
記住我





Bone substitutes are graft materials utilized in ARP to facilitate optimal bone regeneration post-tooth extraction. There are three distinct categories allografts, xenografts, and synthetic bone substitutes (Fig. 1). Allografts, derived from human donors and usually procured from cadavers, are processed to ensure safety and efficacy before use [12]. They include types like demineralized bone matrix (DBM) and freeze-dried bone allograft (FDBA), acting as osteoconductive scaffolds to promote bone growth [13]. On the other hand, xenografts are obtained from different species, commonly bovine or porcine, serving as biocompatible scaffolds for bone regeneration, with bovine bone mineral being a prevalent type [14]. They exhibit osteoconductive properties, aiding in the growth and development of the patient's bone cells.
Fig. 1
Graft materials. a Allografts, (b) xenografts from bovine bone
Studies by Wardani et al. [15] and Saliba et al. [16] explored the application of allografts and xenografts respectively in ARP. While Wardani et al. [15] noted favorable outcomes with allografts, Saliba et al. [16] found significant wound healing potential and reasonable bone regeneration with xenografts, albeit with heightened pain perception. The juxtaposition of allografts and xenografts highlights their diverging characteristics. Human-derived allografts may offer better biological integration, whereas bovine-derived xenografts with their longer resorption rates provide a sustained scaffold, albeit potentially delaying complete bone regeneration [12, 14]. While allografts carry a risk of disease transmission and immunogenic reactions, albeit minimal due to stringent processing standards [12], xenografts pose lesser risk owing to the interspecies barrier, albeit with concerns over prion diseases [7]. Both graft types have shown promising clinical outcomes in bone volume preservation and regeneration [15, 16]. However, the heightened pain perception associated with xenografts as noted in the Saliba et al. study [16] necessitates further investigation. Economic factors, availability, regional regulations, and patient preferences may also influence the choice between allografts and xenografts [7].
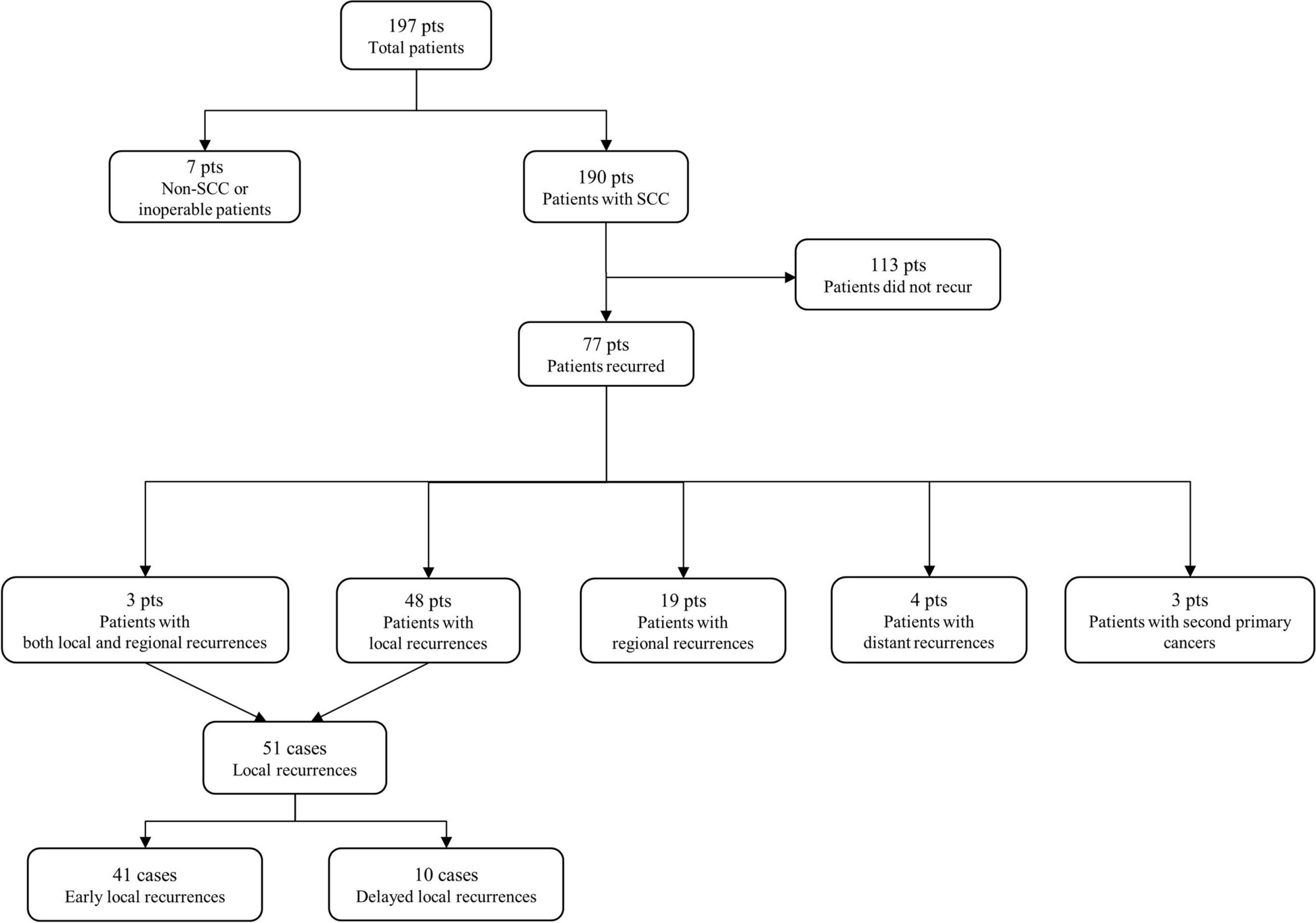
B. Platelet concentratesPlatelet-rich fibrin (PRF), recognized as a second-generation platelet concentrate hailing from autologous blood, demonstrates significant promise in oral and maxillofacial surgical domains due to its proficient wound healing, angiogenesis, and bone regeneration attributes (Fig. 2). Distinct from its predecessor, platelet-rich plasma (PRP), the absence of anticoagulants in PRF facilitates a slow, natural polymerization sequence during centrifugation (Fig. 2). This process culminates in the creation of a dense fibrin clot enriched with fibrin fibers, platelets, leukocytes, and a plethora of growth factors.
Fig. 2
