There have not been many comparative studies on which of the two surgical approach methods, the swing approach, which accesses through lip splitting and mandibulotomy, and the visor approach, which accesses by making an incision in the neck skin without lip splitting, is more suitable for cancer ablation. However, when actually performing surgeries for oral cancer ablation, whether to use the swing method, which involves dividing the mandible for access, or the visor method, there is a need for the surgeon to make a careful decision based on solid evidence. Surgeons should refer to existing literature for the theoretical background of the decision on the surgical approach, and additionally, a new clinical study should be continuously conducted to provide clearer criteria for determining the surgical approach method. In this study, to compare the surgical outcomes of the two approaches, retrospective analysis of oral cancer surgery in the mandible, tongue, and oral floor areas was divided into four major fields: clinicopathological factors, postoperative prognosis factors, postoperative complication factors, and treatment-related factors.
In the clinicopathological factors section, detailed items related to clinical and pathological evaluations, such as sex and age, drinking and smoking status, primary site, tumor size, and clinical/pathological/histological stages, were assessed. The average age of the patient group that underwent the visor approach was 61.7 years, which was higher than the average of 54.6 years for the swing approach group, but this was not statistically significant. Among the 16 cases of the swing approach, 13 cases had larger tumors, around T3–T4, while in the visor approach group, 7 out of 13 cases were T2 or lower. Although this was not statistically significant, with a P-value of 0.0641, which is close to 0.05. It is considered necessary to conduct studies with a larger number of clinical cases to derive statistically significant results.
The histopathologic grade was the only item in the clinicopathological factors that showed a statistically significant difference between the two approaches. However, since this result can only be known after the surgery, it would be impractical to use it as a criterion for deciding the approach before surgery. In a study by Benjamin et al. [5], it was stated that there was no significant difference between the two approaches in terms of pathological margins and local recurrence rates.
In one another study, it was suggested that the swing approach, which involves directly opening and accessing the mandible, might be superior in terms of the surgical field of view [4]. Additionally, Nam W [1] and Tae K [4] stated that while the visor approach is suitable for accessing the anterior and central parts of the mandible and oral cavity, it is not ideal for accessing the posterior oral cavity and the area around the molars. Therefore, it may be necessary to consider whether different approaches should be applied depending on the primary site. In this study, among the 16 cases using the swing approach, 9 were in the mandible, and 7 were in the oral floor and tongue. For the 13 cases using the visor approach, 8 were in the mandible, and 5 were in the