
記住我

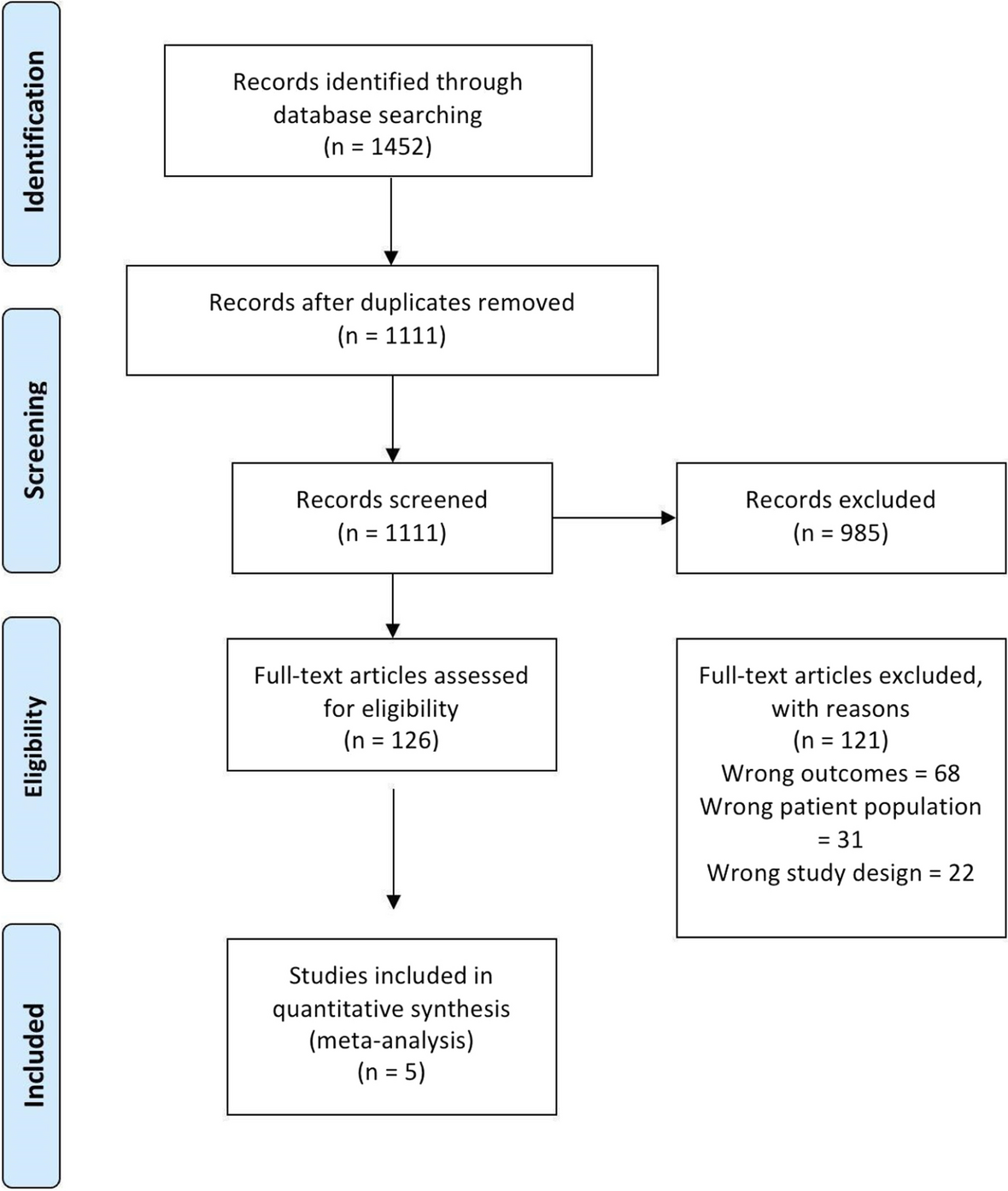


Among 343 initially returned articles, 203 articles were excluded in the first screening step, with 98 duplicates and 42 non-English articles. After the next step, in which titles and abstracts were reviewed, 158 articles were left for the full-text review. Ultimately, there were 126 articles remaining that met the inclusion criteria (Fig. 1, Table 1).
