
記住我
“[at home] everybody is the real self (…) you cannot cheat yourself here, you are what you are when you are at home.”—Parent #3
Traditional laboratory-based child health research is constrained by cross-sectional measurements, retrospective reporting bias, lack of ecological validity, and systematic exclusion of families with accessibility needs. The COVID-19 pandemic has accelerated the need to move research out of the laboratory and into the community. Community-based data collection methods, such as Ecological Momentary Assessment,1 salivary cortisol collection,2 and actigraphy,3 have been largely validated in adult populations, without engagement or involvement of individuals with diverse developmental abilities.4 Advances have been made in establishing the feasibility and acceptability of Ecological Momentary Assessment in children and youth on the autism spectrum but have not included individuals with significant cognitive or motor impairments.5–7
Families of children with medical complexity demonstrate substantial creativity in developing “workarounds” for barriers associated with providing care.8 Cocreation with families allows us to harness this expertise in designing in-home data collection to fit the unique context of their lives, with tangible benefits to the research and families. Kramer-Roy9 describes that this type of participatory research, that centers the needs and voices of individuals with lived experience to give them control over the research process and outcomes, can serve an emancipatory role. A recent review found that children and young people with disabilities, particularly those who experience social marginalization and who have more complex medical, social, and communication needs and are frequently disempowered in their lives, are often excluded from participatory approaches to research.10
To address these gaps, we undertook a qualitative study, based on a living lab approach,11–13 to solicit family input in developing a community-based research platform to advance our ability to study behavior and development in children/youth whose abilities come from across a developmental spectrum. Qualitative approaches have been described as an ideal framework to inform patient engagement in pediatric rehabilitation research because of the focus on relationship building while attending to power imbalances, reflexivity, and coconstruction of meaning.14 Although there is debate regarding whether qualitative research itself should be distinguished from patient engagement,15 there is a history of using qualitative research as patient engagement in the context of codesign.16 The present research was part of a broader initiative to establish a “Living Lab at Home” platform for children and youth that offers researchers, clinicians, and families the tools to engage in longitudinal, multimodality, home-based data collection, appropriate for a wide range of children and youth with medical, developmental, and behavioral conditions.
METHODSEthical approval for this research was obtained from the University of British Columbia Children's and Women's Research Ethics Board (H21-00078).
Recruitment and EligibilityFamilies were recruited from clinics that serve patients with autism, cerebral palsy, and complex pain at a tertiary care pediatric hospital in Western Canada. Patient lists were reviewed by clinicians for families that met eligibility criteria: (1) youth aged 12 to 18 years and (2) youth and/or family members with sufficient English language skills to participate in the interview. We asked clinicians to purposively identify families who might represent a range of diverse identities, social positions, and experiences to ensure that our findings would be captured a broad spectrum of families. Identified families (n = 35) were first contacted by a clinical research coordinator to obtain consent to be contacted for research purposes. Willing families (n = 27) were contacted by a research assistant who obtained informed consent/assent. Families were scheduled for an interview; a total of 19 families participated.
Severe Neurologic Impairment SubstudyTo purposively recruit families with diverse accessibility needs, we recruited a subsample of families of children with a severe neurologic impairment. Severe neurologic impairment is an umbrella term for “disorders of the central nervous system that arise in childhood, resulting in motor impairment, cognitive impairment, and medical complexity, for which much assistance is required with activities of daily living.”17
Given the lower prevalence of these conditions, and the additional burden that care needs place on families, broader eligibility criteria were applied: families could have a child aged 6 months to 18 years and live anywhere in Canada. Recruitment materials were reviewed by a collaborator with lived experience, who also assisted in disseminating these materials within their networks. The study was advertised on social media and to past participants of our research team. Interested families contacted the research team, informed consent was obtained, and 5 families completed the interview.
