Previous clinical and in vitro studies have analyzed the visual, optical, and functional quality of life outcomes obtained with different commercially available EDOF IOLs [4,5,6]. They put forward that these lenses can improve intermediate vision while providing a good level of far vision. However, there is a wide variety of EDOF lenses with different optical designs and their resulting impact on the patient’s visual performance can vary significantly. Previous studies have reported on the outcomes achieved with AcrySof IQ Vivity non-toric [2, 3] and toric [4,5,6,7,8] models. However, to the best of our knowledge, no clinical studies have published any results for the toric model implanted in eyes with low corneal astigmatism. Therefore, the present study aimed to fill this gap.
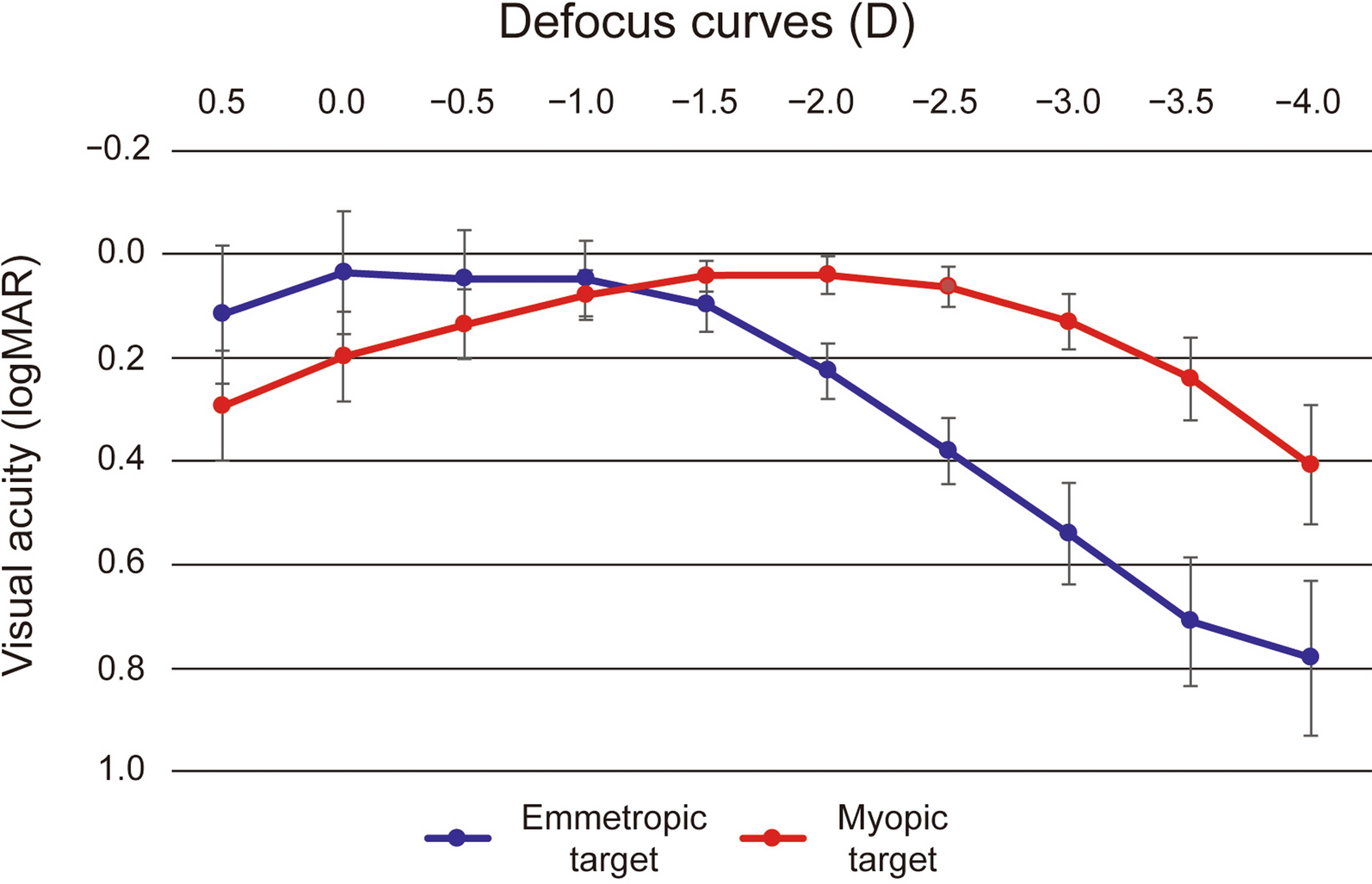
Our results revealed that the lens offers excellent refractive accuracy in both spherical and astigmatism correction (SE and refractive astigmatism were both less than one quarter of a diopter: − 0.10 ± 0.17 D and − 0.16 ± 0.24 D, respectively). This is also supported by the concentration of dots for postoperative refractive astigmatism around the origin in Fig. 2 (mean absolute of 0.18 ± 0.26 D). Our results show that the lens provides an extended range of vision, as evidenced by the monocular defocus curve in Fig. 4, with a peak in visual acuity for distance vision (vergence of 0.00 D) and a continuous reduction for intermediate and near vision (down to − 3.00 D). This gave a depth-of-focus of approximately 1.75 D. We believe better results can be expected if a binocular assessment is performed. The CDVA was ≥ 20/25 in 95.74% of eyes and ≥ 20/32 in 97.87%, and we found a DCIVA ≥ 20/32 in 85.11% and ≥ 20/40 in 74.47% of eyes. We also assessed the rotational stability of the lens as it is important for any platform aiming to correct astigmatism. The rotation was less than 5 degrees in all eyes and the mean absolute rotation was 0.74 ± 1.13 degrees. According to ISO11979-7:2024, the absolute value of rotation should be less than 10 degrees in 90% of implanted eyes [18]. However, we consider this amount of rotation to be clinically insignificant and, based on our values, we conclude that the lens had a high degree of rotational stability when implanted in the capsular bag. This stability correlates with effective postoperative astigmatism correction (mean refractive cylinder of − 0.18 ± 0.26 D) and hence good unaided distance visual acuity (85.11% of patients had a monocular UDVA of 20/25 or better, Fig. 3a). The rotational stability of the AcrySof IQ toric IOL, the platform used for the Vivity IOL, has been reported in previous studies with mean absolute rotations ranging from 2.20 ± 2.20 to 4.24 ± 4.10 degrees and