Definition and symptoms of OGOG is the previous name given to direct intraoral current that is a continuous flow of current in the oral cavity through insulators or conductor, such as a wire and a vacuum-like ion beams, from high to low potential. This OG has variable size, but its flow direction is always the same according to its polarity. OG is also known as electro-galvanism due to its unidirectional current of electric charge and is generated in the saliva-filled oral environment in the presence of two or more dissimilar metals. The most common OG is related to dental amalgam restorations, from which are released metallic oxidized ions on the metal surface. The main causes of cast alloy related to OG can be divided into those with dental and oral origins, including anatomic anomalies, materials, rehabilitated preparation, dental plaque, viral or fungal reactions, and those with non-dental reasons, including general disease, medication, and others such as psychological background (Fig. 2). Regarding dental materials, biological incompatibility such as bacterial adhesion, toxicity, sub-toxic effects, and allergy is representative causes of OG.
Fig. 2
Table of the main causes of cast alloy related with oral galvanism could be divided as dental origins including anatomic anomalies, materials, rehabilitated preparation, dental plaque, and viral or fungal reaction or non-dental origins including general disease, medication, and others such as psychological backgrounds. Dental materials with biological incompatibility, such as bacterial adhesions, toxicity, subtoxic effects, and allergy, were the representative cause of oral galvanism
Galvanic current or a galvanic cell in the oral cavity is called a bimetallic cell with electrochemical differences from dissimilar intraoral metal alloys (Table 2). Ti and other metallic elements, such as cobalt (Co), nickel (Ni), gold (Au), palladium (Pd), mercury (Hg), iron (Fe), silver (Ag), and copper (Cu), have their own individual electrical potentials in the diverse intraoral situation. Thus, more than two different metals including titanium and its related implant prosthetic components might generate unexpected electromotive current [5, 8]. Unfortunately, this galvanic current cannot be measured easily due to its diverse electrical energy properties (Table 2), because intraoral Ti-related galvanic cells are often caused by different metal concentrations and bimetallic cells [14]. As with the galvanic concentration cells from dissolved oxygen in the chemically different electrolyte solution, this titanium ion can make an unexpected galvanic current in diverse intraoral saliva environments [15] (Fig. 3).
Table 2 Main electrode in various alloy types and their standard electrode potentialFig. 3
Schematic drawing of galvanic current measurement device having one electrode on the metallic prosthesis and another one for measurement of the potentials and currents
The main symptoms of OG are an unpleasant burning sensation in the related teeth, intraoral metallic taste, disturbed smell, oral mucosal or tongue pain, and even atypical neuralgic pain. These atypical pains or discomfort can be expressed as emesis, vertigo, or continuous headache. Most of these symptoms occur after delicate changes in occlusal relationships of opposing teeth or in contact relationships of adjacent teeth after amalgam filling restorations or any metallic crown setting including implant crowns [16, 17]. An intraoral metallic taste is a persistent feeling with a vague sensation of smelling or tasting tinfoil taste after any metallic prosthesis delivery. A typical radiating unpleasant feeling is described, ranging from mild discomfort to a dull or worsening pain and ultimately as low-grade continuous pain.
Pain originating from OG has been noted both from an electronic circuit in the metallic restorations and from silver foil or spoon contact on biting [12, 15, 18]. More recently, these pains have originated from ion flow known as the battery effect in restorative dental works [12, 19, 20]. Severe pain might be referred to or projected to other body regions and experienced as headache, facial pain, or low back pain and also may be regarded as psychosomatic pain or discomfort. This psychosomatic pain of OG is a lower sensibility threshold and had a severe mental disease on a hidden psychosis of patient. Some of these patients could be found later to have a psychosomatic cause of pain [12, 21,22,23,24], and this pain might increase according to increased mental disturbances but also disappear easily after a recovery from psychosis.