Family InterviewsInterviews were conducted using Zoom. The interviewer, a White, cisgender female, clinical psychologist/postdoctoral research fellow, did not have any prior relationships with participating families. Most parent-child dyads participated in the interview together; 2 youth participated without parents present, and 6 parents participated without their children (who were primarily nonverbal). Youth who participated without parents present were of sufficient age and capacity to consent for their own participation, and their parents were aware and consented to their child's participation in the study. Interviews lasted 25 to 83 minutes and occurred from April 2021 to May 2022. All interviews began with the researcher providing an overview of the Living Lab at Home, followed by demographic questions. Then, families were asked about their perceptions of the Living Lab at Home, feasibility, barriers/facilitators, concerns, compensation, and research priorities (semistructured interview guide in Supplemental Digital Content 1, Supplemental Materials, https://links.lww.com/JDBP/A416). Feedback was elicited about 3 specific examples of home-based methods: smartphone-based Ecological Momentary Assessment, accelerometer, and salivary cortisol. Families were provided descriptions of each of these methods and what they would entail, tailored based on family understanding and the level of familiarity with research methods/the technology being discussed. The researcher aimed to provide descriptions that were sufficiently detailed that families would understand the concept but vague enough to elicit feedback about alternative ways of collecting data that may be more feasible for the family. Although we did not show pictures or samples during the interviews, the interviewer occasionally used examples of devices participants were familiar with, such as Fitbit, to orient them if needed.
An adapted version of the questions was used for the families of children with a severe neurologic impairment, based on feedback from a collaborator with lived experience. The interviewer provided reflection, clarification, and follow-up questions and solicited feedback in a balanced manner from both members of the family (if present) throughout the interview, in a flexible way depending on the family's needs and comfort. Occasionally, other family members or caregivers who were present during the interview would offer input; this was recorded and transcribed for the purposes of continuity/context. Many families also referenced other children in their family who had developmental, medical, or psychiatric conditions when providing their responses. All families were compensated with a $40 gift card.
Data AnalysisInterviews were recorded, transcribed, and transcriptions checked by the interviewer. Two analytic approaches were used: For questions that generated a response that could be quantified (e.g., How many times a day would it be reasonable to ask you to fill out questions?), responses were summarized descriptively. For the remainder, transcripts were analyzed using reflexive thematic analysis, broadly following the conventions of Braun and Clarke,18 to understand the general sentiment, perceptions, concerns, and ideas raised by the participants. Thematic analysis was selected as a method to capture diverse experiences of families with varying developmental and medical backgrounds, rather than searching for a single narrative that encompasses the variety of experiences faced by families. The researchers took an inductive (data-driven) approach to analysis, with a constructivist epistemological position based on the assumption that the themes are coconstructed between the researchers and participants, thus necessitating a reflexive approach. As such, the research team did not attempt to achieve saturation.19
Data analysis was led by the primary interviewer, supported by a coinvestigator with expertise in pediatric occupational therapy and qualitative research and a medical student. All data from the interviews, including from interviews of the parent alone, youth alone, or parent and child together, were included in a single analysis. Analysis included familiarization with the data, inductive generation of codes, collecting similar codes into themes, and then revisiting the overall data to understand and name the themes in relation to the overall narrative of the transcripts. Themes and the process of analysis were reviewed with the study's senior investigator (a developmental pediatrician). This collaborative approach to analysis was used to enrich the understanding of the data from a variety of perspectives and backgrounds, not necessarily to achieve consensus.18 The first 2 themes were generated through the analysis of interviews from the broader study. These themes were refined as analysis was completed with the severe neurologic impairment substudy (when the third theme was added), and throughout manuscript writing; a process that allowed for further reflection.18
Trustworthiness was established through reflexive practice (summarized below), records of the process of data analysis (summarized above), provision of thick description of findings with corresponding verbatim quotes from participating families, and triangulation of findings by investigators with diverse training and experience backgrounds. The interviewer kept field notes and engaged in reading and self-reflection related to the perspectives she brought to the interviews and analysis. The research team's perspectives were that the Living Lab at Home would have great potential to advance research and increase accessibility for underrepresented populations. In addition, as clinician scientists, the research team had direct experience of the frustrations of not seeing the patient populations they serve represented in research and a focus on ensuring clinical relevance of this research.
