This study, as far as the authors are aware, is the largest study of BD patients (N = 2649) within the UK to estimate the rate of BD relapse over a 5-year period. The rate of relapse in this study was 25.52% over a 5-year period. This rate is comparable to previous naturalistic studies (please see Additional file 1) that have assessed BD relapse rates, such as the US-based, STEP-BD study (Perlis et al. 2006), which calculated a 1-year relapse rate of 48.5% and in Vázquez et al.' s (2015) review paper (Vázquez et al. 2015), which estimated recurrence rates of 26.3% among the naturalistic studies (n = 10) reviewed.
To date, O’Hagan and colleagues (2017) appears to be the only naturalistic UK study to estimate BD relapse rate. Compared to our current study, O’Hagan et al.'s (2017) study noted slightly higher rates of recorded substance misuse (14.1% vs 11.5% in the present study; please see Additional file 1), which may have increased the rate of bipolar relapse they found—i.e. increased rates of substance misuse may have escalated the deterioration of a person’s mental health leading to additional hospitalisation. Another possibility is that our data may be underestimating the true rate of relapse for people with BD residing in Birmingham. For instance, it is possible that not all instances of BD relapse may have precipitated an admission to hospital or a referral to crisis services. Indeed, Hong et al.’s (2010) study reported that only 60% of relapses were re-admissions to hospital. Community mental health services may have managed and attenuated relapses, as opposed to sparking additional referrals to crisis teams/ inpatient admissions. Our study therefore adds value by exploring relapse (normally defined in research studies as hospitalisation) within a routine healthcare system, and with relapse being clinician assessed.
Further, a striking proportion of deaths were reported in our study. Out of the 2649 patients at baseline, 7.2% of this sample (n = 190) had died during the 5-year follow-up; a figure which supports findings from previous BD cohort studies (Hayes et al. 2017). Based on these figures, the death rate among BD populations appears to be higher than the death rate among populations with other serious mental health conditions, such as treatment-resistant depression and schizophrenia, which appear to be around 5.05% (e.g. Madsen et al. 2021) and 2.7–4.1% (Kurdyak et al. 2021), respectively. BD patients consistently show an average reduced lifespan compared to the general population (Staudt Hansen et al. 2019) and our findings further highlight the need for better treatment for this neglected population.
The second aim of this study was to examine the potential factors associated with relapse status and the number of relapses during the 5-year period. Results showed that after controlling for several sociodemographic variables, a reported history of deliberate self-harm/suicidality, having a comorbid mental health diagnosis and the presence of psychotic symptoms, at either first recorded diagnosis or relapse, were all significantly associated with experiencing a relapse episode over the 5-year period (i.e. at least one relapse). Further, when examining factors associated with the number of relapses over the 5-year period, a reported history of deliberate self-harm/suicidality, trauma, the presence of psychotic symptoms (at either first recorded diagnosis or relapse), comorbidity and ethnicity, were all significantly associated with a higher number of relapses during the 5-year period, suggesting the robustness of our findings.
Combined, these findings highlight four potentially modifiable targets for future BD interventions centred on reducing: (1) rates of self-harm/suicidality, (2) the damaging effects of trauma, (3) rates of mental health comorbidity and (4) targeting the reduction of psychotic features within BD. These current results support a plethora of research highlighting the high prevalence of self-harm/suicidality (Clements et al. 2013) and psychiatric comorbidity, particularly anxiety disorders (Simon et al. 2004), among people with BD. Comorbid anxiety disorders specifically pose a unique treatment challenge for BD patients, given that SSRI antidepressants and others used to treat anxiety, can increase the risk of relapse in BD. Similarly, there are high levels of comorbidity between BD and borderline personality disorder (Durdurak et al. 2022) and attention deficit hyperactivity disorder (Schiweck et al., 2021). Other than pharmacological treatment or disorder specific psychological therapy, another approach to combating the high rates of comorbidity present in BD, and potentially helping to reduce relapse rates, is to adopt transdiagnostic treatment protocols for BD patients. Early feasibility trials assessing transdiagnostic approaches show promising results (Perich et al. 2020), however, further research, such as RCTs, are needed to better determine their effectiveness. Network analyses, which provides centrality statistics that indicate how variables are related to others in the network, may also be useful for BD given that symptoms overlap with various other psychiatric disorders (Scott et al. 2021). Further, within BD cases, the presence of psychotic symptoms is a common phenomenon (Dell’Osso et al. 2017) and has previously been identified as a potential risk factor for bipolar relapse (Carlson et al. 2012), as it likely represents a more complex and severe form of bipolar (Elowe et al. 2022).
