
記住我


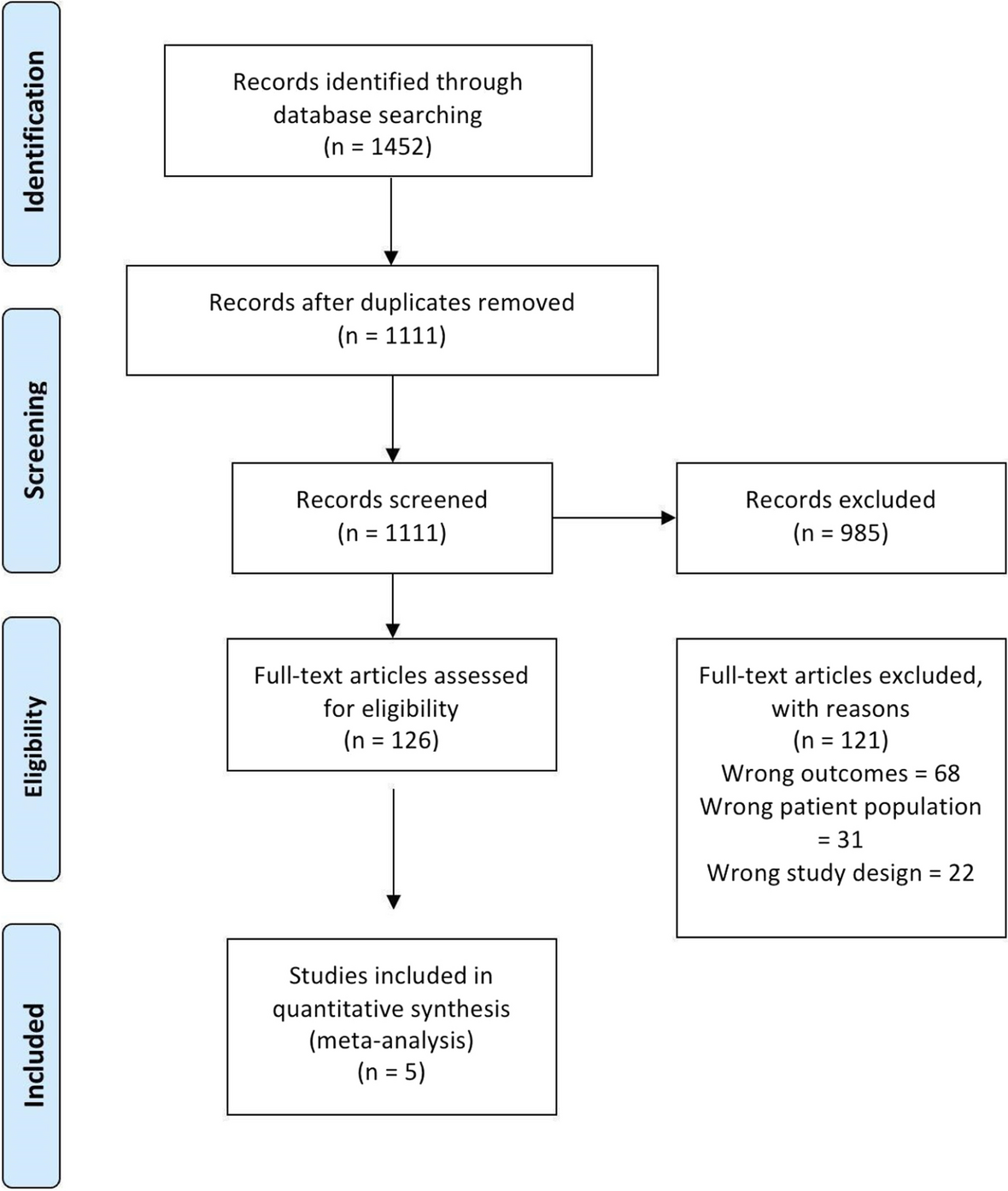


A comprehensive literature search was conducted to identify relevant articles on DA rhinoplasty techniques. The following electronic databases were utilized: Scopus, PubMed, and Web of Science. Inclusion criteria encompassed articles written in English, and the search terms used were a combination of keywords and MeSH, including “graft,” “dorsal augmentation,” “rhinoplasty,” and “surgical techniques.” Studies on surgical and non-surgical approaches, including implants, grafts, and injectables, were considered. The synthesis included a thematic analysis of the various DA techniques, highlighting their advantages, limitations, and reported outcomes. Exclusion criteria encompassed articles not written in English, case reports lacking substantial discussion on techniques, and studies with inadequate methodological detail. Key themes and patterns across studies were identified to provide a comprehensive overview of the current state of DA rhinoplasty approaches.
