

記住我

The EDCs (congenital esophageal duplication cysts) are rare congenital anomalies associated to other congenital defects such as esophageal atresia, intestinal duplication, and tracheoesophageal fistulas (1). The incidence of EDCs is estimated at 1:8,200, with 2:1 male predominance (2, 3).
Foregut cysts can be classified as follows: bronchogenic, heterogenous (which include esophageal duplication), neurenteric, or mixed (4). EDCs are surrounded by smooth muscle on a double layer and lined by alimentary epithelium (squamous or enteric). They either attached to the esophagus in a paraesophageal or intramural way (2, 5–7).
We herein report a unique case of an asymptomatic double cystic esophageal duplication associated with VACTERL syndrome without esophageal atresia.
Fabris et al. described a similar case of a patient affected by VATER syndrome with unique esophageal cystic duplication that differs from our case for the esophageal atresia (8).
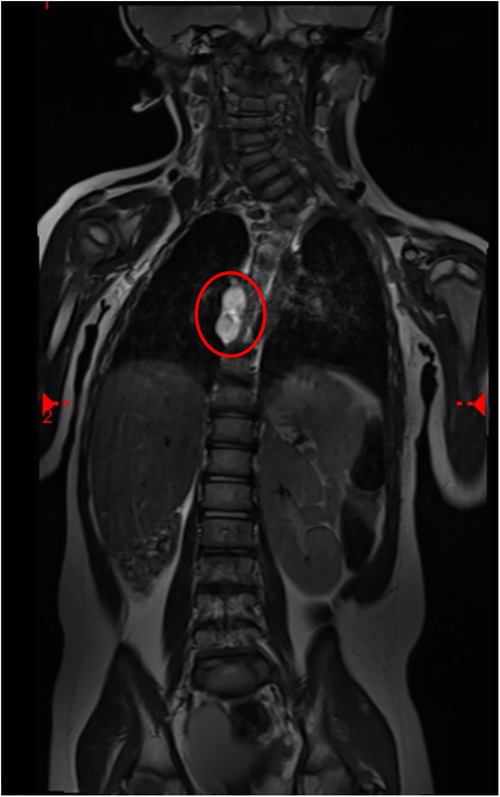
Case descriptionA girl with anorectal malformation (rectovestibular fistula), kidney malformation, and various vertebral defects came to our attention at birth without prenatal screening. VACTERL syndrome was diagnosed. She underwent Peña anoplasty at 4 months without any complications. MRI was conducted at the age of 2 to follow up vertebral defects. MRI accidentally showed a double esophageal duplication (12 mm × 35 mm × 10 mm) at the D7–D9 level (Figure 1). We decided to perform surgery preceded by an esophagoscopy that showed an external compression of the native esophagus under aortic narrowing.
Figure 1. MRI scan of cystic lesions of the esophagus (circle: EDC at the D7–D9 level).
The patient was placed in the lateral decubitus position with the involved side up. A round bolster was placed under the thorax to arch the vertebral column upward to maximize the intercostal spaces of the involved side.
Three trocars were placed: a 5-mm trocar for the optic was put on the fifth intercostal space in the medium axillary, line while two 3-mm operative trocars were positioned on the same intercostal line on the anterior and posterior axillary lines, respectively.
The thorax was insufflated with CO2 with a pressure of 3 mmHg. We did not use single lung ventilation or any ancillary trocar to retract the lung.
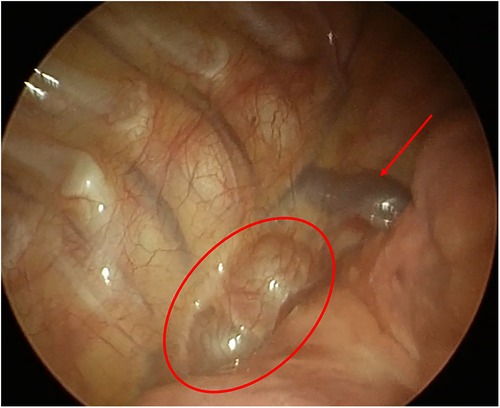
We totally removed the double cists that were on the third distal part of the esophagus, with minimally invasive procedure, by using monopolar and blunt dissection to preserve the vagus nerve, the azygos vein, and the esophageal wall. We closed the muscular defects after excision using separate and absorbable stitches (3-0 Vicryl), and we left thorax drainage (Figure 2).
