 mL), 6.0 mg/kg (0.375–2.6 mL), or 9.0 mg/kg (0.550–4.0 mL) of study treatment for age groups 1, 2, and 3, respectively; those in the low-dose group received total daily doses of 1.7 mg/kg (0.125–0.725 mL), 2.0 mg/kg (0.125–0.850 mL), or 3.0 mg/kg (0.200–1.3 mL) of study treatment for age groups 1, 2, and 3, respectively (Table 2 of the ESM). Patients in the matching placebo group received high-volume or low-volume placebo in accordance with their weight and age group.
The total study duration was approximately 29 days (screening: day - 1 to day 1; treatment period: day 1 to day 8; follow-up period: day 9 to day 28 [± 3]; Fig. 1). On-site follow-up visits took place on days 14 ± 1 and 21 ± 3; an on-site or telephone follow-up visit took place on day 28 ± 3.
2.4 Study AssessmentsPatient demographics and characteristics (e.g., presence of comorbidities or risk factors for severe RSV, RSV symptom duration, and RSV viral load) were collected at screening. The RSV viral load in nasal secretions was measured at a central laboratory (Viroclinics-DDL, Rotterdam, The Netherlands) using a quantitative, real-time, reverse transcription polymerase chain reaction (qRT-PCR) assay on mid-turbinate swab specimens that were collected at screening, daily during treatment, daily from day 9 up to day 13 if patients were still hospitalized (Cohort 1) or symptomatic (patients in Cohort 1 who had been discharged and Cohort 2), and on days 14 and 21. The severity and duration of 12 RSV signs and symptoms, including six key RSV symptoms (breathing problems, tachypnea, tachycardia, retractions, breathing sounds, and cough), were assessed using the PRESORS observer-reported outcome questionnaire (PRESORS ObsRO; Version 7.1) [20], which was completed by caregivers [21] on an electronic device at screening, twice daily (morning and evening) from day 1 to day 14, and once daily (evening) from day 15 to day 21 (Table 3 of the ESM) [20, 21].
2.5 Study Objectives and EndpointsThe primary objective was to establish antiviral activity by assessing the AUC of RSV RNA viral load, as measured by qRT-PCR in nasal swabs, from immediately prior to the first dose of study treatment through day 5. The primary hypothesis was that rilematovir has antiviral activity against RSV, as assessed by a positive dose–response relationship of rilematovir compared with placebo. Selection of the primary antiviral endpoint was based on the early antiviral effect of rilematovir observed in a phase Ib study [18]. The primary efficacy analysis of the study was based on the results of Cohorts 1 and 2 combined, as antiviral activity was expected to be independent of the clinical setting. Secondary objectives included evaluation of the dose–response relationship for antiviral activity, the impact of rilematovir on the clinical course of RSV infection, the emergence of changes in viral genome potentially associated with antiviral resistance, acceptability and palatability, and safety and tolerability.
Secondary virologic endpoints included changes from baseline in RSV viral load over time and the time to first confirmed undetectable RSV RNA viral load (defined as an RSV RNA viral load value less than the lower limit of quantification [LLOQ], target not detected). For the RSV-A qRT-PCR assay, the limit of detection was 620 (2.8 log10) copies/mL, and the LLOQ was 1000 (3 log10) copies/mL. For the RSV-B qRT-PCR assay, the limit of detection was 80 (1.9 log10) copies/mL, and the LLOQ was 250 (2.4 log10) copies/mL. A confirmed undetectable sample was defined as the first of two or more consecutive undetectable samples post-baseline.
Secondary clinical endpoints for Cohort 1 included the time to hospital discharge and time to the end of oxygen supplementation (Methods in ESM). Meanwhile, RSV signs and symptoms (assessed using the PRESORS ObsRO) and medical resource utilization (i.e., need for hospitalization [Cohort 2] or re-hospitalization [Cohort 1] or outpatient encounters during the study) were assessed for both cohorts. During the study, the definition of time to resolution of PRESORS ObsRO key RSV symptoms was evaluated and refined at interim stages to ensure a more suitable, clinically relevant endpoint for further development in phase III studies. The requirement of being free of oxygen, hydration, and feeding supplementation for at least 24 h was added, resulting in the derivation and analysis of the time (hours) from the first dose of study treatment until the first time at which all key RSV symptoms were scored as not present or mild (i.e., “resolved”) after being free of oxygen, hydration, and feeding supplementation for at least 24 h (Table 3 of the ESM). This requirement was added as such supplementation could mask symptom severity.