oral floor and tongue. Overall, the ratios were similar, indicating that the location of the primary site itself did not significantly influence the surgeon’s choice of approach. Since no significant differences were observed in postoperative prognosis between the two methods, it was thought that rather than deciding the approach solely based on the primary site, it would be more appropriate to make a decision considering the overall location and size of the lesion, and other factors for each case.
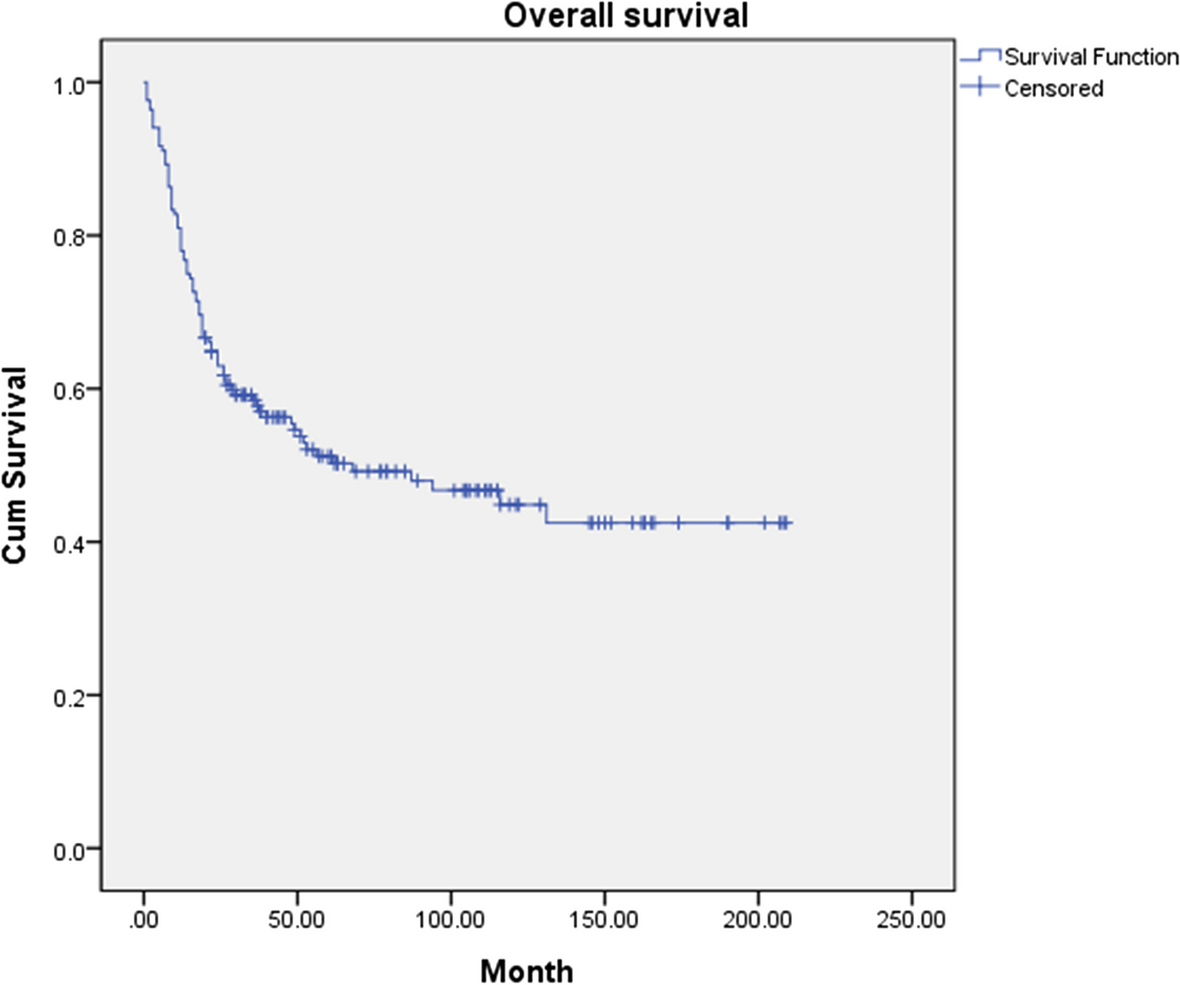
For the postoperative prognosis factors, evaluations were made on locoregional recurrence, cervical node/distant metastasis, survival status over 3 and 5 years post-surgery, and the necessity of postoperative adjuvant therapies such as radiation and chemotherapy. It was observed that the survival rate over 3 and 5 years was higher for the swing approach, but there was also a higher incidence of locoregional recurrence. In the visor group, the proportion of patients who received postoperative adjuvant therapies such as radiation and chemotherapy was much higher, though not statistically significant. But the use of the visor approach alone was not the simple reason for the higher incidence of postoperative adjuvant therapy in these clinical research cases. Instead, it was a comprehensive judgment based on the location and size of the lesion at the time of surgery as well as the postoperative pathological report of the resected specimen.
In the most recent study comparing the two approaches by Vyshnavi [6], it was noted that the surgery duration was longer in the visor group, but the adequacy of exposure, safety margins, surgical outcomes related to healing, and complications were similar in both groups. Additionally, in 2018, Leslie E. Cohen et al. [7] mentioned that there were no significant differences observed in surgical site complications or surgery duration between the two approaches, and both methods can be seen as effective for tumor removal.
In the postoperative complication factors category, evaluations were made on dissatisfaction related to aesthetics, speech, mastication (chewing), and swallowing. Additionally, the occurrence of wound infection was also assessed. In 2023, Hardingham et al. [8] mentioned that difficulty in swallowing is a common outcome after surgical resection of oral or oropharyngeal squamous cell carcinoma. Especially during the visor approach, while there are aesthetic advantages, there is a potential to induce sensory abnormalities in the mental region [9]. In this study, during the postoperative complication assessment, the focus was on aesthetic aspects, and an evaluation of sensory abnormalities was not conducted. During the postoperative assessment of patients, the sensory abnormality status was not recorded in medical records for all patients; hence, this item could not be included in this study. Li et al. [10] proposed a modified visor approach to address these sensory abnormalities by preserving the mental nerve, and as a result, they stated that lip splitting and mandibulotomy were unnecessary. In Li’s study, complications related to swallowing, mastication, and speech also showed similar results between the two approaches [10].