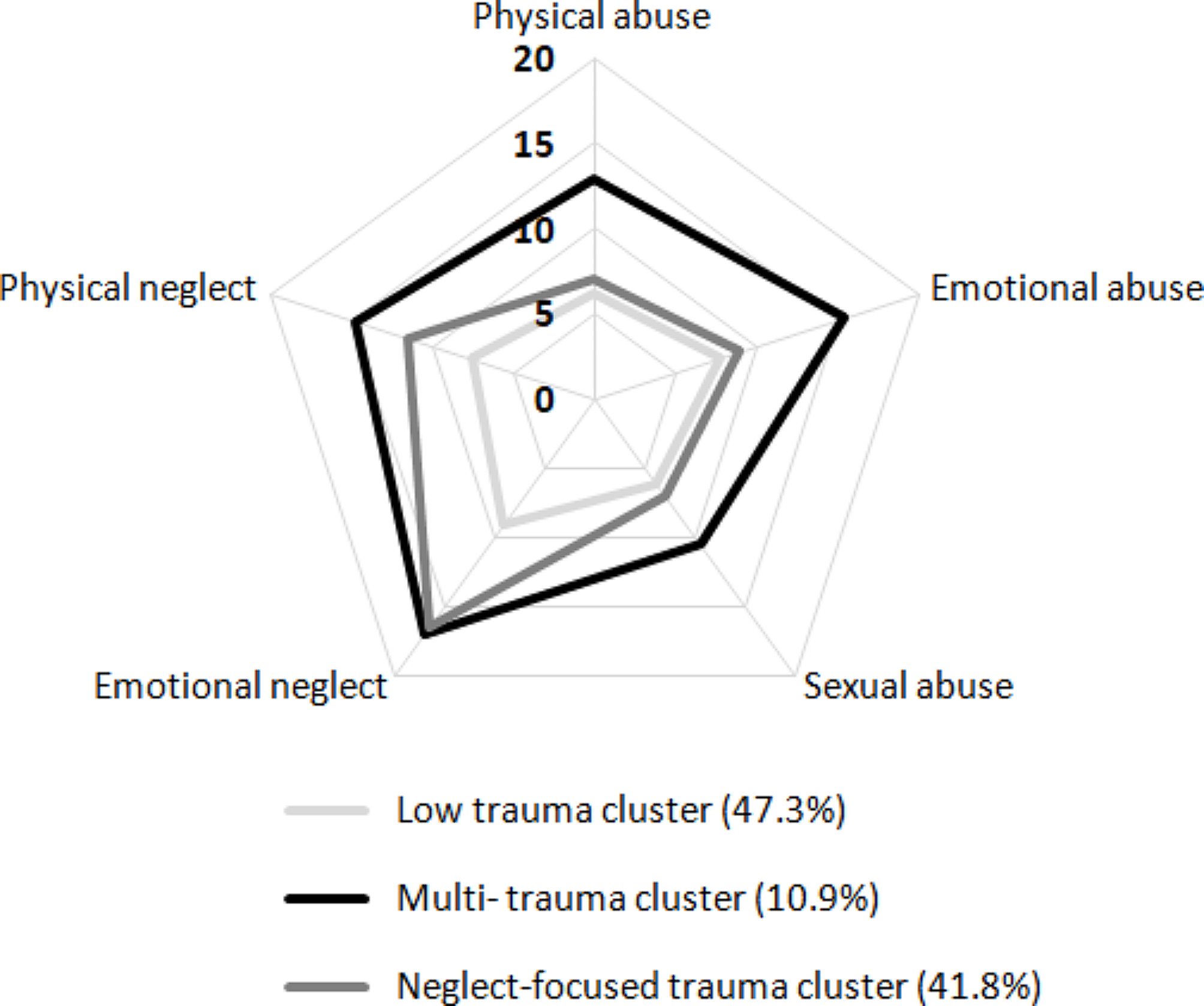
A burgeoning area of research demonstrates the significant role that trauma exposure, particularly during childhood, plays in the onset and trajectory of BD (Aas et al. 2016). Agnew-Blais and Daneses’ (2016) meta-analysis (Agnew-Blais and Danese 2016) shows that the course of BD is more pernicious and complex when individuals have been exposed to childhood trauma. This has been observed by markers such as an earlier age BD onset, the presence of psychotic features, cognitive impairment, rapid cycling, suicidality, greater depressive symptoms, poorer global functioning, increased number of mood episodes, greater comorbidity, and a poorer response to front-line biological treatments, such as lithium (Aas et al. 2016). Thus, the idea of trauma-focussed interventions for BD patients is gaining traction (Hett et al. 2022), and this current study further supports this idea by showing that trauma exposure in BD patients is also associated with relapse outcomes.