Who needs the DA rhinoplasty?As a surgical procedure that aims to enhance the appearance of the nasal bridge, DA rhinoplasty is also known as dorsal hump reduction or augmentation rhinoplasty. Rhinoplasty that produces a visible bump or convexity on the nasal bridge is usually recommended for individuals with a dorsal hump. People with prominent dorsal humps often seek DA rhinoplasty to improve the profile of their nose. It could be genetic, trauma-related, or as a result of other factors. Commonly, the procedure is used to improve facial harmony and address aesthetic concerns. If candidates are considering DA rhinoplasty, they should consult with an experienced plastic surgeon or otolaryngologist. An evaluation of the nasal anatomy, a discussion of the individual's aesthetic goals, and consideration of their overall health are all required before the procedure can be performed [1, 4, 5, 15, 23, 24]. There are several reasons why augmentation of the nose may be necessary: dorsal hump or nasal bump: a dorsal hump or nasal bump on the nasal bridge is one of the primary indications for augmentation of the nose. An aging process, trauma, or genetics can cause this hump. A prominent dorsal hump can be smoothed and more aesthetically pleasing with this procedure for individuals who are unhappy with the appearance of the dorsal hump. DA rhinoplasty is commonly performed for cosmetic reasons. The overall harmony and balance of facial features can be significantly affected by a dorsal hump. Several studies have shown that this procedure can greatly enhance facial symmetry and better complement the remaining facial proportions [2, 11, 25,26,27,28,29]. It can be challenging to feel confident and self-esteem when people have aesthetic concerns about their noses. It is possible for patients to feel more self-confident and have a better quality of life after undergoing DA rhinoplasty due to the improved appearance of their face. An obstruction or difficulty breathing may occur as a result of a dorsal hump. As well as improving the appearance of the nasal structure, DA rhinoplasty can improve its functionality by ensuring that it is both functional and aesthetic in design. In deciding to undergo cosmetic surgery, a patient's preferences are crucial. Even though a dorsal hump does not cause functional problems for some people, they may find it bothersome. It can shape the nose to fit aesthetic preferences by having DA rhinoplasty [5, 6, 8, 23, 30,31,32,33,34].
Grafts and surgical approachesMany rhinoplasty surgeons believe that autologous grafts are the best material for grafting. Patient acceptance and low infection rates make autologous grafts a great choice. However, autologous grafts have several well-known disadvantages, including irregular shapes, absorption, donor site morbidity, and aesthetic results that may preclude use in revision or more extensive surgeries [31]. Table 1 summarizes the current technique studies of dorsal augmentation rhinoplasty. Following are explanations of various grafts and surgical techniques.
Table 1 The current technique studies dorsal augmentation rhinoplastyBoneCortical bone grafts are also an option for rhinoplasty. The most common donor sites are the skull, ribs, and iliac crests. For traumatic midface injuries and hypertelorism reconstructions, the skull presents an ideal donor site since it is adjacent to the operative site. For isolated rhinoplasty procedures, other donor sites can be considered. A nasal deformity that cannot be adequately corrected with other graft materials may benefit from bone grafts, as they provide excellent strength and stability. It is very stable and reliable to use bone grafts over a long period [1]. However, because the bone is rigid, it is difficult to shape intraoperatively, requiring saws, burrs, and drills; these tools can create heat that kills osteocytes and denatures growth factors, resulting in graft resorption. In contrast with endochondral bone from other donor sites, such as the ribs and the iliac crest, membranous bone from the skull may not resorb as quickly as endochondral bone from other donor sites. Furthermore, cranial bones can be used because of their proximity to the operation field, and their scarring can be concealed within a hair-bearing scalp [1, 21]. The harvesting of cranial bone grafts can cause alopecia, as well as defects of total thickness, intracranial hemorrhage, and brain injuries. Split cranial bone grafts can be produced in situ or ex vivo from a full-thickness craniotomy segment. As a result of the potential morbidities associated with the donor site, this graft is best suited to surgeons performing craniofacial reconstruction routinely. This approach can be used for midline nasofrontal reconstructions involving craniofacial approaches and possible craniotomies [1].