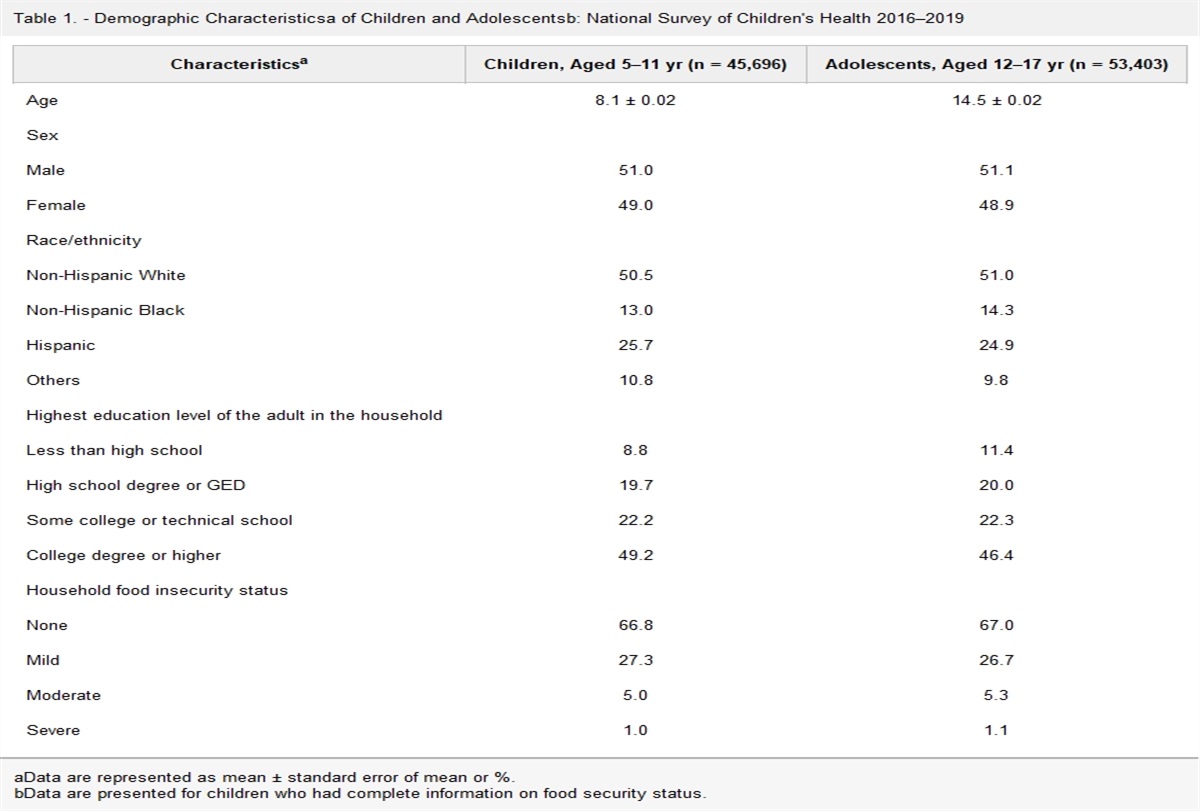
RESULTS Descriptive Statistics of Quantifiable ResponsesTable 1 presents the demographic information of families who took part. Three-quarters of participants expressed an interest in taking part in a Living Lab at Home study; the remaining participants stated that it would depend on the topic and/or requirements of the specific study (Table 2). Some participants indicated that they would not want to take part in the accelerometer (21%) or saliva (17%) data collection, primarily citing concerns related to privacy (e.g., data security with respect to location tracking or biological samples) and comfort/convenience (e.g., lacking space to refrigerate saliva collection and not liking the look or feel of wearing an accelerometer). A median response of 2 weeks of data collection was reported to be feasible, and most preferred that this be a consecutive period of data collection with no break. Most participants indicated that responding to smartphone questionnaires 2 to 3 times a day would be acceptable, and nearly all (88%) wanted access to their study data in some form.