Preparation of platelet-rich plasma (PRP) and platelet-rich fibrin (PRF). PRP is produced through a two-step differential centrifugation process. First, red blood cells (RBCs) are separated during an initial centrifugation phase. Subsequent centrifugation concentrates the platelets, which are then suspended in a minimal plasma volume. This process leverages varying specific gravities to sediment cellular components based on acceleration force adjustments. On the other hand, PRF represents a second-generation autologous platelet concentrate derived from whole venous blood. After a brief centrifugation (~ 10 min) of blood in vacutainer tubes without anti-coagulants, a fibrin gel rich in growth factors, platelets, leukocytes (comprising nearly half of the initial blood sample), and lymphocytes is harvested. This gel is characterized by its slow and strong polymerization
In a recent exploration, Lahham et al. [17] investigated the repercussions of recurrent applications of concentrated PRF (C-PRF) within extraction sockets. The study unveiled notable reductions in hard tissue loss within the test group over a span of 3 months, thereby hinting at C-PRF’s potential in alleviating ridge alterations post-extraction and fostering bone regeneration endeavors [17]. The enriched content of growth factors and bioactive components within PRF notably amplifies socket healing and tissue regeneration. This presents a viable alternative to conventional grafting materials, which necessitate a significantly prolonged integration period before proceeding with implant placements [18].
Upon examining the efficacies of diverse plasma concentrates (PCs) in ARP scenarios, it was ascertained that PCs significantly contribute to new bone formation during ARP in contrast to spontaneous healing [19]. Noteworthy is that among the analyzed PCs, no substantial differences were discerned between leukocyte- and platelet-rich fibrin (L-PRF) and pure platelet-rich plasma (P-PRP), underscoring the potential applicability of either concentrate in ARP instances [19]. Furthermore, Madi et al. [20] substantiated the efficacy of PRF in socket preservation through a methodical review that evaluated the impact of various grafting materials on newly formed bone, both histologically and radiographically. Among the scrutinized materials, PRF emerged prominently for its capability to promote satisfactory new bone formation whilst preserving ridge contour [20]. In another review, Santos Pereira et al. [21] dissected the advantages of advanced platelet-rich fibrin (A-PRF) in tissue regeneration amid reconstructive and jaw graft surgery. The insights from the study positioned A-PRF as a beneficial adjunct in sustaining ridge profile, bolstering bone density, and expediting tissue repair post-extraction [21]. Additionally, the review illuminated the potential of A-PRF in alleviating post-operative pain and swelling, alongside contributing to swifter epithelial healing [21].