According to Cizer et al. (2022), inferior turbinate bone grafts are commonly used in rhinoplasty to increase the width of the nose. They approached the lower turbinates in the nose’s lateral wall with an erectile surgical approach. The nasal mucosa has a multilayer squamous epithelium surrounding the middle spongy bone. It is necessary to perform rhinoplasty with a medial flap to harvest inferior turbinate bone grafts. In the inferior turbinate, lidocaine and adrenaline solution are infiltrated after decongestion. Superior and anterior margins of the inferior turbinates are incised mucosally. Medial mucosa elevates along the lower turbinate from its beginning until its horizontal part. Using Heymann nasal scissors, the lower turbinate and lateral mucosa are excised. The excision is completed by directing the scissors inferiorly before reaching the posterior attachment point of the lower turbinate. From the periosteum, the inferior turbinate’s lateral mucosa is peeled extracorporeally. The inferior concha bone is crushed with a straight Kelly clamp to achieve the desired shape. With scissors, people can make the necessary corrections again. As soon as the septum and dorsum are completed, the prepared ITBG is positioned in the planned area. A saddle nose deformity is caused by insufficient septum cartilage in trauma and granulomatous diseases. Thus, ITBG is designed primarily for the reconstruction of saddle nose deformities. Similar to septal cartilage grafts, nasal DA also has increased indications. There have also been successful results using this technique for minor dorsal deficits. During IT, the insertion should be advanced inferiorly so as not to damage this branch. Some cases require postoperative nasal packing or cauterization. It is typically detected and controlled intraoperatively. In addition to mucous cysts, turbinate bone mucosa can cause a mucous cyst in the nasal dorsum. A mucous cyst that has developed requires total excision. Apart from the postoperative care and applications for septorhinoplasty, there is no need for special care or precaution for patients undergoing ITBG. Four years of follow-up revealed no evidence of graft resorption [13].
The study by Mehta et al. (2021) discusses their experience using olecranon bone grafts in severe saddle nose deformities. Twelve patients underwent olecranon bone grafting on their dorsal nasal augmentations between 2011 and 2020. During the surgery, grafts were inserted through old nasal dorsum scars in all ten patients with congenital deformities. At the nasion, in both cases, the grafts were fixed with screws. X-rays of the nasal bone and clinical photographs were used to assess each patient's graft resorption postoperatively. A nasal DA with Olecranon bone graft exhibits minimal donor area morbidity and simplifies harvesting. The Olecranon cortex should be thick enough to allow custom molding and resist resorption over time, thus providing a desirable outcome [56].
An evaluation of freeze-dried cortical allograft bone for nasal dorsal augmentation was performed by Clark et al. (2019). This is an analysis of 62 patients over 10 years following the 42 months. Sixteen out of 19 allografts showed objective evidence of continued volume or neovascularization. According to the patients’ subjective opinion, 37 out of 43 grafts were reported to have had volume persistence. An overall success rate of 85% was achieved. Allograft bone made from freeze-dried allografts can be used safely and effectively as a substitute for human bone donated. Whether allograft bone can be partially demineralized so that it can be carved with a scalpel can be confirmed in future studies for young patients needing long-term reconstruction [57].
CartilageA good graft material for dorsal augmentation is autologous cartilage. A variety of cartilage contains autologous tissue, including conchal bowls, nasal septums, lateral crura, and costa. Biocompatible materials can be used to wrap cartilage grafts with Surgicel. Due to its original publication, medical cartilage wrapped in Surgicel is also called a Turkish delicacy. The most common complications with autologous cartilage include graft resorption, infection, and implant migration. In the case of revision or secondary rhinoplasty without autogenous cartilage, special care must be taken [31, 58, 59]. Studies assessed the effects of secondary rhinoplasty on patients with cleft lip and palate. An onlay tip graft, columellar strut implant or graft, and lower lateral cartilage repositioning were all included in rhinoplasty procedures. The septum and concha were harvested for cartilage, while the ribs were not used. As part of the research, the Rhinoplasty Outcome Evaluation (ROE) survey was administered, the Mortier scoring scale was modified, and 8 intranasal symmetry measurements and 4 nasofacial measurements were measured. A comparison was made between preoperative and postoperative patient satisfaction and nasal esthetics [41, 60,61,62,63].