with at least 88% of lens rotating less than 10 degrees [19,20,21]. An undesired rotation of a toric IOL by 5 degrees translates into a theoretical loss of approximately 17% of the astigmatic effect [22, 23]. This corresponds to 0.17 D of lost astigmatism correction for a T2 model although the baseline residual astigmatism and lost astigmatism correction do not generally share a common axis and do not add linearly [7]. Our results also show that the AcrySof IQ Vivity IOL confers good vision without eyeglasses (see the high percentage of patients reporting “good” or “very good” vision under bright light at far and intermediate distances in Fig. 5a). The lens proved to be safe in terms of visual disturbances as shown by the good results for seven types of disturbance (see Fig. 5b). This correlates with the fewer optical phenomena reported previously with the non-toric model, which are both significantly less than those observed with other EDOF or multifocal IOLs [24]. Our results were similar to those reported by McCabe et al. [3] with the non-toric model at 6 months postsurgery.
As explained in the introduction, some studies have published data on patients implanted with either non-toric or toric AcrySof IQ Vivity IOLs [4,5,6], but they did not include separate sub-analyses for the toric model for a proper assessment of its performance. In a non-interventional study, Gundersen and Potvin [4] assessed the effect of spectacle-induced low myopia (− 0.50 D and − 1.00 D) in the non-dominant eye on the binocular defocus curve in a sample of 40 patients implanted with AcrySof IQ Vivity IOLs. As mentioned, the study considered both non-toric and toric lenses and the outcomes were reported as a single sample, so we cannot analyze any specific results for the toric model. In a similar study, Arrigo et al. [5] reported on real-life experiences in 108 eyes implanted with either non-toric or toric models of the AcrySof IQ Vivity IOLs. They analyzed the visual acuity and refractive outcomes and administered a quality of vision questionnaire. They decided not to perform dedicated analyses on these eyes because of the relatively low number of toric IOLs implanted although the overall patient feedback was very good and the authors concluded that the lens is a well-tolerated choice to correct far and intermediate vision with very few postoperative complications or visual symptoms. Finally, Kandavel et al. [6] also examined both toric (n = 29) and non-toric (n = 35) models of the AcrySof IQ Vivity IOLs. They concluded that their findings supported previous studies in that both toric and non-toric models achieve a similar visual disturbance profile to monofocal IOLs while offering improved near and intermediate vision with less dependence on spectacles.