Table 1. - Demographic Information of Participating Families (N = 24) M ± SD or n (%) Child demographics Femalea 13 (54%) Child age in yrb Broader group (n = 19; range 12–19 yr) 15.26 ± 1.76 Severe neurologic impairment subgroup (n = 5; range 3–15 yr) 8.80 ± 5.54 Child ethnicityc,d Asian origins 8 (33%) European origins 19 (79%) North American Aboriginal origins 3 (13%) Oceania origins 1 (4%) Child diagnosesd,e Autism spectrum disorder 7 (29%) Cancer 2 (8%) Cerebral palsy 5 (21%) Chronic pain 11 (46%) Neurodevelopmental conditions (e.g., ADHD, ID, and LD) 8 (33%) Neurologic conditions (e.g., epilepsy, brain injury, and congenital conditions) 6 (25%) Psychiatric conditions (e.g., anxiety, depression, OCD, and PTSD) 9 (38%) Rare genetic/metabolic disorderf 5 (21%) Parent demographics Femalea 18 (75%) Parent age (yr) 45.45 ± 5.08 Parent ethnicityc,d Asian origins 5 (21%) European origins 17 (71%) North American Aboriginal origins 2 (8%) Oceania origins 1 (4%) Language spoken at homed English 23 (96%) Others 6 (25%)Includes demographic information about children/youth who were not present during the interview because they were unable to communicate verbally but for whom the parent provided information on behalf of their family.
aParticipants were asked to self-report their sex for the interviews of the broader group. However, based on participant feedback, this was changed to “gender” for the severe neurologic impairment substudy interviews. As such, the table combines both. No participant reported a sex or gender other than male/boy or female/girl.
bThis table combines demographics for all groups involved in the study; however, it should be noted that the eligible age range for families in the broader study was 12 to 18 years, whereas the severe neurologic impairment substudy was open to families of children 6 months to 18 years. As such, the age ranges are reported separately. Range includes 1 adolescent who was 19 years at the time of participating in the interview but who was in the appropriate age group for eligibility for this study when recruitment began.
cSelf-reported through an open-ended question and then categorized based on Statistics Canada categories. Individuals who reported “Caucasian” or “White” were categorized as European.
dAdds up to >100% as participants could select more than 1 option.
eDiagnoses were self-reported by families in an open-ended question and coded into categories by researchers.
fSpecific diagnoses not reported to protect family privacy. Disorders included presentations such as visual impairments, feeding difficulties (requiring tube feeds), developmental delay and communication challenges, issues related to tone and spasticity, and neurodegeneration.
ADHD, attention-deficit/hyperactivity disorder; ID, intellectual disability; LD, learning disability; OCD, obsessive-compulsive disorder; PTSD, posttraumatic stress disorder.
aResponse provided for the entire family, as not all members of the dyad answered all questions. In the case in which the parent and youth disagreed on their response, it was coded as “Mixed.”
bOne family responded, “it depends.” No family suggested more than 3 times a day or less than once.
cThis category represents some families wanting to see their own data, some wanting a summary of data across all participants, and some wanting both to be able to compare themselves with other families.
Reflexive thematic analysis was used to describe 3 primary themes: the importance of flexible adaptations to allow for incorporation of research into families' daily lives (flexibility and customization), perceived benefits of a reciprocal relationship between families and the research team (reciprocity), and barriers to research participation that would be addressed by these methods (opportunity and accessibility). Actionable feedback was used to generate a series of recommendations for future projects using the Living Lab at Home platform (Table 3).