The wealth of studies consistently accentuates the auspicious nature of PRF, along with its advanced variant, in enhancing the healing ambiance within oral surgical sites, predominantly post-tooth extractions. Collectively, these findings articulate a persuasive argument for integrating platelet concentrates in clinical regimens to augment bone regeneration and overall tissue healing, thereby smoothening the trajectory for successful dental implant installations.
C. Collagen membranesCollagen membranes are extensively employed with bone substitutes in ARP procedures to reduce bone resorption and promote bone regeneration post-tooth extraction (Fig. 3). Collagen membranes, either derived from animal connective tissues or synthesized, serve as barriers that prevent soft tissue invasion into the bone defect, thereby enabling bone regeneration (Fig. 3A). These membranes are bioresorbable, eliminating the need for secondary surgery for removal, and create a conducive environment for bone healing. Several studies have evaluated the efficacy of bone substitutes and collagen membranes in ARP. For instance, a study highlighted that the deproteinized bovine bone graft and absorbable collagen membrane were beneficial in preserving the alveolar ridge bone, showing no adverse effect on the osseointegration of delayed implants [22]. Another trial aimed to reduce the dimensional changes in the alveolar bone post-tooth extraction by using an equine collagen membrane and a collagen cone, suggesting the potential of collagen materials in ARP [23].
Fig. 3
Bone substitutes, such as synthetic grafts and autogenous bone grafts, serve as scaffolds that support the growth of new bone tissue. a Synthetic grafts, including hydroxyapatite, tricalcium phosphate, and bioceramics, offer a biocompatible alternative to natural bone grafts. b Collagen membranes, derived from various animal sources or obtained through recombinant technology, have gained popularity due to their excellent biocompatibility, biodegradability, and versatile mechanical properties
Different biomaterials have been explored in various studies, including porcine bone substitutes, allografts, alloplasts like biphasic calcium phosphate and β-tricalcium phosphate (Fig. 3B), along with collagen and high-density polytetrafluoroethylene membranes [24]. A systematic review compared the dimensional changes and histological features between anorganic bone and collagen-preserving bone in ridge preservation procedures, promoting awareness of different bone xenograft efficacies in stimulating the healing of post-extraction sockets [2]. Furthermore, a study demonstrated that the use of a bone substitute covered with a collagen membrane resulted in fewer changes in vertical and horizontal alveolar ridge dimensions compared to the collagen membrane alone [25].
A tomographic evaluation by Binkhorst et al. [26] revealed significant preservation of bone volume post-extraction and enhanced bone density when using bone substitutes and collagen membranes, indicative of improved bone quality. This conducive healing period further enabled subsequent restorative procedures like implant placement. While these findings are promising, extended and long-term studies are necessary to ascertain the optimal types and combinations of bone substitutes and collagen membranes for varying clinical scenarios. The utilization of bovine porous bone mineral in conjunction with collagen membrane showed slightly more benefit in preserving alveolar ridge dimensions post-tooth extraction, compared to using bovine porous bone mineral with the autologous fibrinogen/fibronectin system [27]. The diverse findings across different studies underscore the necessity for further research to establish the optimal materials and techniques for ARP, tailored to individual clinical scenarios.
D. Bioactive materialsBioactive materials, encompassing hydroxyapatite (HA), collagen, and three-dimensional (3D) bone repair materials, are at the forefront of advancements in ARP post-tooth extraction. Leveraging modern 3D printing technologies, these materials are engineered to mimic the natural bone structure and composition, thus promoting enhanced integration and regeneration.
A notable exploration in this domain is by Guo et al. [11], who developed a minimally invasive bone repair material. Their innovative design, a 3D bone repair material, comprises a photocurable polyether F127 diacrylate hydrogel loaded with mixed spheroids of mesenchymal stem cells (MSCs) and vascular endothelial cells (ECs). The MSC-EC-F127DA system demonstrated remarkable potential in promoting bone repair and preserving the alveolar ridge shape, marking a significant stride towards effective ARP procedures [11].
Moreover, emerging biomimetic materials, injectable bone substitutes, and patient-specific implants and materials are pivotal in enhancing ARP outcomes. For instance, injectable bone substitutes have been utilized in a range of studies for alveolar bone regeneration and immediate implant placement post-tooth extraction [28, 29]. Particularly, patient-specific titanium mesh has been recognized as a novel approach for stabilizing the augmentation region using particulate bone substitute materials combined with autologous bone, albeit with noted complications like dehiscence [30]. Moreover, the combined use of xenogeneic bone substitute material covered with a native bilayer collagen membrane has shown promise in alveolar ridge preservation, as evidenced by a randomized controlled clinical trial [31].