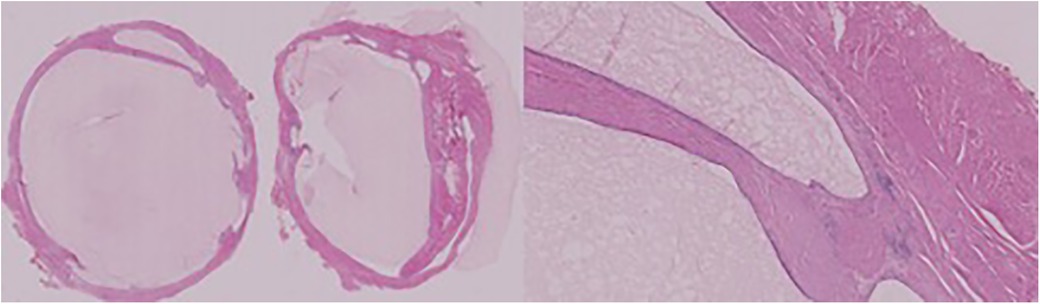
Figure 2. Left: EDCs; right: details of each layer.
The postoperative evolution was uneventful. We removed the drainage, and the patient started oral feeding after 24 h from the surgery. She was discharged after 4 days without any complications. The histological report confirms the diagnosis of double cystic esophageal duplication (Figure 3).
Figure 3. Foregut duplication cysts. Intrathoracic picture (arrow: azygos vein; circle: EDCs).
After 12 months of follow-up, the patient showed any GI symptoms, and oral feeding was compliant Sixteen-month MRI showed normal anatomy of the esophagus (Figure 4).
Figure 4. MRI scan 16 months after surgery (the circle shows no lesions).
DiscussionAmong the mediastinal cysts, EDCs are the most common They might be result of abnormal development of the primitive foregut. They are epithelial-lined structures defined by histologic features and not by their position. Foregut cysts can be classified as follows: bronchogenic, heterogenous (which includes esophageal duplication), neurenteric, or mixed (9).
Most of the esophageal duplication cysts are located in the right posterior-inferior mediastinum. Two-thirds of these lesions are found in the lower third of the esophagus and the other third in the upper/middle third of the esophagus (10).
CT and MRI scans are tools used to study mediastinal masses; however, several types of imaging share similar features.
The clinical presentation of EDCs depends on the dimension and infection of the cyst. About 80% of these lesions are diagnosed in childhood, and the majority are symptomatic such as pulmonary infection, respiratory distress, dysphagia, and nutritional intolerance (5, 11). Most of these cysts are benign, with asymptomatic anomalies that occur during foregut formation; neurological complications are usually the reasons for initial investigation (12).
Early surgical resection is recommended for both symptomatic and asymptomatic patients with EDCs. Developmental aberrations can result from recurrent or persistent pulmonary infections. It is recommended to perform an early elective surgery since the increased rate of infection might make the surgery more difficult (13).
The thoracotomy approach has been the standard of care for the excision of EDCs. However, in recent years, it has been proven that the thoracoscopic approach has been described to be safer for this indication (14–16), since it offers advantages such as reduced postoperative pain, shortened length of hospital stay, and improved cosmesis. In addition, the morbidity of a thoracotomy can be avoided (17).
The literature describes tissue dissecting devices using ultrasound or thermal energy for removal through enucleation or partial resection (14, 17–19).
ConclusionVACTERL syndrome is still an unknown disease since the specific genetic mutation is unknown. The literature describes a few cases of esophageal duplication related to esophagus atresia in patients without VACTERL syndrome (20–24).
Only one case is described by Fabris et al. in 1995 similar to our patient, affected by VACTERL syndrome and esophageal foregut duplication. The patient described had esophageal atresia with a unique EDC (8). Therefore, our case is the first that describe a double cystic esophageal duplication in a VACTERL syndrome without esophageal atresia.
Thoracoscopic removal of ECD is safe, with enormous advantages over thoracotomy.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementWe obtained full informed consent from the minor's parent for the publication of any potentially identifiable images or data included in this article.
Author contributionsGV, ST, VB conceived the case report and wrote the first draft of the manuscript. GV and ER contributed to data collection and the provision of analysis tools. All authors contributed to the article and approved the submitted version.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Khan MU, Saidy KM, Ousulimane DM, Khan MD. Posterior mediastinal gastroenteric cyst in neonate. Saudi Med J. (2004) 25:9557.