Table 3. - Recommendations for Revisions to the Living Lab at Home Platform Based on Feedback From Initial Interviews Feedback Recommendation Flexibility and customization The need for flexible timing Have the option for participants to select what time of the day to complete data collection and provide a large window of time during which to complete itFamilies described a need for adaptations specific to the condition they were managing, such as flexible options for the position of an accelerometer to account for medical equipment (e.g., wheelchair and G-tube) or smaller body size. Families of youth with conditions that affect motor function described potential challenges of acquiring a saliva sample or answering self-report questions independently. They also expressed concern about the child damaging the accelerometer or injuring themselves with it. Families with a severe neurologic impairment and/or autism cited sensory issues as a potential barrier:
“If you're going to provide a wearable, in my opinion, this might be a bit much, but like, I think there should be a silicon type of strap as well as a metal one (…) and maybe a fabric option as well for those that like a soft microfiber.”—Youth #13
The importance of flexibility in timing (when and how long) was emphasized by nearly every family taking part in this study. Families of children with medical complexity also drew attention to the need to pause data collection in cases of a major medical event or hospitalization. Furthermore, they emphasized the importance of flexibly including multiple respondents in data collection, with siblings mentioned by many families as playing an important role in the child's life. Data collection also offered the opportunity for siblings to feel included:
“Maybe just a little bit about like, more of the family… like who else is involved besides, just the person. Just because you asked about me and [child], but like he does have a younger brother and a dad that is very important and does a lot of stuff.”—Parent of a child with a severe neurologic impairment #1
Some families referenced the possibility of study tasks serving as a regular reminder of ongoing challenges, necessitating a trauma-informed approach:
“I guess, just like in general, procrastinating and not wanting to do it because then it reminds you of all the [expletive] you're dealing with. I don't know, like, that's a big one for me. I like to bury it away (…) So I don't think I'd necessarily want to do that every day and bring it up 3 times a day.”—Youth #15
Taken together, these findings highlight the need for a flexible and individualized approach to data collection.
Theme 2: ReciprocityA central tenant of ethical patient-oriented research is a reciprocal relationship between researcher and participant, rather than participants being a “means to an end” from whom researchers collect data. In keeping with this theme, the importance of participant involvement in research development and potential benefits for both researchers and participants in projects using the Living Lab at Home platform were identified during the interview process.
Most youth and families expressed interest in receiving a report of their own data and/or the cumulative data from the study, some citing past experiences of taking part in research and having their data go “off into the void.” Tracking and visualizing data collected longitudinally has the potential to help youth interpret trends and relationships between their symptoms and experiences:
“(…) maybe it'll help us understand ourselves a little better.”—Youth #12
For many children with communication challenges, parents become skilled at interpreting their child's moods and behaviors. Still, using the data collected, particularly data on invisible phenomena (e.g., salivary cortisol and accelerometer sleep data) may help parents gain a better understanding of their child:
“Especially with having a child who's nonverbal. It's a whole other can of worms here. Because it can be a whole bunch of other stuff we find out about her and about things going on inside her body from data collected.”—Parent of a child with a severe neurologic impairment #4
Some families discussed data visualization increasing their accountability in engaging in health-related behaviors or tracking the efficacy of interventions. For other families, their data would aid in the identification of palliative care goals and increase their child's comfort:
“Well some people might be really interested in looking at charts and graphs and knowing. But I know that our graph looks like this [downward motion]. And we're just, our goal is to keep [child's name] comfortable. So anything that would feed back to support that goal. Otherwise, it's your data.”—Parent of a child with a severe neurologic impairment #2
Data summaries and reports were seen as useful in communicating symptom trends not only to families but also to health care providers. Many families wanted data to support their own account of their illness, aid their memory, and supplement information already being collected by those involved in their care:
“(…) because if you're getting statistics from this like back from what's going on, you could bring that to a doctor, you can say, I've been a part of this research group, this is what we've been monitoring. And what can we do with this? So, I know for me, I think that would have been a lot more helpful, having proof that something's wrong.”—Youth #9
One parent saw the distribution of data back to families and, therefore, lack of children's confidentiality as a potential barrier to accurate data collection:
“You know sometimes kids want to give answers to people, but are afraid of what their parents might see if they answer honestly, and if the parent has access to the child's information.”—Parent #9
Families were mixed as to whether they would like to see their own data in tandem with overall study results. This method of data presentation may promote not only a sense of belonging in affected youth but also potential feelings of otherness:
“I think that it could also offer reassurance to a teen to let them know that they are similar to others. I think it could be a trigger, it could be disheartening, to see if you are an outlier with a negative finding so I think that that should be treated with some caution.”—Parent #4