These advancements underscore a progressive trajectory in ARP, augmenting dental implant success, aesthetic outcomes, and overall patient satisfaction through the integration of bioactive materials. This sphere of bioactive materials not only holds promise in surmounting challenges posed by traditional materials and methods but also signifies an ongoing quest toward optimizing ARP for varying clinical scenarios.
II. Techniques employed in ARPA. Minimally invasive delivery methodsInjectable bone repair materials are an emergent avenue in bone regeneration and repair, with applications extending to dental and orthopedic domains (Fig. 4A). These materials are crafted for minimal invasive administration, simplifying the operational aspects, and hastening post-operative recovery. They adapt to the bone defect’s shape upon injection, offering a scaffold for bone regeneration.
Fig. 4
Techniques for socket preservation. a Schematic drawing of socket preservation (Image was purchased from Adobe Stock). b Socket preservation in the maxillary canine extraction defect focuses on maintaining the dimensions and quality of the extraction socket following tooth removal
Various substances constitute injectable bone repair materials, including natural and synthetic materials such as calcium phosphate cements, bioactive glasses, and hydrogels. Some of these materials are bioresorbable, allowing for the natural bone tissue to replace the scaffold as it degrades over time. The primary objective is to foster a conducive environment for bone cell attachment, proliferation, and eventual regeneration, a crucial aspect of ARP and implant dentistry [15, 32].
Guo et al. [11] pioneered an injectable bone repair material that stabilizes upon curing. This material showcased active spreading, filling the defect, and offering a robust scaffold for bone regeneration [11]. Recent advancements have also been seen in other types of injectable materials like ternary calcium-based bone cement, which has been shown to promote bone repair [33], and hierarchically degradable bioactive scaffolds that mimic the natural bone repair process [34]. Furthermore, injectable nanocomposite hydrogels, particularly those based on calcium phosphate and alginate, have also shown promise in supporting angiogenic and osteogenic cell functions, which are crucial for bone repair [35].
These novel materials and the associated minimally invasive delivery methods are transcending the barriers posed by traditional graft materials and procedures, heralding a new era of regenerative therapies in dental and orthopedic applications.
B. Comparative analysis of techniques based on the properties of materialsThe conventional techniques for ARP and bone regeneration, including the use of allografts, xenografts, and barrier membranes, have been longstanding practices in clinical settings (Fig. 4B). They have been effective to a certain extent in promoting bone regeneration and ensuring successful dental implant placement. However, they pose challenges such as the risk of infection, longer healing times, and sometimes insufficient bone regeneration, which could hinder the success of subsequent dental implant placement [36, 37].
Novel materials and techniques have emerged with the potential to address some of the limitations associated with conventional approaches. Among these novel approaches are the following:
1.Platelet concentrates: studies have proposed that PRF can be used to support bone regeneration during alveolar ridge augmentation. PRF, combined with bone graft materials, might increase bone regeneration, although the efficacy of PRF in enhancing bone regeneration in ARP remains a topic of investigation [38,39,40].
2.Injectable bone repair materials: as illustrated by the works of Guo et al. [11], injectable bone repair materials provide a minimally invasive approach to bone repair, showcasing significant potential in preserving the alveolar ridge post-extraction.
3.Bioactive materials: these materials, including HA and bioactive glasses, mimic the natural bone structure and composition, fostering better integration and regeneration.
The comparative analyses between conventional and novel techniques have shown varying results. For instance, a systematic review showed that procedures with allografts produced the highest bone percentages at 3 months (54.4%), while those using xenografts yielded the lowest at 5 months (23.6%) [41]. Other studies have compared different ARP techniques such as GBR, socket seal (SS) technique, or unassisted socket healing, revealing radiographic bone changes following ARP [42]. Moreover, some studies have evaluated the combination of different materials and techniques, like combining PRF with different bone graft materials, indicating potential benefits in bone regeneration [39].
Despite the promising outcomes observed with the application of novel techniques and materials, challenges persist. These challenges include the need for standardized protocols, long-term clinical data to establish efficacy and safety, specialized training for clinicians, and understanding the biological mechanisms underlying these novel materials and techniques. The cost considerations, regulatory approvals, and the learning curve associated with the adoption of novel techniques also pose hurdles for widespread acceptance and application in clinical practice.
