
記住我

In accordance with the tenets of the Declaration of Helsinki, the Ethics Committee of the Affiliated Eye Hospital of Nanchang University Review Board (Jiangxi, China) approved the study protocol (KJ2008-10). All patients fully understood the treatment and provided written informed consent before study participation.
In this prospective, comparative study, 23 eyes of 18 patients with hyperopia at the Affiliated Eye Hospital of Nanchang University, China were recruited. The patients had no ocular diseases other than refractive error and met the following inclusion criteria: presence of hyperopia in ≥ 1 eye, age > 18 years, and a strong willingness to correct hyperopia. All patients underwent a systematic preoperative ophthalmologic examination, including slit-lamp examination, measurement of UDVA, corrected distance visual acuity (CDVA), intraocular pressure, and Pentacam high resolution (HR) imaging.
Eyes were randomly categorized into two groups—SMI-LIKE group (11 eyes of 9 patients) and FS-LIKE group (12 eyes of 9 patients). In the SMI-LIKE group, allogenic lenticules extracted from myopia SMILE were implanted into a femtosecond laser made pocket. While in the FS-LIKE group, allogenic lenticules were positioned under a femtosecond laser flap. Posterior corneal elevation was measured using the Pentacam over a three-month follow-up period.
Surgical techniquesThe same experienced surgeon performed all procedures (SL). The VisuMax femtosecond laser system (Carl Zeiss Meditec AG, Germany) with a repetition rate of 500 kHz and pulse energy of 130 nJ was used to perform all surgeries. Track distance and spot distance was set at (i) 4.5 µm in the lenticule and cap and (ii) 2.0 µm in the lenticule side and cap side.
Before surgery, donor patients underwent a comprehensive blood test, including blood routine examination, liver and renal function tests, and screening for infectious diseases (human immunodeficiency virus, hepatitis B virus, hepatitis C virus and syphilis). SMILE procedures were performed on donors using the myopia treatment mode. The femtosecond laser settings were as follows: 120 µm intended cap thickness, 6.5–6.8 mm optical zone (lenticule diameter), 7.5 mm cap diameter; and a 2 mm side cut at 120°. The lenticule was manually extracted and prepared with caution for re-implantation. To avoid flipping the lenticule orientation, we marked the anterior surface of the lenticule at the incision position with a marker.
Lenticule implantation surgery was scheduled on the same day as the donor eye procedure. The diopter of the implanted lenticule was determined according to the spherical error of the subjective refraction of the recipient with an opposite sign. In the SMI-LIKE group, the stromal pocket was created using a flap license. The intended cap thickness was set at 100 µm and the diameter was 7.9 mm. A hinge length of 330° was used, thereby providing a 30° superior incision for lenticule implantation. Once laser scanning was completed, the surgeon inserted a spatula into the cornea and dissected the pocket plane. The extracted lenticule was then inserted into the pocket. In the FS-LIKE group, a flap of 100 µm and diameter of 7.9 mm was created instead of the cap. The hinge was located at 90°, with a length of 50°. After lifting the flap, the fresh donor lenticule was transferred directly onto the exposed stromal bed. The flap was replaced, and a bandage contact lens was placed over the cornea after surgery. For all surgeries, centration was accepted when the lenticular margin was concentric with the margin of the pocket or stromal bed. Representative images of SMI-LIKE and FS-LIKE are shown in Fig. 1.
Fig. 1
Corneal images of SMI-LIKE and FS-LIKE. a Anterior optical coherence tomography image of SMI-LIKE. b Anterior optical coherence tomography image of FS-LIKE. SMI-LIKE, small-incision lenticule intrastromal keratoplasty; FS-LIKE, femtosecond laser-assisted lenticule intrastromal keratoplasty
Postoperative topical medication regimens were identical for each eye and consisted of 0.5% levofloxacin four times per day for seven days and prednisolone acetate ophthalmic suspension was applied topically four times daily for seven days. After the first week, the medication was changed to topical 0.1% fluorometholone four times daily for one month, and subsequently the application frequency was decreased to once a day for another month. The contact lens in the FS-LIKE group was removed one day postoperatively.