A common motivator for research participation was the altruistic goal of being part of a research process that helps others in a similar position. For many, this was incentive enough to overcome burdens imposed by data collection:
“That would be our goal. That the research helps somebody. Promise me that? And we're in.”—Parent of a child with a severe neurologic impairment #2
Theme 3: Opportunity and AccessibilityParticipants saw the potential for in-home data collection methods to increase opportunities for families who might not otherwise be able to take part in research because of geographic location, finances, mental health, or logistical challenges:
“(…) there's not any entities doing this kind of research here in [Northern Canada], where we live (…) for us, any research, unless it's home-based, would involve travelling.”—Parent of a child with a severe neurologic impairment #4
In addition, travel to hospitals and research centers would impose potential confounds on the data collected. Allowing youth to remain in a comfortable environment was suggested to lead to more ecologically valid data:
“Maybe you'll get better, or more realistic data, than you would if you would if you have somebody sitting in an office, in a hospital, or at a research lab, because that in itself, it is an unusual environment, and it could sort of affect how people respond.”—Parent #13
For parents of children with a severe neurologic impairment, the lack of data collection methods appropriate for their children was described as a barrier to participation and their ability to benefit from research findings, which could be solved by adapted in-home data collection:
“I've never really paid attention to the research studies because um… because of the lack of, like, accessibility to us, for us”—Parent of a child with a severe neurologic impairment #1
DISCUSSIONThe voices of children/youth with diverse developmental capabilities and their families have not traditionally been incorporated into the design and validation of in-home methods of data collection, despite the tremendous potential these approaches have to enhance child health research and care. Ours is the first study to describe 3 themes inherent to their participation in a living laboratory to study everyday experiences for children and families whose health conditions cross the developmental spectrum. Flexibility and customization captured that home-based data collection occurs in the context of existing activities and responsibilities and encourages the adaptation of methodologies to meet the specific needs of the child. Although flexibility might require some leeway with respect to scientific rigor, the trade-off is likely to be favorable in benefit of ecological validity, retention of families in studies, and meaningful data collection. Further research is needed to determine how to implement these suggestions while still collecting usable, valid data, although research examining the use of smartphone-collected parental reports of behavior in children with autism suggested that data collection may be abbreviated without compromising study integrity.20 Involvement of multiple caregivers/family members was also cited as key, mirroring recent work by Phoenix et al.,21 advocating for the representation of diverse family structures in research, and recognizing that caregiving roles can be uniquely dispersed in the context of supporting children with disabilities.
Reciprocity describes the mutual benefit to both researchers and participants that results from effective community-based research. This aligns with the rapidly growing literature on the benefits of patient engagement at all stages of the child health research enterprise,22 and that families want to engage with researchers in this way.23 Although researchers benefit from the unique insights of families in the codevelopment of more acceptable methods, families also identified many potential benefits to participants. A common sentiment expressed by families was the desire to use their data to better understand themselves, their child, and their condition. Although returning general lay summaries of research findings to participants is increasingly common practice and desired by participants,24 providing individual research findings is considered controversial, and the majority of the existing published pediatric literature on the topic has focused on the ethics of this practice.25,26 This is of particular importance for research with clinical implications and is an area that deserves consideration of the ethics, practicalities, and family preferences in how this reciprocity is constructed,27 as well as investigating whether access to one's own data may have therapeutic potential.28
Opportunity and accessibility illustrates family perceptions of existing barriers to research participation and how this can be addressed by home-based research. Unequal access to research opportunities has been described as both a legal and ethical issue.29 Despite research showing that communities with disabilities are keen to engage in research,30 many studies either directly exclude these groups or engage in indirect exclusion by lacking accessible methods, thus contributing to disparities in health research and care. Families recognized adapted in-home methods as having the potential to increase accessibility to research for those with developmental and medical needs and in rural and remote communities. This offers the opportunity to contribute to research and benefit from advancing research in areas in which their children are not typically represented, focusing on topics of importance to them (e.g., pain management/improving comfort, mental health, and sleep). Nevertheless, remote participation has drawbacks, and some families expressed a desire to incorporate occasional in-person visits. This theme demonstrates the value of eliciting patient engagement at the early stages of project development so that specific barriers can be identified and addressed. Importantly, family suggestions regarding adaptations to address their needs were generally straightforward and low cost to implement.