The field could indeed benefit from multidisciplinary research collaborations encompassing material science, cellular biology, and clinical dentistry. Ongoing and upcoming projects, such as multi-center clinical trials investigating the efficacy of different biomaterials and techniques, hold the potential to further illuminate the path towards optimizing results and improving patient satisfaction in ARP and implant dentistry. Both conventional and novel techniques play pivotal roles in the evolving landscape of ARP and implant dentistry. While conventional techniques provide a reliable foundation, the infusion of novel materials and methods propels the field towards new horizons, fostering a conducive environment for enhanced bone regeneration and successful dental implant therapy.
III. Clinical and histomorphometric outcomesA. Bone maturity, new bone formation, and resorption ratesThe success of ARP hinges significantly on the ability to foster new bone formation, ensure bone maturity, and control bone resorption rates. Here is a more detailed analysis of these factors based on various studies:
1.New bone formation: a study evaluated healing at molar extraction sites and found that using FDBA and an absorbable collagen sponge could effectively preserve the ridge dimension without affecting the amount of new bone formation [43].
2.Bone resorption rates: a 3-year prospective randomized clinical trial aimed to analyze the changes in alveolar bone crest levels and differences in resorption rates between various grafting materials used in ARP post-tooth extraction. The study spanned evaluations over 1, 2, and 3 years of clinical function [44]. Another study observed that alveolar ridge resorption often occurs within the first 6 months post-tooth extraction, with the resorption rate decreasing gradually over the years. This resorption is a crucial factor affecting the longevity and stability of dental implants post-ARP [45].
3.Use of concentrated growth factors: two studies investigated the application of concentrated growth factors (CGFs) in conjunction with other materials for ARP: One study evaluated the effect of CGFs combined with deproteinized bovine bone mineral (DBBM) on ARP during implantology, indicating that this combination might be beneficial for ARP [46]. Another study, a split-mouth, randomized, controlled clinical trial, investigated ARP in post-extraction sockets using concentrated growth factors, hinting at the potential of CGFs in promoting bone preservation and regeneration post-tooth extraction [47].
These studies collectively illustrate the potential of innovative techniques and materials in enhancing bone regeneration, controlling bone resorption, and thus contributing to the success of ARP procedures. However, it is evident that the choice of materials and techniques plays a pivotal role in these outcomes. Further longitudinal and comparative studies could provide more insights into optimizing ARP protocols for improved clinical outcomes.
B. Evaluation of pain management and wound healingIn the realm of ARP, managing post-operative pain and evaluating wound healing is crucial for assessing the overall success of the procedures and ensuring patient satisfaction. Various studies have shed light on different aspects of pain management and wound healing following ARP procedures.
One study compared the wound healing potential and pain management efficacy of collagen and xenograft bovine bone covered by a cellulose mesh when inserted into the socket of extracted teeth [16]. Another study discussed the role of maresin 1, a pro-resolving lipid mediator, in accelerating extraction wound healing, promoting socket bone fill, preserving alveolar ridge bone, and reducing post-operative pain, as tested in a rodent preclinical model [48].
Additionally, a randomized controlled trial evaluated the impact of administering hyaluronic acid gel following ARP procedures in terms of changes in wound dimensions over time, which could be a marker for wound healing [49]. A different clinical trial investigated the effectiveness of amnion-chorion membranes in ARP, including clinical, radiologic, and morphometric assessments of wound healing [50]. Furthermore, a histologic study provided evidence regarding vital bone formation and dimensional changes when different types of bone allografts were used in ridge preservation of non-molar tooth sites, which could indirectly relate to wound healing [51]. The research by Saliba et al. [16] demonstrated that collagen supports a quicker wound healing rate, a higher potential influence on socket healing, and a reduction in pain perception when compared to xenograft bovine bone following tooth extraction procedures. This research insight is valuable for assessing post-operative patient comfort and the wound healing process, which are critical for the overall success and patient satisfaction in ARP procedures.
These studies collectively contribute to a growing body of knowledge that underscores the importance of effective pain management and thorough wound healing evaluation in ARP procedures, which can significantly impact the patient’s experience and the success of subsequent dental implant placement.
C. Impact on subsequent implant placement and stabilityThe prime goal of ARP is to create a favorable milieu for the successful placement and stability of dental implants. Various studies have ventured to elucidate the correlation between diverse ARP methodologies and the enduring success of implants, revealing a positive association between efficacious ARP strategies and enhanced implant stability.
The adequacy of bone volume in three dimensions is indispensable for implant osseointegration, making ARP and augmentation crucial for implant therapy [52]. A particular study highlighted that employing particulate xenogenic or allogenic materials, shielded with absorbable collagen membrane or sponge, was linked with favorable outcomes concerning horizontal ridge preservation [2,
留言 (0)