Only two recent studies have specifically assessed the AcrySof IQ Vivity toric IOL [7, 8]. Barber et al. [7] studied the toric model in 35 eyes of 35 patients. They analyzed the outcomes obtained at 1 month postimplant with the T3 (74%), T4 (17%), and T5 (8.6%) models; however, unfortunately, no eyes were implanted with the T2 model. The authors used the Barrett Universal II toric formula for the IOL power calculation and the target refraction was emmetropia. They also used the ORA SYSTEM® to guide the selection of toric IOL power and alignment. The mean absolute postoperative IOL rotation at 1 month was 1.1 ± 0.2 degrees and remained stable throughout the postoperative follow-up period (1 day and 1 week, P = 0.58). They found that the maximum postoperative rotation observed at 1 month was 3 degrees. Our mean value was 0.74 ± 1.13 degrees, ranging from 0 to 4 degrees, which is in tandem with their outcomes. They measured IOL orientation with digital photography using a slit lamp mounted on an iPhone (Apple; Cupertino, California, USA) and a toric reticle from the toriCAM app (Graham Barrett; version 4.0) as a reference mark [25]. The resulting photographs were analyzed to determine the IOL axis. They observed that the residual refractive astigmatism was ≤ 0.50 D in 94% of eyes and ≤ 1.00 D in 100%. At 97.87% and 100% of eyes for the same levels of residual refractive astigmatism, our results broadly agreed with theirs. At the 1 month follow-up, their mean residual regular astigmatism was 0.21 ± 0.047 D, which was also similar to ours (< 0.25 D). Barber et al. [7] also reported mean monocular UDVA and CDVA scores of 0.18 ± 0.022 and 0.078 ± 0.017 logMAR, respectively. At intermediate distances, their mean monocular UIVA and DCIVA scores were 0.27 ± 0.040 and 0.17 ± 0.025 logMAR, respectively, while these results were slightly better in our study: 0.12 ± 0.07 and 0.14 ± 0.09 logMAR. Finally, the same authors [7] concluded that Vivity toric IOLs had excellent postoperative rotational stability without any lenses rotating by more than 3 degrees at the final 1-month follow-up visit and was effective and predictable for astigmatism correction.
The more recent of the two clinical studies, published by Nguyen et al. [8], assessed 20 patients treated bilaterally with AcrySof IQ Vivity toric IOLs, implanting the T2 model in 10% of eyes, the T3 in 35%, the T4 in 32.5%, and the T5 in 22.5% (the mean IOL cylinder power was 2.01 ± 0.71 D for the whole sample). They used the Barrett Universal II formula/Barrett Toric Calculator (American Society of Cataract and Refractive Surgery) with a target refraction of emmetropia or first minus in all eyes. At 3 months, they reported a mean SE of − 0.55 ± 0.45 D and − 0.63 ± 0.48 D for automated and manual refraction, respectively. The mean residual astigmatism was 0.49 ± 0.34 D and 0.54 ± 0.37 D for automated and subjective refraction. Our results were better, as the mean values were closer to emmetropia. All eyes except one (2.5%) had a residual astigmatism ≤ 1.00 D, whereas in our study all eyes ≤ 1.00 D. At 3 months, they found the binocular UDVA, UIVA (66 cm), and UNVA (40 cm) were 0.01 ± 0.06, 0.08 ± 0.08, and 0.14 ± 0.07 logMAR, respectively, and the monocular CDVA, DCIVA (66 cm), and DCNVA (40 cm) were 0.02 ± 0.06, 0.08 ± 0.08, and 0.05 ± 0.08 logMAR. Our mean values were better and similar for distance vision but worse for intermediate and near: − 0.02 ± 0.08, 0.14 ± 0.09, and 0.23 ± 0.12 logMAR, respectively. IOL rotation (measured using a slit lamp and by rotating a thin beam of light until it aligned with the IOL axis reference mark) from the intended placement