Auricular cartilageNear the nose, the ear is a readily available cartilage donor site. This graft is considered viable since it is nearby and easy to harvest. Both ears can be harvested to get enough cartilage, and septal cartilage can be preserved when auricular cartilage is used. Unlike secondary donor sites, there is no need to include the ear in the primary site. The conchal bowl can be harvested anteriorly and posteriorly. The nose’s dorsum cartilage can be augmented by 3 to 6 mm. The best results are not always possible when handling auricular cartilage. The natural curvature of auricular cartilage makes dorsal nasal profiles difficult. This material is brittle, elastomeric, and lacks rigidity in structural applications. Furthermore, scar contractions can occur due to auricular cartilage's inherent memory and propensity for resorption [1]. Various reconstructive procedures, such as aesthetic rhinoplasty, can benefit from Auricular cartilage grafts, according to Zinser et al. (2013). This study evaluated the clinical viability, indications, and morbidity of tragal cartilage and auricular cartilage from concha and scapha in rhinoplasty. There were 170 grafts in total between 150 augmentation rhinoplasties. Trachus, concha, and scapha were the sites of donor tissue. Pearson's intraclass correlation was used to assess intraobserver reliability. Scapha harvesting time averaged 27 (8) min, tragus harvesting time 4.5 (1.4) min, and concha harvesting time 5.7 (1.6) min. In order of size, the concha, tragus, and scapha provided the largest grafts. Tips, columella struts, shields, rims, and dorsal onlays were all grafted [64].
Costal cartilageDermofat grafts absorb more quickly than nasal cartilage and provide significant volume. Carving and placing the graft requires high skill, even though harvesting the cartilage can result in pneumothorax and chest wall scarring. Dermofat or diced cartilage can produce a much better shape with a better definition and predictability when performed by an experienced surgeon. Compared to septal extension grafts, dorsal augmentation requires more costal cartilage. Because it is longer and straighter, the seventh rib cartilage is ideal for augmenting the dorsal area. There are inframammary folds that prevent access to the seventh rib cartilage. Costal cartilage must be carved for DA. Perfect fit requires precise carving. The graft will develop deviations if the operator cannot carve it to the correct dimensions and shape. DA is required for most Asian patients with low dorsums. Warping of the graft is minimized by carving the core cartilage concentrically [5, 65, 66]. As part of their research, Lee et al. (2021) reviewed all patients who underwent rhinoplasty with crushed autologous costal cartilage used for dorsal augmentation. A photo before and after three facial plastic surgeons used the procedure to evaluate its success. The level of satisfaction of patients was also assessed. Postoperative complications were investigated, as well as anthropometric measurements. 39.5, 47.45, 13.1, and 0.0% of facial plastic surgeons' evaluations were excellent, good, fair, and poor results. In 42.1, 39.5, 15.8, and 2.6% of cases, patients were delighted, satisfied, moderate, and dissatisfied. In the postoperative period, there was a noticeable increase in the heights of the dorsum and radix. Dorsum complications included 28.9%, surface irregularities, five resorptions, and two short noses. Crushed autologous costal cartilage can significantly increase the nasal dorsum. When surgery is indicated, this technique may be a better alternative due to the high rate of complications at the recipient site [30]. In a study by Toriumi et al. (2017), autologous costal cartilage or micro fats were used to augment the dorsum with autologous cartilage. With the increasing demand for augmentation rhinoplasties and the increased use of graft materials for structural rhinoplasties, costal cartilage grafts are becoming more popular. In dorsal grafting, costal cartilage is an art and a science. Dorsal grafts are carved to match the contour of the nasal dorsum. A contoured graft must be fixed to the bony dorsum and contoured according to the patient's desires to minimize the risk of warping and displacement. There is a discussion of the different types of dorsal grafts and how they are fixed. Dorsal grafts are fused to the perforated or rasped nasal dorsum through the perichondrial interface. This creates a natural-looking and immobile nasal dorsum. Fixing the dorsal graft decreases warping and deformity. In rhinoplasty, microfat could camouflage compromised tissues and promote healing. A surgeon can enhance soft tissues by injecting micro-fat into an open surgical field, promoting healing and enhancing healing effects using MISTA. After injection into soft tissue carriers, a microfat implant is placed into the surgical field. The use of MISTA in cosmetic and reconstructive surgery is tremendously beneficial [6].
An article by Yoo et al. (2019) discusses conventional and recent applications of costal cartilage in Asian rhinoplasty. Costal cartilage has been used for Asian rhinoplasty techniques in different studies. There are two types of costal cartilage commonly used for dorsal augmentation: solid-block cartilage and diced cartilage. Surgeons have reported numerous types of grafting techniques for tip and septum reconstruction. Surgeons should consider both donor-site morbidity and graft complications when performing costal cartilage grafts. Several strategies have recently improved the prevention of these complications [67]. Warping after ACC implants is the most common complication reported by Miranda et al. (2013). Three patients received monoblock ACC implants, and one received laminated ACC implants in the present patient group. The second most common complication was resorption in the ACC group. All four patients who had resorption received monoblock augmentation in this study. Surgeons should remember that resorption can occur with any dorsal costal cartilage implant [30]. According to Yilmaz et al., previously, ACC was used for dorsal enhancement without high resorption rates, and the shape of the nose was satisfactory. Future studies are needed to clarify this discrepancy [3].