Postoperative examinationFollow-up appointments were scheduled 1 day, 1 month, and 3 months after surgery. Postoperative examinations included Pentacam imaging examinations, slit-lamp examination, UDVA and CDVA measurement, spherical equivalent (SE) refraction, and intraocular pressure.
Pentacam Scheimpflug imagingAll eyes were examined using the Pentacam imaging system (Oculus GmbH, Wetzlar, Germany). After attaining patient alignment, the device captured 25 images and automatically recorded 12,500 elevation points within 2 s. To avoid miscalculations of poor imaging, the quality of each measurement was shown in the specification window, and only results with “OK” statements were accepted. The examination was duplicated if the statement did not meet the requirements (marked as yellow or red). Only maps with at least 10 mm of corneal coverage and no deduced data in the central 9 mm zone were accepted.
Data collectionMean keratometry of the posterior corneal surface (Kmb) and elevation data were extracted directly from the Pentacam image. The reference best-fit sphere (BFS) was defined in the central 8.0 mm region of the preoperative data to be equal across images. For points above the reference, the values were positive; for points below, the values were negative. The calculated value of a single point was the posterior central elevation (PCE) above the BFS. The other 26 determined points in the central 6 mm zone were obtained as follows: 4 points at a distance of 1 mm from the center along the 45°, 135°, 225°, and 315° meridians (0° was defined as the horizontal semi-meridian on the right, and rotating counterclockwise in both eyes), 8 points at a 2 mm distance from the center at 0°, 45°, 90°, 135°, 180°, 225°, 270°, 315°, and 14 points at a distance of 3 mm from the center along 15°, 45°, 75°, 90°, 105°, 135°, 165°, 195°, 225°, 255°, 270°, 285°, 315°, and 345°. The posterior corneal elevation in the central 4 mm area (PCE-4 mm) and in various concentric circles (2 mm diameter, posterior mean elevation (PME)-2 mm; 4 mm diameter, PME-4 