Beyond the 3 themes, concerns about the feasibility and adverse events in home-based longitudinal developmental research were also raised. Interestingly, the modality of data collection that may have been perceived as lowest barrier (accelerometer; as it does not require any active engagement to collect data) raised concerns about the privacy and confidentiality of data, as well as the comfort of the wearable device and possibility of damaging the device. Research participation that prompts families to think about their challenges may add to the emotional burden of managing an illness. Such adverse events may serve to systematically exclude certain families, particularly those who have experienced traumatic medical experiences. Although families identified positive aspects to accessing their own data (i.e., tracking progress/interventions and motivating behavior change), concerns were also raised about the possibility of iatrogenic harm.
In-home approaches to longitudinal, real-world data collection methods are increasingly used to obtain in-depth assessment of clinical phenomena. Integration of multiple modalities is increasingly common,31,32 as are smartphone applications that can both actively and passively collect multiple modalities of data (e.g., self-report, physical activity, screentime, light exposure, and social connections through telephone calls).33 Studies cite compliance and lack of diversity as challenges requiring further research. Our hope is that the present findings will assist in developing patient-centered approaches to reduce burden for families, increase the quality and completeness of the collected data, and contribute to the meaningful integration of research with clinical care.34 This is particularly important for families whose children have medical and developmental complexity, in which there are documented inequities in unmet health care needs.35
LIMITATIONSThis study focused on the views of families whose children's function is represented across the developmental spectrum, addressing equity and accessibility across diverse research settings. However, as data were not collected regarding socioeconomic status or geographic location, we cannot speak to how representative our sample is from this important equity-related perspective; this information is now being collected as part of our ongoing Living Lab at Home development. In addition, although we did not engage in member checking specific to this project (i.e., returning results to study participants for their input on how accurately the findings and interpretation represent their experiences), the information obtained in these interviews has been incorporated into a pilot demonstration project (paper forthcoming) describing family experiences with in-home research modalities that incorporate the feedback described herein. This will allow us both to check whether our interpretation of their data reflects families' experiences and to see whether the implementation of their data in practice addresses the concerns they raised. Future research may incorporate interaction with the data collection tools being discussed (particularly for complex or novel technology that families might not be familiar with) in real time during the interview to elicit feedback, for example, using think-aloud protocols.
CONCLUSIONSThis study sought to elicit views of families and their children across the developmental spectrum about longitudinal home-based data collection methods suitable for use in pediatric research. Families saw value in in-home data collection and provided creative and feasible solutions to mitigating challenges. Consideration should be given into how to embed family feedback within the development of larger platforms of data collection, beyond just for individual projects, and how to provide integration of this research-oriented data collection with clinical care.36
ACKNOWLEDGMENTSThe authors thank Ursula Brain, Jane Shen, Anne-Mette Hermansen, Laesa Kim, and their clinician colleagues for their contributions to recruitment, data collection, and transcription. The authors also thank the families, researchers, and clinicians who shared their time and thoughts as part of the present project.