Diagnosis with testing methods including immune markers Clinical diagnosis and management of OGMost patients experiencing OG visit the dentist initially and then a family doctor, internal medicine specialist, and otorhinolaryngologist complaining of intraoral pain or discomforts with unknown origins. Due to atypical signs or symptoms of OG, the initial diagnosis is somewhat difficult, but the first step is to collect anamnestic information including age, gender, main symptoms, onset and duration, general health, medical and dental history, and past or recent medications.
An intraoral examination is necessary for the exact identification of number and surface features of filling materials or metal restorations. This could be accompanied by routine radiograms including panoramic view and hematologic or urine analysis, and fungal contamination test may be carried out in partially edentulous or senior patients with saliva flow rates. However, the most important oral examination is the identification of metal restoration in the vicinity of surrounding mucosal inflammations, lichenoid changes of buccal mucosa, and metal-stained mucosa. The results of the visual exam are recorded as none, rare, slight, moderate, or severe, of which scales could be helpful for recording each patient’s own pain or discomfort level.
The patient’s main symptom is pain, which usually occurs after occlusal-related prosthesis fabrication or a recent filling treatment. If there are different materials or properties of metals related to the occlusal surface, the metal may be separated by rubber for the tentative clinical diagnose of OG, and any suspicious pain of galvanic currents might be relieved by the simple separations of the metallic prostheses [14, 17, 25]. In addition, even after a new prosthetic treatment is applied to an adjacent tooth, an initial clinical diagnosis is possible by separating the tooth in the same way. A barrier can be created with silver nitrate and composite resin, or other nonmetallic material can be used [14, 25]. If the patient’s pain symptoms disappear with simple separation, primary diagnosis and treatment may be possible by replacement with the same material-based prosthesis or filling materials or nonmetallic materials. A clinical OG diagnosis and replacement of related intraoral prosthetic materials to avoid contact between dissimilar metals can relieve pain and discomfort in sensitive patients. After removal of this galvanic cell, the patients can be educated regarding these situations and avoiding way for his/her further dental treatments.
For the psychiatric evaluation, it can be recommended to check several points such as lack of energy to cope with daily work or household duties, impaired quality of life, tiredness, anxiety, depression, inability to relax, sleeping disorder, and easy annoyances [26]. A full battery of psychological tests, such as BDI (Beck Depression Inventory), MMPI (Minnesota Multiphasic Personality Inventory), STAI (State-Trait Anxiety Inventory), and WAIS (Wechsler Adult Intelligence Scale), might be administered by a psychiatrist. The psychiatric interview is semi-structured, and the DSM-III (Diagnostic and Statistical Manual of Mental Disorders) or CMI (Cornell Medical Index) health questionnaire [27] can be used as basic criteria for a psychiatric diagnosis [12, 14, 28].
Laboratory diagnosis and intraoral testing of OGAll metal elements have their own electrode potential known as standard electrode (Table 2), and various dental metal alloys may influence intraoral galvanic effects due to electron potential differences. The protective passivation layers between the metal alloy and salivary electrolyte produce OG, and continuous abrasion and corrosion in this damaged interface worsen galvanic effects [29,30,31]. Most dental restorative alloys have the potential to cause intraoral hypersensitivity of the skin or intraoral mucosa. Common metal elements used in fabrication of dental crowns and bridges are Ni, chromium (Cr), Co, Pd, gold (Au), Ti, and Hg. Most noble metals such as Au or Pd are resistant to light or dry corrosion in hypersensitive skin when used in jewelry. However, even these noble metals might be corroded due to exposure to the moist environment of the oral cavity [22, 32,33,34,35]. However, it has been unknown which mechanisms are averse to metal alloys, nor pathognomic to innate immunity of oral cavity.
Heavy metals can be found in urine, feces, and blood tests. The most common metals tested are lead (Pb), Hg, arsenic (As), and cadmium (Cd), while less common metals include Cu, zinc (Zn), aluminum (Al), and thallium. Sometimes, hair analysis might be needed; for example, an Hg analysis of head hair was performed for investigation of metal exposure using cold-vapor atomic absorption spectrometry [36, 37]. Hair mineral analysis is used as a toxicological screening for metals including uranium (U), Pb, Hg, Cd, As, Al, and Ni.