Strengths and limitations
This study has several strengths, the first being its large sample size. Additionally, unlike in RCTs, the naturalistic data here arguably provides a more clinically valid account of relapse rates, as it includes BD patients with more complex presentations (e.g. comorbid diagnoses) that are routinely seen in secondary care. It is also important to point out that our data is capturing clinician-defined relapse, and that all data used has been entered and completed by healthcare professionals, thus providing an invaluable insight into the service provision and journey to recovery (or otherwise) experienced by patients with BD. However, there are some limitations to note. Within the UK and the NHS healthcare system, the treatment of BD, as with other complex and severe forms of mental illness, routinely falls under secondary care mental health services, especially for people with more severe forms of the condition. However, being provided treatment within secondary care does not exclude management within primary care. A proportion of BD cases may either first present themselves within primary care (e.g., via GP appointment) or indeed, following discharge from secondary care services, those with BD may prefer to have ongoing medication management within primary care (NICE 2022). Secondary mental healthcare management is the predominant option for those with BD who are more unwell, and as a result, our data may be biased towards that group, and not be generalisable to people with more milder forms of BD. By default, our methods used a calendar-based approach to cohort definition, meaning that data is available on large numbers of patients who have a diagnosis of BD and are receiving routine care within secondary mental health services. This provides much needed valid data on the progress and outcomes of people with BD and avoids the well-known issues of lack of generalisability of research cohorts. The limitations of using our electronic health records approach, is that data on variables that could be of interest to modelling, such as presentation on index episode, are not reliably available, and our results should be considered in this light. As the analyses are based on electronic health records within an NHS Trust, we can only analyse data that has been recorded and documented. For instance, to obtain a BD diagnosis date in this study, we selected the earliest recorded bipolar diagnosis date for each patient. However, as outlined by the data in Table 1, it is likely that patients may have received their true BD prior to this date, and if so, this would skew the time from diagnosis to relapse variable computed in this study. Some other important associations/predictors of relapse were inevitably not available in the data, such as cognitive impairments (Miskowiak et al. 2022) or early age illness onset (Davarinejad et al. 2021). Further, whilst the data has strong ecological validity, there may be differences with studies that have used research assessments. We would view these different approaches as providing complimentary data. Finally, the available data does not include information from some mental health services providing care to young people under 25 years, this being provided by an organisation from which we could not obtain data. As such, our data does not include information on crisis team presentations and some inpatient admission. Therefore, the relapse rate found may be an underestimate of the total BD population. However, although the rate of paediatric BD diagnosis has doubled in outpatient clinical settings (Meter et al. 2011), the peak incidence for most people with BD is 25 years and over (Bellivier et al. 2003), and there is a well-recognised diagnostic delay of 8–10 years; so the extent of our underestimate is difficult to know. Our results are most valid for people who are over the age of 25 years.
Future research
Given the benefits linked to using naturalistic data such as electronic health records, future research may benefit from adopting a machine learning approach to better predict who may relapse and why. Recent work has utilised machine learning approaches to pinpoint important predictors to depressive relapses in BD (Siqueira et al. 2021) using the STEP-BD dataset. However, replicating this approach within a large UK mental health Trust would be advantageous to better determine relapse risk factors and aid decision-making in the treatment and prevention of BD, specifically within the UK. Additionally, future research would benefit from further examining the comorbidity of physical health conditions within individuals diagnosed with BD to better understand the treatment needs and outcomes of this group and offer better insight to healthcare professionals on ways to tailor treatment approaches for this patient group.


留言 (0)