Acceptability and palatability of rilematovir were assessed by questionnaires completed by caregivers on day 8. Safety and tolerability were assessed by adverse events (AEs), clinical laboratory assessments, electrocardiograms, vital signs, and physical examinations throughout the study. RSV-related complications were identified from reported AEs and classified according to respiratory complications, infectious complications, cardiovascular complications, and acid-base or electrolyte complications. AEs were coded using the Medical Dictionary for Regulatory Activities Version 23.1 [22]. Clinical laboratory assessments were conducted at screening, day 8, and day 21, and, for patients with an onsite visit, on day 28. Laboratory abnormalities were determined according to the Division of Microbiology and Infectious Diseases pediatric toxicity tables (November 2007). Patients’ safety was monitored throughout the study by an independent data monitoring committee.
The emergence of changes in the RSV F gene sequence was evaluated by next-generation sequencing (Illumina, San Diego, CA, USA) of mid-turbinate swab samples collected at baseline and selected post-baseline timepoints (Viroclinics-DDL). Sequencing analyses of RSV-A and RSV-B strains focused on 24 F protein positions of interest for RSV F inhibitors (positions 127, 137, 138, 140, 141, 143, 144, 323, 338, 339, 392, 394, 396, 397, 398, 399, 400, 401, 474, 486, 487, 488, 489, and 517) [17, 23]. Additional information is provided in the ESM.
2.6 Statistical AnalysisAll randomized patients who received one or more doses of study treatment were included in the safety analysis population. Efficacy analyses were conducted in the intent-to-treat-infected (ITT-i) analysis population, defined as all randomized patients who received one or more doses of study treatment and who had an RSV RNA viral load of ≥ 1 log10 copies/mL above the LLOQ of the RSV qRT-PCR assay at baseline. Patients’ data were analyzed according to the randomized treatment arm.
The primary analysis and analysis of the dose–response relationship were conducted using a hybrid methodology combining aspects of multiple comparison testing with modeling techniques (Multiple Comparison Procedure-Modeling) [24,25,26], as described in the ESM. The time to the first confirmed undetectable RSV RNA viral load, resolution of key PRESORS ObsRO RSV symptoms, hospital discharge, and the end of oxygen supplementation were estimated using the Kaplan–Meier analysis.
2.7 Sample SizeAssuming a reduction in RSV viral load AUC of 20% compared with placebo, considering a coefficient of variation of 35%, and a one-sided alpha of 2.5%, the power to conclude a dose response using the Multiple Comparison Procedure-Modeling procedure under different assumptions for the dose–response relationship (linear, maximal efficacy, and exponential) was > 90% if data of both cohorts were combined (n = 74 per treatment arm). Therefore, the trial was initially planned to enroll 72 participants in Cohort 1 (n = 24 per treatment arm), and 150 participants in Cohort 2 (n = 50 per treatment arm). During the trial, it was decided to increase the sample size in Cohort 1 to 144 (n = 48 per treatment arm) to enable a more precise estimation of the clinical course endpoints in this hospitalized cohort (Protocol Amendment 1).
As no clinical endpoints for a phase III study had been identified at the time of study design and the association between the antiviral effect and clinical course endpoints was not yet established for RSV, a key secondary objective of this phase II study was the evaluation of clinical course endpoints and their dependence on viral load reductions. Results of this phase II study were meant to inform the discussion on and selection of clinical course endpoints and guide the design for subsequent phase III studies. Therefore, during IA3, a sample size re-estimation was performed to allow an extension of Cohort 2 to confirm and increase the precision of the results of selected clinical course endpoints (Nre-estimated = 210; Table 1 of the ESM). Clinical course endpoints considered were time to resolution of key RSV symptoms (PRESORS ObsRO), incidence of RSV-related complications, and change from baseline in key RSV symptoms (PRESORS ObsRO). The number of patients in Cohort 2 required to limit the conditional “consider” probability (i.e., an inconclusive result at the end of the study) to 20% for clinical endpoints was calculated (up to a maximum of n = 100 per treatment group) using a Go/No-Go approach, with a required confidence of 90% (one-sided) to exclude a predefined target value and/or minimum acceptable value.
留言 (0)