There have been numerous reports of complications related to the mandibulotomy performed during the swing approach. In a study by Byun et al. [11] on complications and contributing factors of mandibulotomy in 2000, postoperative nonunion at the mandibulotomy site was reported. This was attributed to the instability caused by the movement between bone fragments when intraosseous wiring was used. However, it was mentioned that initial nonunion did not occur when miniplates or plates were used for fracture fixation. Most of the other complications were related to postoperative radiation therapy at the mandibulotomy site. McCann et al. [12] reported nonunion and radiation-induced osteonecrosis in patients who received preoperative radiation therapy. Altman and Bailey [13] reported nonunion in the mandible of patients who underwent radiation therapy and recommended avoiding mandibulotomy in patients who received radiation therapy to the mandible. However, Shah et al. [14] stated that pre/postoperative radiation therapy does not affect bone healing. Davidson et al. [15, 16] also mentioned that preoperative radiation therapy does not influence the occurrence of nonunion or malunion related to mandibulotomy, and mandibulotomy can be used during the swing approach without an increased incidence of radiation-induced osteonecrosis, regardless of radiation therapy.
In Vyshnavi’s study [6], the most common complication in both groups was found to be the orocutaneous fistula, indicating wound infection. In a study by Cliento BW et al. [5], it was mentioned that most of the patients who developed fistulas had undergone postoperative radiation therapy. In this study, wound infection occurred in 4 cases with the swing approach, of which 2 had undergone postoperative adjuvant therapy, and in the 1 case with the visor approach, postoperative adjuvant therapy was also used. Although statistical analysis is difficult due to the small sample size, it can be inferred that there may be some infections correlation with postoperative radiation therapy depending on the surgical approach.
There was no clear evidence regarding the induction of postoperative complications by anticancer chemotherapy. Byun et al. [11] reported that complications occurred in 16% of patients who did not receive chemotherapy after oral cancer surgery and 60% of those who did. However, since there were no patients who underwent only chemotherapy, it was reported that an accurate assessment was difficult. In this study, all patients who received chemotherapy also underwent radiation therapy, making it difficult to determine the sole side effect of chemotherapy, suggesting the need for further research.
In this study, the swing approach showed slightly more aesthetic and functional dissatisfaction, and the occurrence of wound infections was also higher. However, this was not statistically significant. In a study comparing the two approaches in functional and aesthetic areas by Leslie E. Cohen et al. in 2018 [7], it was found that the visor flap method showed improvements in both functional and aesthetic aspects. It was also noted that patients who underwent the swing approach had worse outcomes in terms of eating and language functions compared to those who underwent the visor approach. This is presumed to be due to lip splitting, suggesting that the visor approach might offer slight advantages in mastication and speech. Overall, in terms of postoperative functional aspects such as mastication, swallowing, and speech, it is believed that the visor approach can achieve at least similar or slightly better results than the swing approach.
In the treatment-related factors section, analyses were conducted on the duration of hospitalization, the necessity of blood transfusion, the number of days of bed rest, the duration of nasogastric tube maintenance, and the necessity and duration of tracheostomy. In terms of the average hospitalization period, the visor approach required a shorter stay of 43.3 days compared to the 51.0 days for the swing approach, which showed a statistically significant difference. Additionally, while not statistically significant, the duration of nasogastric feeding and tracheostomy maintenance appeared to be longer in the swing approach. This is believed to be a result of a more invasive approach applied to the upper digestive organs and trachea responsible for swallowing when performing lip splitting during surgery. In a study by Devine JC et al. in 2001 [17], it was mentioned that during the swing approach, the genial muscle attached to the center of the mandible needs to be detached, which could delay the postoperative recovery of mastication and swallowing abilities, and this was considered the main reason.
The duration of nasogastric tube maintenance and the number of days of bed rest were clinical factors specifically analyzed in this study to compare the differences between the two surgical approaches, and it was difficult to find similar related studies. However, in terms of the duration of hospitalization, similar results to this study could be found. In Li’s study [10], it was mentioned that without performing lip splitting and mandibulotomy, both aesthetic results and the duration of hospitalization could be reduced in visor approach.
In this study, despite conducting comparative analysis across many evaluation items, it was disappointing that there were few items showing statistically significant differences in results. Despite objective reference points that could be considered indications for choosing a surgical approach were not clearly identified, this research is deemed valuable as it provided various clinical and pathological factors for comparison and analysis, so that surgeons can predict and refer to patient prognosis patterns after applying the two surgical methods. It is expected that future continuous clinical research, collecting and analyzing more than 30 cases per surgical approach, will yield statistically significant results, and this would provide more reliable and meaningful criteria for applying surgical methods. Further analysis through a secondary clinical study is intended.





留言 (0)