2. Arbona JL, Fazzi JG, Mayoral J. Congenital esophageal cysts: case report and review of literature. Am J Gastroenterol. (1984) 79:177–82.6702802
PubMed Abstract | Google Scholar
4. Diehl DL, Cheruvattath R, Facktor MA, Go BD. Infection after endoscopic ultrasound-guided aspiration of mediastinal cysts. Interact Cardiovasc Thorac Surg. (2010) 10:338–40. doi: 10.1510/icvts.2009.217067
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Whitaker JA, Deffenbaugh LD, Cooke AR. Esophageal duplication cyst. Case report. Am J Gastroenterol. (1980) 73:329–32.7416128
PubMed Abstract | Google Scholar
6. Wang B, Hunter WJ, Bin-Sagheer S, Bewtra C. Rare potential pitfall in endoscopic ultrasound-guided fine needle aspiration biopsy in gastric duplication cyst: a case report. Acta Cytol. (2009) 53:219–22. doi: 10.1159/000325129
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Fabris S, Cavazzana A, Gamba P. VATER syndrome and esophageal foregut duplication. Pediatr Surg Int. (1995) 10:252–4. doi: 10.1007/BF00177172
CrossRef Full Text | Google Scholar
9. Parikh D, Short M. Chapter 16: Esophageal duplication cyst. In: Puri P, editor. Pediatric surgery. Switzerland AG, Berlin, Heidelberg: Springer (2017.
10. Bhatia V, Tajika M, Rastogi A. Upper gastrointestinal submucosal lesions clinical and endosonographic evaluation and management. Trop Gastroenterol. (2010) 31:5–29.20860221
PubMed Abstract | Google Scholar
11. Cevasco M, Menard MT, Bafford R, McNamee CJ. Acute infectious pseudoaneurysm of the descending thoracic aorta and review of infectious aortitis. Vasc Endovascular Surg. (2010) 44:697–700. doi: 10.1177/1538574410376449
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Leblanc C, Baron M, Desselas E, Phan MH, Rybak A, Thouvenin G, et al. Congenital pulmonary airway malformations: state-of-the-art review for pediatrician’s use. Eur J Pediatr. (2017) 176:1559–71. doi: 10.1007/s00431-017-3032-7
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Partrick DA, Rothenberg SS. Thoracoscopic resection of mediastinal masses in infants and children: an evaluation of technique and results. J Pediatr Surg. (2001) 36(08):1165–7. doi: 10.1053/jpsu.2001.25740
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Michel JL, Revillon Y, Montupet P, Sauvat F, Sarnacki S, Sayegh N, et al. Thoracoscopic treatment of mediastinal cysts in children. J Pediatr Surg. (1998) 33(12):1745–8. doi: 10.1016/S0022-3468(98)90276-7
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Hirose S, Clifton MS, Bratton B, Harrison MR, Farmer DL, Nobuhara KK, et al. Thoracoscopic resection of foregut duplication cysts. J Laparoendosc Adv Surg Tech A. (2006) 16(05):526–9. doi: 10.1089/lap.2006.16.526
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Tiwari S, Kothari P, Gupta A, Jayaswal S, Dikshit V, Kekre G. Thoracoscopic resection of foregut duplication cyst in a neonate. J Minim Access Surg. (2021) 17(01):88–90. doi: 10.4103/jmas.JMAS_58_20
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Sinha SK, Khanolkar A, Thakkar NC, Raj P, Kumar P, Bhalotra AR. Thoracoscopic excision of foregut duplication cyst: a case report and review of literature. J Indian Assoc Pediatr Surg. (2016) 21(03):147–9. doi: 10.4103/0971-9261.182591
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Bratu I, Laberge JM, Flageole H, Bouchard S. Foregut duplications: is there an advantage to thoracoscopic resection? J Pediatr Surg. (2005) 40(1):138–41. doi: 10.1016/j.jpedsurg.2004.09.025
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Inan M, Basaran UN, Aksu B, Dereli M, Dortdogan Z. Esophageal duplication associated with esophageal atresia and tracheoesophageal fistula in a child. Int J Pediatr Otorhinolaryngol Extra. (2007) 2:202–5. doi: 10.1016/j.pedex.2007.05.010
CrossRef Full Text | Google Scholar
22. Janik JS, Hernandez AM, Lilly JR. Esophageal atresia with proximal pouch tracheoesophageal fistula and noncommunicating esophageal duplication. Pediatr Surg Int. (1988) 3:70–3. doi: 10.1007/BF00177086
CrossRef Full Text | Google Scholar
23. Escobar MA Jr, Welke KF, Holland RM, Caty MG. Esophageal atresia associated with a rare vascular ring and esophageal duplication diverticulum: a case report and review of the literature. J Pediatr Surg. (2012) 47:1926–9. doi: 10.1016/j.jpedsurg.2012.07.051
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Knod JL, Garrison AP, Frischer JS, Dickie B. Foregut duplication cyst associated with esophageal atresia and tracheoesophageal fistula: a case report and literature review. J Pediatr Surg. (2013) 48(5):E5–7. doi: 10.1016/j.jpedsurg.2013.02.071
留言 (0)