For direct measurement of the sensibility threshold, electric stimulation using rising values of current can be performed by placing the negative electrode of an electronic pulp tester on the occlusal surface of each premolar or adjacent teeth. The indifferent electrode is placed on the occlusal surface of the premolar in the next oral quadrant, and the pulp tester is connected to voltage- and current-measuring instruments. The electrical current emitted by the tester is pulsated, the minimum current intensity evoking a sensation is recorded [38, 39], and the sensibility threshold is measured on the oral mucosa. To measure galvanic current between different dental alloys, the tongue, mucosa, and lips, several measurement devices were used, including an Odontologic 2000 device® (Embitron Co., Prague, Czech Republic) and an FfB Oralenergiemessgerat EM202® (FfB Co., Nürnberg, Germany) [40,41,42]. Every measurement device has a similar mechanism in which one electrode is placed on the metallic prosthesis, and the other is used for the measurements of the potentials and currents (Fig. 3).
For a better understanding of OG measurements, we evaluated international patents for the correlational research of OG with dental implant surface and prostheses. On the patent searching site https://patents.google.com/?q=Oral+galvanism&oq=Oral+galvanism, 211 search results were returned for “OG”, and 157 results were returned “dental implant galvanism” (https://patents.google.com/patent/EP1278479A1/en?oq=EP1278479A1, https://patents.google.com/patent/US8784104B2/en?oq=US8784104B2, https://patents.google.com/patent/RU2218078C1/en?oq=RU2218078C1, https://patents.google.com/patent/SE8604941D0/en?oq=SE8604941D0, https://patents.google.com/patent/RU2326620C1/en?oq=RU2326620C1, https://patents.google.com/patent/RU2462184C1/en?oq=RU2462184C1, https://patents.google.com/patent/RU2212185C1/en?oq=RU2212185C1) . Additional PCT searches on https://patentscope.wipo.int/search/en/search.jsf also returned 63 results under the keywords of OG and galvanic (https://patents.google.com/patent/US5725377A/en?oq=US5725377A, https://patents.google.com/patent/RO123606B1/en?oq=RO123606B1, https://patents.google.com/patent/KR100898726B1/en?oq=KR100898726B1, https://patents.google.com/patent/RU2018285C1/en?oq=RU2018285C1, https://patents.google.com/patent/CN103027757A/en?oq=CN103027757A, https://patentscope.wipo.int/search/en/detail.jsf?docId=SE227190350&_cid=P11-K7CNAM-76771-1, https://patentscope.wipo.int/search/en/detail.jsf?docId=RU29358799&_cid=P11-K7CNC5-77054-1, https://patentscope.wipo.int/search/en/detail.jsf?docId=RO233910277&_cid=P11-K7CNCZ-77146-1, https://patentscope.wipo.int/search/en/detail.jsf?docId=WO1997036551&_cid=P11-K7CNDF-77195-1) (Table 3). Different methods of galvanic current measurement in the oral cavity have been developed to observe the pathological effect of galvanic currents and voltage in the oral mucosa; nevertheless, correlative significance is still unknown [40, 43].
Table 3 International patent and PCT searching for oral galvanism Immune markers of OGOG could affect the immune defense reactions of the oral cavity and cause a range of different types of discomforts in the oral cavity. Most immunologic markers in the oral cavity are different levels in the human saliva with decreased levels of IgA1, IgA2, secretory IgA (sIgA), and lysozyme and an increased level of IgA against heat-shock protein 60 (anti-hsp60 IgA) [44,45,46]. Podzimek et al. [44] analyzed 397 oral discomfort patients and 30 patients with removal of electro-active dental materials and demonstrated the importance of measuring GC in patients having oral discomfort symptoms, such as inflammatory lichen planus on the tongue and buccal mucosa, gingival metal pigmentations, prosthetic corrosion, and metallic taste. Levels of IgA1, IgA2, sIgA, and lysozyme were increased, with decreased levels of anti-hsp60 IgA after removal of prosthetics, and clinical symptoms were also decreased in 70% of patients. This author described that oral prosthesis with more than 5 μA GC had an electro-active trend and recommended that at currents greater than 10 μA GC, the oral prosthesis be removed from the patient [44].