A study by Ujamet et al. (2123) concluded that autologous costal cartilage was an excellent graft material for nasal reconstruction as it provided both volume and quality. Most commonly, costal cartilages from the 5th- 8th ribs are harvested for augmentation grafts. Despite this, the 10th rib offers excellent graft potential and is often overlooked. Using rib cartilage to repair secondary cleft nasal deformities has rarely been documented in the literature. Their simple and rapid technique makes rib cartilage worthwhile for secondary rhinoplasty and nasal deformities caused by cleft lips. Researchers have demonstrated the ease of harvesting, the stability, and the predictability of outcomes using the 10th rib cartilage in several clinical cases. Various challenging secondary cleft rhinoplasty procedures with excellent results have been successfully performed with the 10th rib graft by the senior author. Several advantages make the 10th rib graft a good option for such procedures, including its easy harvestability, dynamic cartilage properties, and predicted outcomes [68]. Using autogenous cartilage grafts to enhance rhinoplasty, Leach et al. (2018) reported long-term patient-reported outcomes after open augmentation rhinoplasty with autogenous cartilage grafts. An overview of operative steps and perioperative care was provided to optimize results. From 2008 to 2016, 11 such augmentation rhinoplasties were reviewed retrospectively. An advanced cosmetic westernization of the nose was indicated in cases of saddle nose deformity, the post-traumatic collapse of the nose, and post-traumatic nasal deformity. In this study, a patient questionnaire was used to measure the long-term outcomes as reported by the patient. Nose shape, position, and function improved significantly in all patients. As a result, there were no cartilage exposures, warpings, or resorptions and no recurring deformities. A second correction was successful with the above technique for a patient whose dorsal graft fractured 2 years later. It took 5.2 years on average for the study to be completed. In the follow-up questionnaire, 100% of nine patients expressed satisfaction with the appearance of their noses. No nose problems were reported by 100% of respondents during follow-up. A low-volume operator successfully performed augmentation rhinoplasty with L-shaped costal cartilage grafts for diverse indications. This technique can provide long-term patient satisfaction and pleasing aesthetic results [69].
Septal cartilageDorsal augmentation is often performed with septal cartilage. Due to its rigidity and flat, planar geometry, this graft is easily carved into any other nasal tip graft. There is a limited supply of septal cartilage. With smaller noses, surgeons have less septal cartilage available for DA procedures. A traumatic injury or revision rhinoplasty that already damaged septal cartilage makes the situation worse. Slightly deviated septums can also make harvesting grafts difficult. Over-resection of the septum can lead to septal perforations, and not considering the septal lining can compromise the structural integrity of the nose. In sufficient quantities, septal cartilage remains popular as a graft [1]. CCDG grafts were evaluated by Lee et al. (2022) for their postoperative feasibility. A retrospective review of 38 rhinoplasty records of patients who underwent an open approach to DA was conducted. Twenty patients (52.6%) received CCDG graft compared to 18 with DG graft (47.4%). A study comparing anthropometric data from facial photographs with satisfaction questionnaires analyzed aesthetic outcomes and palpable irregularities on the nasal dorsum after surgery. There was a successful outcome for both groups in terms of aesthetics. After surgery, there was a more significant increase in dorsal height, radix height, and tip projection compared to preoperative data. Rotation of the tip was not significantly increased. Both groups had significant palpable irregularities, although aesthetic satisfaction was similar. A significant difference was seen between the CCDG graft group and the DG graft group regarding dorsal irregularities. Furthermore, two surgeons evaluated the CCDG graft group significantly better than the DG graft group regarding the degree of irregularity. A revision rhinoplasty was not performed on any of the patients who complained about an irregular dorsum. An alternative to irregular dorsum complications can be achieved with CCDG grafts [70].