mm; 6 mm diameter, PME-6 mm) was calculated as the mean value from points in the corresponding area. Graphs of all the calculated values are displayed in Fig. 2. Changes in elevation were determined by subtracting the preoperative data from postoperative data (difference elevation map). The change in elevation was due to a shift in the posterior corneal surface. All data were recorded in an Excel spreadsheet (Microsoft Corp., Redmond, WA, USA) for further analysis.
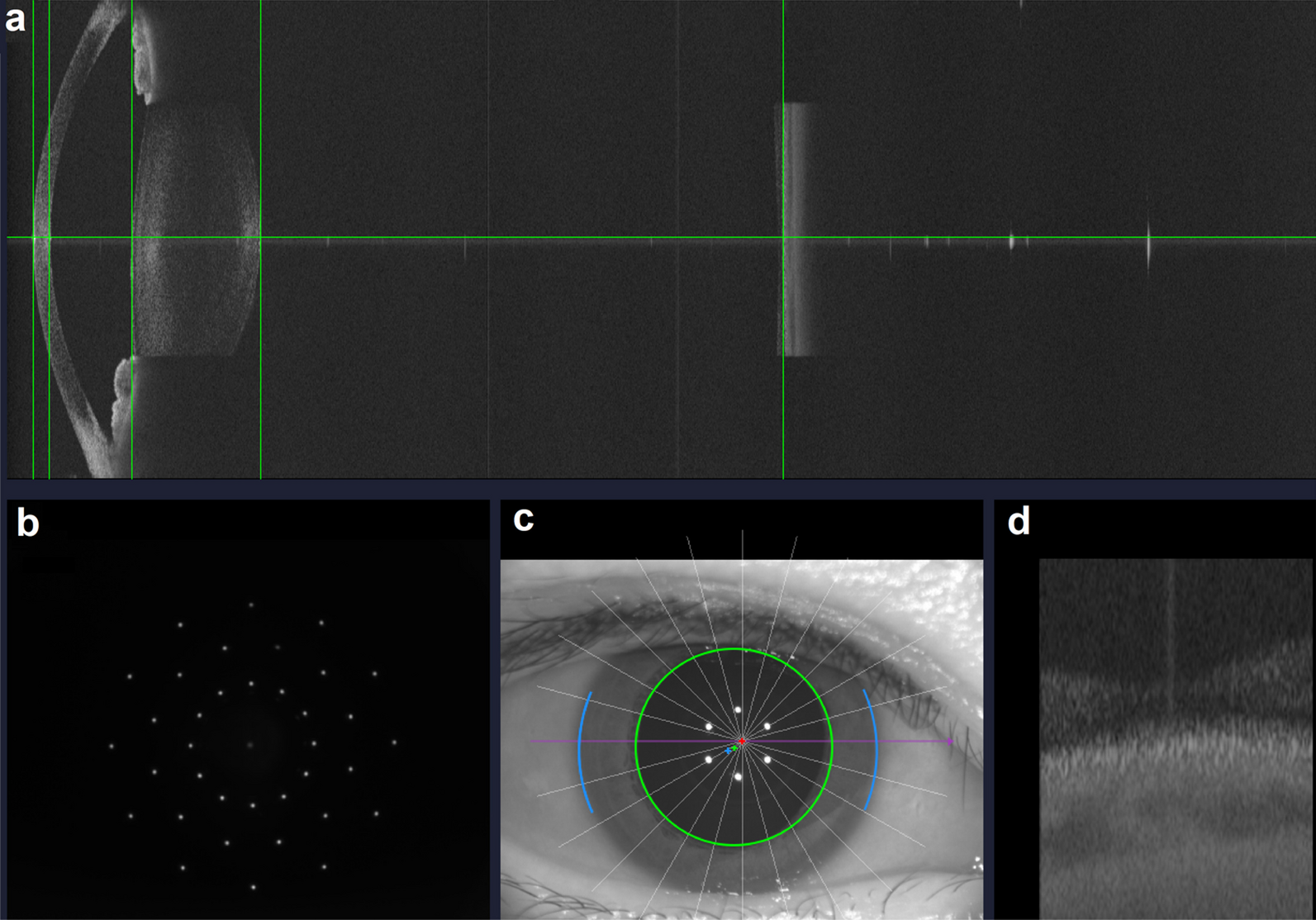
Fig. 2
Overview of all the calculated values in Pentacam. Posterior central elevation (PCE, black dot); Mean value from 4 points in 2-mm diameter (PME-2 mm, yellow dot); Mean value from 8 points in 4-mm diameter (PME-4 mm, red dot); Mean value from 14 points in 6-mm diameter (PME-6 mm, green dot); Mean value from 13 points in the central 4-mm area (PCE-4 mm, black dot, yellow dot and red dot). PME, posterior mean elevation
Statistical analysisDescriptive results are presented as mean and standard deviation. The Shapiro-Wilk normality test and test for homogeneity of variances were performed for all data. Two-way analysis of variance for repeated measures with Bonferroni correction was employed to compare pre- and postoperative values. Pearson’s Chi-squared test or the Kruskal-Wallis test was used to compare differences between groups. A bivariate normal analysis was performed prior to the correlation test. Pearson’s or Spearman’s correlation tests were used to determine the association between changes in posterior corneal elevation and lenticule thickness. A stepwise multiple linear regression model was performed to explore possible factors affecting posterior corneal elevation changes, such as lenticule thickness, lenticule refractive power, preoperative corneal characteristics (corneal thickness, Q value, K value in anterior corneal surface and posterior corneal surface, total corneal refractive power). Statistical analyses were performed using SPSS (version 20.0; SPSS Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05.
留言 (0)