In another whole saliva study, proteins, Na, Cl, and P were significantly higher, and Ca, Mg, and IgA concentrations were lower, in OG patients; these proteins, lysozyme, and Ca concentrations were changed in the parotid saliva as well. However, pH did not change according to galvanic current differences or galvanic symptoms [41]. A decrease of saliva pH may affect local changes in biofilm contacting the metallic prostheses rather than galvanic current itself, followed by passivation or activation of the intraoral electric currents in the surfaces of metallic restorations.
Compared with B-lymphocyte responses, proliferation of T lymphocytes was significantly decreased by galvanic current and voltage changes. This situation could be prolonged by metal ion release in the oral cavity, which was also compatible with lymphocyte potential changes such as K+ and Ca2+ conduction block [47]. Functional K+ channels are necessary for T-lymphocyte proliferation [48, 49], and values of galvanic currents and voltage affect potentials of K+ channels, leading to T-lymphocyte malfunction [44]. The pathologic intensity values of galvanic current and voltage ranged from 3 to 10 μA and from 80 to 200 mV [50], depending on the surface molecules including CD 3, 19, 11a/18, 3/69, 3/95, 19/69, and 19/95 from lymphocytes. Additionally, pathological threshold values of 5 μA for galvanic currents and 100 mV for galvanic voltage were reported [44].
Galvanic corrosionGenerally, metal corrosion can be defined as a phenomenon in which a metal material undergoes a chemical or electrochemical reaction with the surrounding environment, deteriorating the material properties or shortening its effective useful life. Metal corrosion can be classified as high- or low-temperature corrosion [47, 48]. Atmospheric, seawater, soil, and microbial corrosion are divided according to the environmental change. In addition, shape differences such as uniform, intergranular, pitting, crevice, and galvanic corrosion are different corrosion types, with selective leaching and hydrogen damage types as well (Fig. 4).
Fig. 4
Schematic drawing of different metallic corrosion types by shape, including uniform, intergranular, pitting, galvanic, and crevice corrosion
Incidence of metallic corrosion increases with increasing temperature and Cl and decreasing Cr and Mo contents of the metal [10, 49]. Intergranular corrosion, or intergranular attack, may occur where the boundaries of crystallites of the material are more susceptible to corrosion than their insides. Pitting corrosion is similar to crevice corrosion (CC), which is brought about by local damage to the passive film, with chlorides playing a significant role [48,49,50]. The hydrolysis of the released corrosion products decreases the pH value of the electrolyte in the pit or crevice, accelerating corrosion [50]. CC, a localized attack on a metal surface, may occur at the gap or crevice between two joining surfaces. These gaps or crevices can be formed between two metals or between a metal and a nonmetallic material. CC refers to corrosion that occurs in confined spaces that are difficult to clean or difficult to access, commonly referred to as crevices. Among various intraoral crevices, a gap between a prosthesis and the remaining tooth, or a crevice between the boundary of a prosthesis and other fillings, can be considered. In these intraoral crevices, oxygen is insufficient, or the movement of oxygen is restricted, so that hydrolysis corrosion products are generated in the crevices. This results in local decay of the passive state due to a decrease in pH, which is particularly common in stainless steels when chlorides are involved. Decayed pits, scratches on alloys due to abrasion or insufficient finishing in dental laboratories, and interdental spaces or tight spaces between different parts of a restorative structure can be considered intraoral crevices, and these CCs include special microenvironments in the oral cavity. Diverse dental restorations, including dental implants, are often fabricated to extend below the gingival margin into the gingival fissure, and physiological fissures or crevices also occur.