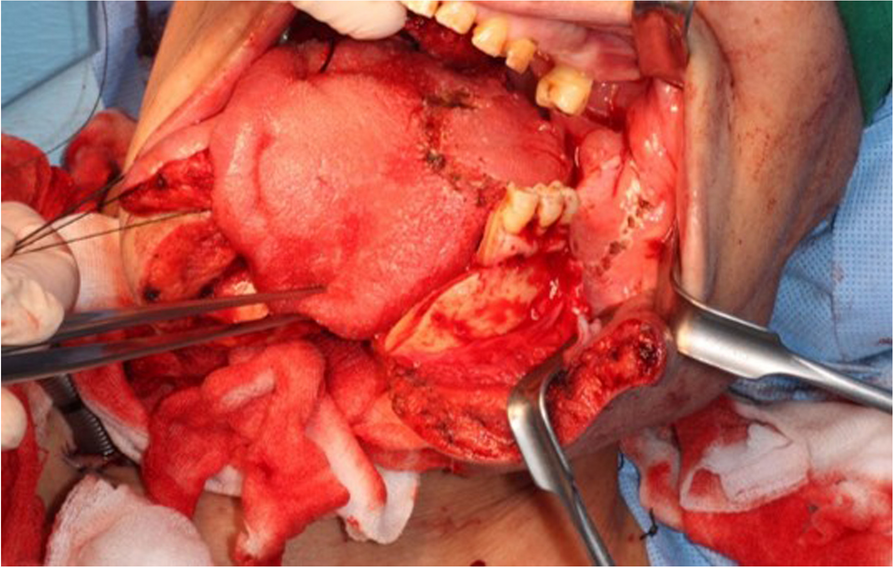
Lee et al. (2016) defined a septal L-strut to prevent the collapse of the nasal dorsum as pressure moves from the rhinion to the supratip breakpoint. Using computed tomography, a model of the L-strut with a width of 1 cm was developed. If the superior L-strut is to be preserved, at least 45% of it must be preserved. To prevent collapse or distortion of the caudal L-strut, augmentation rhinoplasty must preserve or reinforce it. As the DA material moves toward the supratip breakpoint, an augmentation pocket must hold it. To better understand why target tissues deform and collapse, clinicians used a numerical analysis utilizing a FEM-based model [71]. Ahn et al. (2019) introduced a new septal extension graft using a cartilage-bone complex and cartilage. An external approach and sedative anesthesia were used for all operations. The perpendicular plate of the ethmoid bone and septal cartilage were harvested through septoplasty. A “sandwich technique” differs from other SEGs14 by using linked septal cartilage and bone instead of inserted bone between layers of cartilage (Fig. 1). A complex cartilage-bone projection and lengthening was created by two layers of cartilage on each side. Creating strong fixation, the double-layered cartilage portion of the L-strut was placed on the caudal septum of the L-strut and the bony portion on the tip side. During septorhinoplasty, 30 consecutive patients were treated. All procedures were performed using a sandwich technique that combined cartilage with bone. External approaches were used in all cases, and septoturbinoplasty was also performed. Additionally, 21 osteotomies, 10 augmentations using silicon, 10 augmentations using Alloderm, and 7 paramaxillary augmentations were performed with tip plasty. The surgery results were satisfactory for all patients (Fig. 2). According to specialist opinions, there were three excellent and 23 good cases. There were 26 successful surgery outcomes, including excellent and good outcomes. No case was poor, and four cases were fair. Twenty-four cases resulted in no complications, three resulted in notable transcolumellar scarring, three resulted in mild nostril asymmetry, and one resulted in cartilage gauziness. As of the study’s follow-up period, there were no cases of infection, nor were there any cases requiring reoperation. Using cartilage and bone complex, the sandwich technique can be very effective for Asians with weak nasal tips [72].
Fig. 1
Techniques of surgery and anthropometric measurements. An illustration of a bone and cartilage complex (left). NLA, nasolabial angle; NTP,nasal tip projection; NL, indicates nasal length; CLA, columella-lobular angle; NFA, nasofrontal angle. Reprinted from ref [72] (Open Access Contents)
Fig. 2
A and C, E, and G Photographs of the face taken before surgery. B, D 10 months. F, H 12 months after surgery. Reprinted from ref [72] (Open Access Contents)
Ear cartilageEar cartilage is often used in rhinoplasty. Different methods have been used to harvest, prepare, and apply conchal cartilage grafts. It is readily available and accessible. Due to its elasticity and intrinsic curvature, ear cartilage is unsuitable for weight bearing. As a result, conchal cartilage is commonly used as a stacked or fascia-wrapped DA graft. Conchal cartilage diced with attached perichondrium is suitable for patients with moderate to thick skin and little risk of infection. Segmental dorsal grafts can enhance a mildly flat nasal dorsum or repair a sunken supratip. A large piece of conchal cartilage must be harvested for a full-length nasal augmentation. Convex shapes can be cut from large pieces and stacked to eliminate their natural curve. Long-term DA using such methods may leave the graft visible. It is not recommended to use conchal cartilage for severe dorsal deficiency [34].