REFERENCES 1. Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annu Rev Clin Psychol. 2008;4:1–32. 2. Condon EM. Psychosocial influences on acceptability and feasibility of salivary cortisol collection from community samples of children. Res Nurs Health. 2016;39:449–462. 3. Berger AM, Wielgus KK, Young-McCaughan S, et al. Methodological challenges when using actigraphy in research. J Pain Symptom Manage. 2008;36:191–199. 4. Psihogios AM, Lane-Fall MB, Graham AK. Adolescents are still waiting on a digital health revolution: accelerating research-to-practice translation through design for implementation. JAMA Pediatr. 2022;176:545–546. 5. Kovac M, Mosner M, Miller S, et al. Experience sampling of positive affect in adolescents with autism: feasibility and preliminary findings. Res Autism Spectr Disord. 2016;29-30:57–65. 6. Dallman AR, Bailliard A, Harrop C. Identifying predictors of momentary negative affect and depression severity in adolescents with autism: an exploratory ecological momentary assessment study. J Autism Dev Disord. 2022;52:291–303. 7. Chen YW, Cordier R, Brown N. A preliminary study on the reliability and validity of using experience sampling method in children with autism spectrum disorders. Develop Neurorehabil. 2015;18:383–389. 8. Barton HJ, Coller RJ, Loganathar S, et al. Medical device workarounds in providing care for children with medical complexity in the home. Pediatrics. 2021;147:e2020019513. 9. Kramer-Roy D. Using participatory and creative methods to facilitate emancipatory research with people facing multiple disadvantage: a role for health and care professionals. Disabil Soc. 2015;30:1207–1224. 10. Bradbury-Jones C, Isham L, Taylor J. The complexities and contradictions in participatory research with vulnerable children and young people: a qualitative systematic review. Soc Sci Med. 2018;215:80–91. 11. Hossain M, Leminen S, Westerlund M. A systematic review of living lab literature. J Clean Prod. 2019;213:976–988. 12. Ståhlbröst A, Holst M. The Living Lab Methodology Handbook. Luleå, Sweden: Plan Sju kommunikation AB; 2012. Available at: www.ltu.se/cdt. Accessed July 31, 2022 13. Archibald MM, Wittmeier K, Gale M, et al. Living labs for patient engagement and knowledge exchange: an exploratory sequential mixed methods study to develop a living lab in paediatric rehabilitation. BMJ Open. 2021;11:e041530. 14. Phoenix M, Nguyen T, Gentles SJ, et al. Using qualitative research perspectives to inform patient engagement in research. Res Involv Engagem. 2018;4:20. 15. Doria N, Condran B, Boulos L, et al. Sharpening the focus: differentiating between focus groups for patient engagement vs. qualitative research. Res Involv Engagem. 2018;4:19. 16. Manalili K, Siad FM, Antonio M, et al. Codesigning person-centred quality indicators with diverse communities: a qualitative patient engagement study. Health Expect. 2022;25:2188–2202. 17. Allen J, Brenner M, Hauer J, et al. Severe Neurological Impairment: a Delphi consensus-based definition. Eur J Paediatric Neurol. 2020;29:81–86. 18. Clarke V, Braun V. Thematic Analysis: A Practical Guide. Thousand Oaks, CA: Sage; 2021. 19. Braun V, Clarke V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual Res Sport Exerc Health. 2019;13:201–216. 20. Jones RM, Tarpey T, Hamo A, et al. Smartphone measures of day-to-day behavior changes in children with autism. npj Digital Med. 2018;11:34. 21. Phoenix M, Reitzel M, Martens R, et al. Reconceptualizing the family to improve inclusion in childhood disability research and practice. Front Rehabil Sci. 2021;2:710580. 22. Woodgate RL, Zurba M, Tennent P. Advancing patient engagement: youth and family participation in health research communities of practice. Res Involv Engagem. 2018;4:9–6. 23. Smith J, Pike I, Brussoni M, et al. Mixed methods study exploring parent engagement in child health research in British Columbia. BMJ Open. 2019;9:e025404. 24. Shalowitz DI, Miller FG. Communicating the results of clinical research to participants: attitudes, practices, and future directions. Plos Med. 2008;5:e91. 25. Vanaken GJ, Noens I, Roeyers H, et al. Ethics of returning children's individual research findings: from principles to practice. Eur Child Adolesc Psychiatry. 2021;30:1163–1171. 26. Lefaivre MJ, Chambers CT, Fernandez CV. Offering parents individualized feedback on the results of psychological testing conducted for research purposes with children: ethical issues and recommendations. J Clin Child Adolesc Psychol. 2010;36:242–252. 27. Deluzio TDB. How Do Individuals with Cerebral Palsy and Their Families Prefer How Do Individuals with Cerebral Palsy and Their Families Prefer to Receive and Use Evidence-Based Information to Individualize to Receive and Use Evidence-Based Information to Individualize Services to Optimize Outcomes? Services to Optimize Outcomes? Ontario, Canada: The University of Western Ontario; 2017. Available at: https://ir.lib.uwo.ca/etd/4627. Accessed September 28, 2022. 28. Boerner KE, Desai U, MacLean KE, et al. Data visualization as an intervention for pediatric c
留言 (0)