axis was 2.5 ± 1.7 degrees at 1 week and 1.7 ± 1.7 degrees at 3 months postimplant. None of the lenses deviated by more than 7 degrees. As previously discussed, our mean rotational value was low, and we found rotation only up to 4 degrees. They administered the QUVID questionnaire to all patients at the 3-month follow-up visit and to 75% of patients (15 of 20) before surgery. All 20 patients reported they were satisfied with their visual outcomes and desired no further surgery. The mean preoperative QUVID score was 4.1 ± 5.3 and it rose to 22.5 ± 18.0 at 3 months postimplant (P < 0.01). Half of the patients (50%) reported no postoperative visual symptoms, whereas the symptoms reported as present “most of the time” were halo (n = 1, 5%), glare (n = 2, 10%), and hazy vision (n = 1, 5%). No patients reported any symptoms that bothered them “quite a bit” or “very much”, and the severity of the visual disturbances was moderate at most for all patients, with hazy vision (n = 2, 10%) being the most common moderately severe symptom. Our results revealed that about 63.83 and 72.34% of patients reported no starburst, halos, or glare, or if they experienced them, did not find them bothersome. For the other four visual disturbances we evaluated, between 82.92% and 97.87% of patients were untroubled at 3 months postimplant.
Unfortunately, there is nothing in the literature about defocus curves for the Vivity toric model although we can compare our results with those obtained with the non-toric model. For example, Bala et al. [2] conducted an international clinical study with 156 patients implanted bilaterally with Vivity non-toric lenses. Based on the binocular defocus curve at 6 months, they determined that patients achieved ≤ 0.0 logMAR for visual acuities from + 0.50 to − 0.50 D, < 0.1 logMAR down to − 1.50 D, and < 0.2 logMAR down to − 2.00 D (50 cm). The defocus curve of ≤ 0.0 logMAR (20/20) obtained in the defocus range of + 0.50 to − 0.50 D suggests the non-toric lens is tolerant to low amounts of residual refractive error. In another study, McCabe et al. [3] assessed 107 patients at 6 months postimplant and found that the Vivity non-toric IOL provided an extended monocular depth of focus compared to the monofocal AcrySof IQ IOL (increase of 0.54 D at 0.2 logMAR). Our results (see Fig. 4) were slightly lower than those of McCabe et al. [3]. Note that our defocus curve was measured under monocular conditions so we can expect to see better results if measured under binocular conditions due to binocular summation [26].
Nevertheless, we obtained a large depth of focus, about 1.75 D, which gives patients a good continuous range from distance to intermediate vision. These two multicenter studies reported good refractive and visual acuity outcomes for the non-toric model at 6 months. Specifically, Bala et al. [2] found that 84.7% of patients achieved a mean absolute SE ≤ 0.50 D (mean of − 0.15 ± 0.32 D). The mean monocular CDVA, DCIVA, and DCNVA were − 0.008 ± 0.007, 0.161 ± 0.013, and 0.414 ± 0.013 logMAR, respectively. Meanwhile, McCabe et al. [3] reported that 91.6% of eyes achieved a SE within ± 0.50 D (mean 0.049 ± 0.345 D). The mean monocular CDVA, DCIVA, and DCNVA were 0.016 ± 0.009, 0.148 ± 0.012, and 0.359 logMAR. Our values were similar for refraction (100% of eyes with SE within ± 0.50 D, mean − 0.10 ± 0.17 D) and distance and intermediate vision, and better for near vision (− 0.02 ± 0.08, 0.14 ± 0.09, and 0.23 ± 0.12 logMAR, for CDVA, DCIVA, and DCNVA, respectively). Limitations of our study include reduced sample size and the inclusion of data of several surgeons in our cohort.







留言 (0)