Conchal cartilageSecondary or reconstructive rhinoplasty can benefit from conchal cartilage grafts because they are easy to harvest and produce good results in the long run. The conchal cartilage has several anatomical characteristics, and the harvest technique is well-documented. Conchal cartilage’s intrinsic curvature makes it a poor material for DA due to its inability to produce symmetrical results. Additionally, the conchal cartilage rarely yields a piece large enough for a single piece of dorsal augmentation. Conchal cartilage has an intrinsic curvature, which can be overcome by multilaminar cartilage. Conchal cartilage is intrinsically irregular but becomes apparent after surgery. This problem has also been avoided using conchal cartilage divided and wrapped in fascia, which has gained widespread acceptance as an ideal method for DA [73]. With conchal cartilage, it is possible to augment the nasal tip similarly to LLC. Due to its inherent curvature and limitations in length, conchal cartilage has limited usage as a DA material. A large amount of cartilage must be harvested to augment the nasal tip and radix with conchal cartilage. Stacking multiple layers of a convex shape eliminates its natural curvature. The graft will be visible over time when DA is performed through such methods. DA often uses wrapped diced conchal cartilage or conchal cartilage. Hematoma and keloid formation are likely at the donor site when using conchal cartilage for substantial augmentation. The recipient may also develop irregularities in their dorsal surface, graft resorption, and infection [74].
Using retroauricular fascia and conchal cartilage, Varedi and Bohluli (2015) developed a composite graft. For dorsal augmentation, especially segmental augmentation, diced conchal cartilage compared well to intact perichondrium, according to the senior author of this paper [75]. The augmentation of the dorsal region with diced conchal cartilage wrapped in Surgicel was reported in Erol (2000) [76]. Dorsal enhancement can also be achieved quickly and conveniently with diced cartilage and warm blood, as Codazzi and colleagues (2014) reported [77]. By using diced cartilage grafts wrapped in temporalis fascia, Daniel (2008) modified its application. Because this procedure is easy to prepare and results in less resorption, it has gained popularity over the past decade [78]. A fibrin glue graft with diced cartilage provides favorable aesthetic results and a low resorption rate, according to Tasman (2015) [79].
Varedi et al. (2015) presented their experiences with augmentation of the dorsum using conchal cartilage and retroauricular fascia. Study participants had moderate to severe dorsal deficiencies. An auricular cartilage and postauricular fascia biopsy was performed through the postauricular sulcus. A layer of conchal cartilage was used if there was a moderate amount of dorsal deficiency. More severe deficiencies required a multilayer conchal graft, which superimposed cartilage pieces. 6-0 polydioxanone (PDS) sutures were used to attach cartilage segments. The cartilage segment was then fixed to the postauricular fascia with 6-0 PDS sutures. It was necessary to undermine the nasal dorsum to place chondrofascial grafts carefully. Following functional disorders, chondrofascial grafts were inserted in the dorsal pocket after tip plasty and lateral wall osteotomies. This study included fourteen participants. It took an average of 25.4 months to complete the follow-up. There was a wide range of ages among the patients. The grafts were not reabsorbed, displaced, or asymmetrically reabsorbed in the second week. Neither the donor site nor the postoperative scar was visible. The donor sites were affected by mild ecchymosis in eight patients. A small amount of graft resorption was observed in three male patients. Performing revision surgery on these patients was unnecessary because the esthetic results were not compromised. Composite turbinate cartilage and retroauricular fascia grafts were effective in patients with moderate to severe nasal dorsal deficiency [80]. Kim et al. (2015) studied diced conchal cartilage attached to the perichondrium to augment nasal dorsums, radixes, and tips. The records of 37 patients with diced conchal cartilage and perichondrial attachments inserted into the nasal dorsum, radix, or tip were reviewed. Face-to-face comparisons of pre- and post-operative photographs were used to assess postoperative surgical outcomes. The analysis also included complications. A valuable graft material in rhinoplasties is diced conchal cartilage with perichondrial attachment [81].