Intraoral electrochemical corrosion is also known broadly as OG. However, the exact terminology with GC is defined as an ionic release from intraoral metallic restorations, which can cause local or systemic pathological problems associated with OG [14, 15, 51]. GC, or bimetallic corrosion, is the contact corrosion between two dissimilar metals or alloys under the circumstances of electrolyte. This electrolyte makes a driving force named electrochemical potential between two dissimilar alloys, such as body fluids or saliva. Several metal ions released from dental alloys, albeit in small amounts, have short- or long-term effects in the oral cavity through electrochemical corrosion and wear [40, 41, 52]. In addition, the concentration of metal ions in saliva rapidly increases [40, 41].
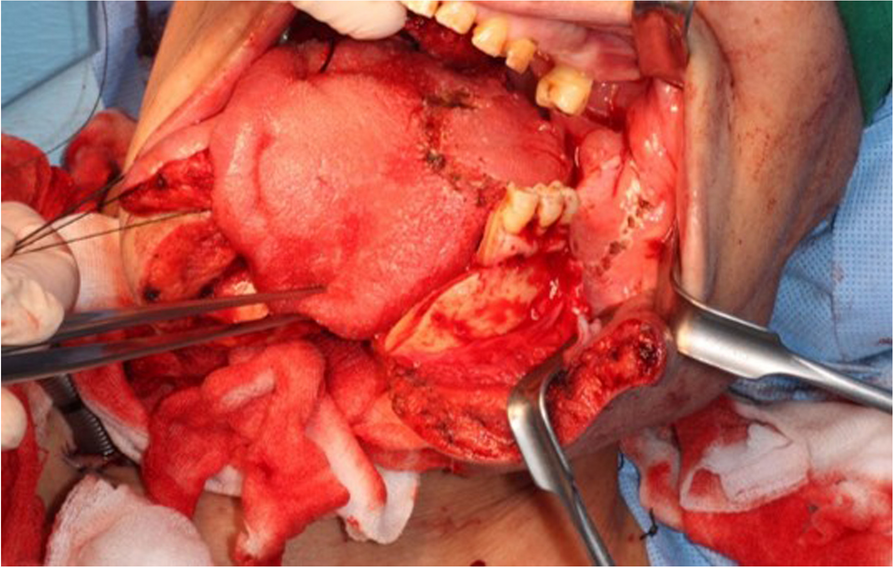
Clinically, GC occurs in a variety of intraoral situations, such as when dental alloys are in direct contact with each other, amalgam fillings are placed right next to a crown, or when opposing metal restorations that are occluding cause mutual interference during jaw functions such as mastication and swallowing. Intraoral GC also occurs as an inevitable chemical reaction between the oral environment and dental implants, which have an essential titanium fixture, titanium abutment and its accompanied implant crown, or other prosthesis. At least two or three different interfacial surfaces between them could release diverse metal ions to activate metal surfaces of each component, resulting in galvanic cell damage near the implant abutment-fixture junctional area (Figs. 5 and 6). This inevitable chemical reaction of dental implant connections is known as intraoral implant corrosion or implant galvanic cell damage.
Fig. 5
Galvanic cell formation near the junction between the implant abutment and fixture showing an inevitable chemical reaction between the titanium fixture, titanium abutment, and its accompanied implant crown or other prosthesis, known as implant corrosion or implant galvanic cell damage
Fig. 6
Schematic representation of Ti debris and reactive ions related to galvanic corrosion in the implant-attached gingival connection. Titanium debris in the implant connection part corroded by reactive ions and phagocytosis by macrophages in the junctional epithelium
Dental alloys are classified into high-grade noble, precious or noble, non-precious, and Ti alloys. High-grade noble metals or Au-based alloys include Au, platinum (Pt), and Pd. Noble metals that are reasonably priced and biocompatible include Pd-based alloys and Au, Ag, Cu, and gallium (Ga). Representative examples of non-precious metals are stainless steel and nickel-titanium (Ni–Ti) alloys mainly used in orthodontic appliances and nickel-chrome (Ni–Cr) and chrome-cobalt (Cr-Co) alloys mainly used in dentures and fixed prostheses. On the other hand, Ti and Ti alloys known for their biocompatibility have been used mainly for dental implant fixtures and superstructures and are widely believed to be biocompatible.
Currently, all dental implant fixtures are made of Ti with a purity of 99wt% or more, and more precisely, they are mad
留言 (0)