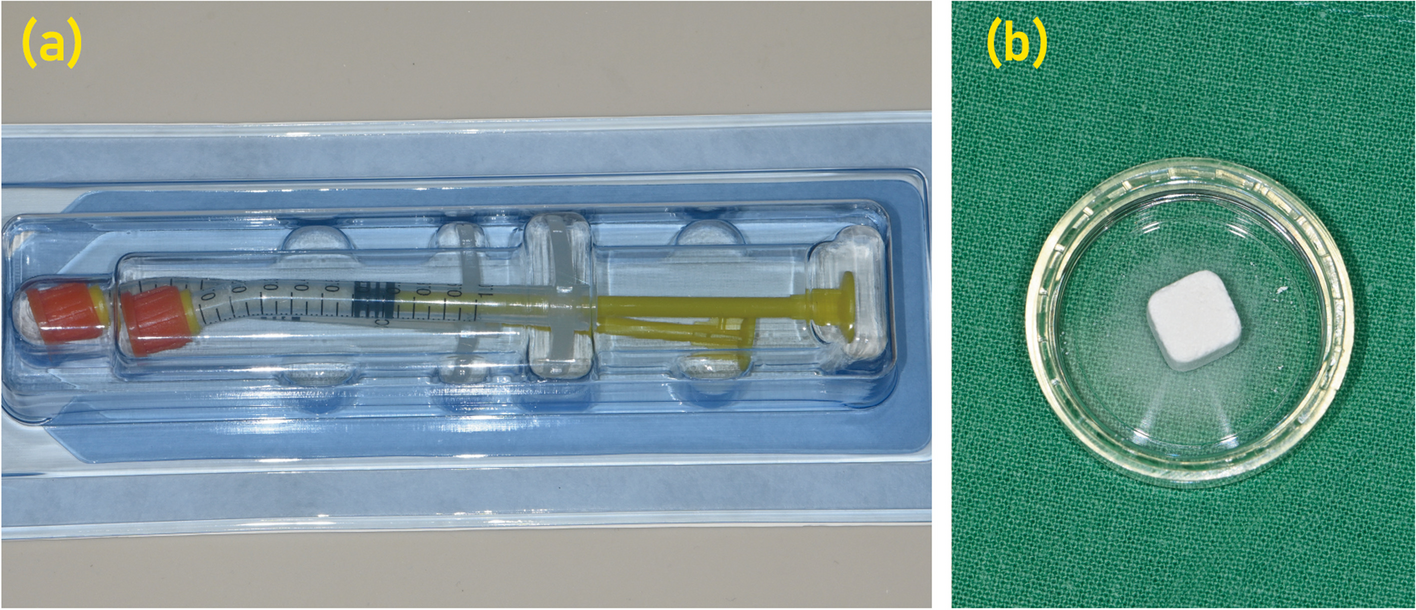
Diced cartilage with fascia graftCostal cartilage provides enough cartilaginous material to augment the low dorsum of Asian patients, making it the best cartilage graft for significant dorsal augmentations. However, solid block costal cartilage grafts can warp and show through thin skin. In addition to wrapping diced cartilage in the temporal fascia, diced cartilage can also be used to overcome such drawbacks. Silicone implants have replaced diced cartilage grafts that were used decades ago. The researchers, however, found the graft undergoes total resorption and attributed the process to foreign bodies reacting with Surgicell. Their report describes a modified method of wrapping diced cartilage in temporal fascia. It is easy to perform and results in a lower resorption rate, making the method readily adopted by numerous surgeons. Diced cartilage grafting effectively removes dorsal irregularities or enhances the dorsal area [5]. Diced cartilage grafts are unpredictable regarding resorption, which can result in overcorrection and under-correction. The extent of augmentation provided by diced cartilage grafts is limited, which prevents them from providing structural nasal support. Larger grafts have a greater migration risk, whether the entire graft or the diced cartilage itself, which can result in palpable and visual irregularities. Diced cartilage can also result in “amorphous” aesthetic lines due to its nature, unlike more rigid alternatives that produce more precise contours due to its rigidity. Several reports have described dermal scarring that leaves the overlying skin looking like cobblestones, especially in thin-skinned patients. For those who require moderate amounts of augmentation between 1 and 4 mm, diced cartilage does present a viable option for DA [1]. An easier way of using GDCG was developed by Yoo et al. (2022). A novel mold for DA is described here about GDCG. DA with molded GDCG was used in the study on 80 patients. Reviewing facial photographs and medical records assessed postoperative complications and patient satisfaction. To examine changes in implant widths and heights over time for 23 patients who underwent three-dimensional scanned imaging, dorsal widths and heights were measured at the radixes and rhinions. After 3 months, the latest follow-up photograph was compared with the 3-month postoperative picture to assess graft resorption. Three-dimensional scanned images were used to assess the change of the dorsum over time. Surgery was found to be successful for 66 of the patients. Nineteen patients experienced complications, and 8 had to have their procedures revised. As a result of
留言 (0)