
記住我

Older trauma patients are known to have greater mortality after traumatic injury than their younger counterparts.1 Patients who survive serious injuries often suffer permanent disability and functional decline. In light of this, palliative care has become an increased focus for the surgical community.2,3 In 2017, the American College of Surgeons-Trauma Quality Improvement Program published guidelines outlining an early approach to palliative care highlighting the following goals in the first 24 hours: providing an early prognosis, identifying a medical surrogate decision maker, and obtaining an advance directive when available.4
Few have assessed the clinical significance of advance directives when it comes to the care of the injured patient. It has been noted that the presence of a “do not resuscitate” order is associated with adverse outcomes after traumatic injury and 5.2-fold increased odds of mortality.5 However, in patients with a significant injury and unlikely return to an acceptable quality of life, transitioning to comfort care and avoiding suffering may be the desired outcome. Early implementation of comfort care measures and “withdrawal of life sustaining support” (WLSS) may be the treatment of choice to avoid complications or futile procedures. A review of advanced directives in the trauma intensive care unit (ICU) suggested that, although advanced directives documenting patient wishes have increased, their utility may be complicated by vague wording and the unique circumstances regarding trauma.6 A single center study of trauma patients found that multidisciplinary family meetings to discuss goals of care often occur after life-prolonging procedures such as a tracheostomy or a feeding tube placement, suggesting that these discussions often take place when death was imminent and other options are exhausted.7 The relationship between advance directives limiting care (ADLC) and WLSS is critical to study, as one study estimated that more than 80% of older trauma patients who died in the ICU did so after WLSS.8
The objective of this study was to evaluate the impact of ADLC on clinical outcomes for older trauma patients in a large national database. A propensity match to assess similar patients who did and did not have ADLC was performed. We hypothesized that patients with ADLC are more likely to undergo WLSS compared with patients without ADLC. We also hypothesized that hospital factors indicating a poor prognosis would have greater impact on WLSS than ADLC.
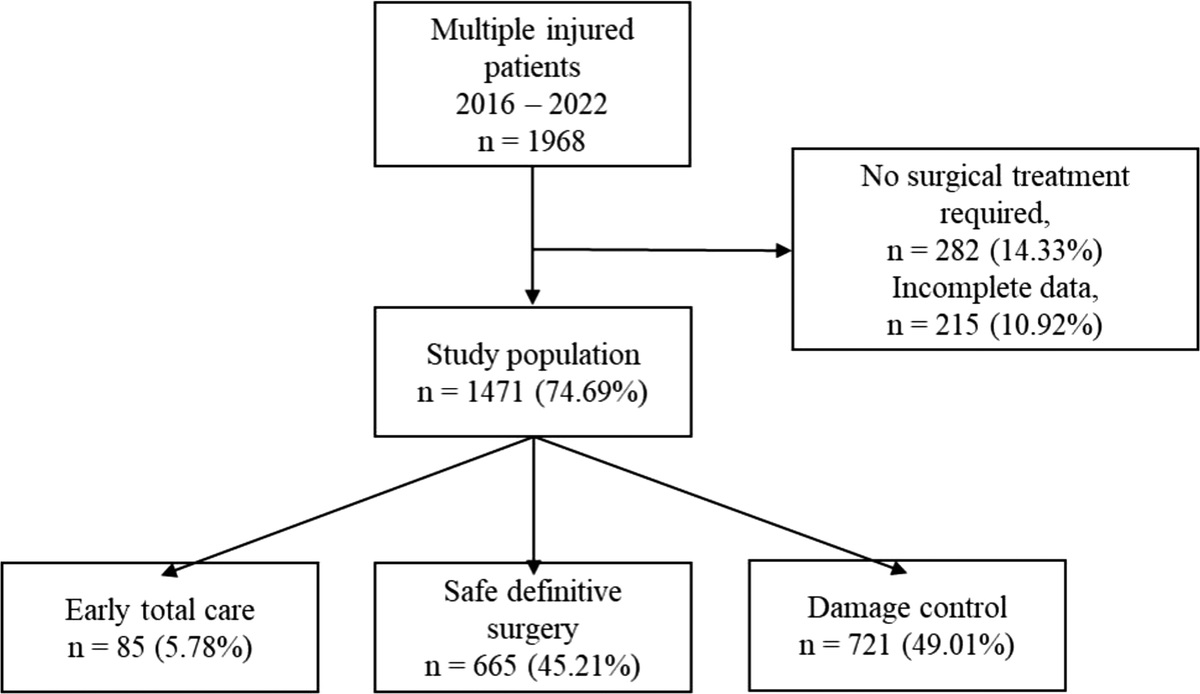
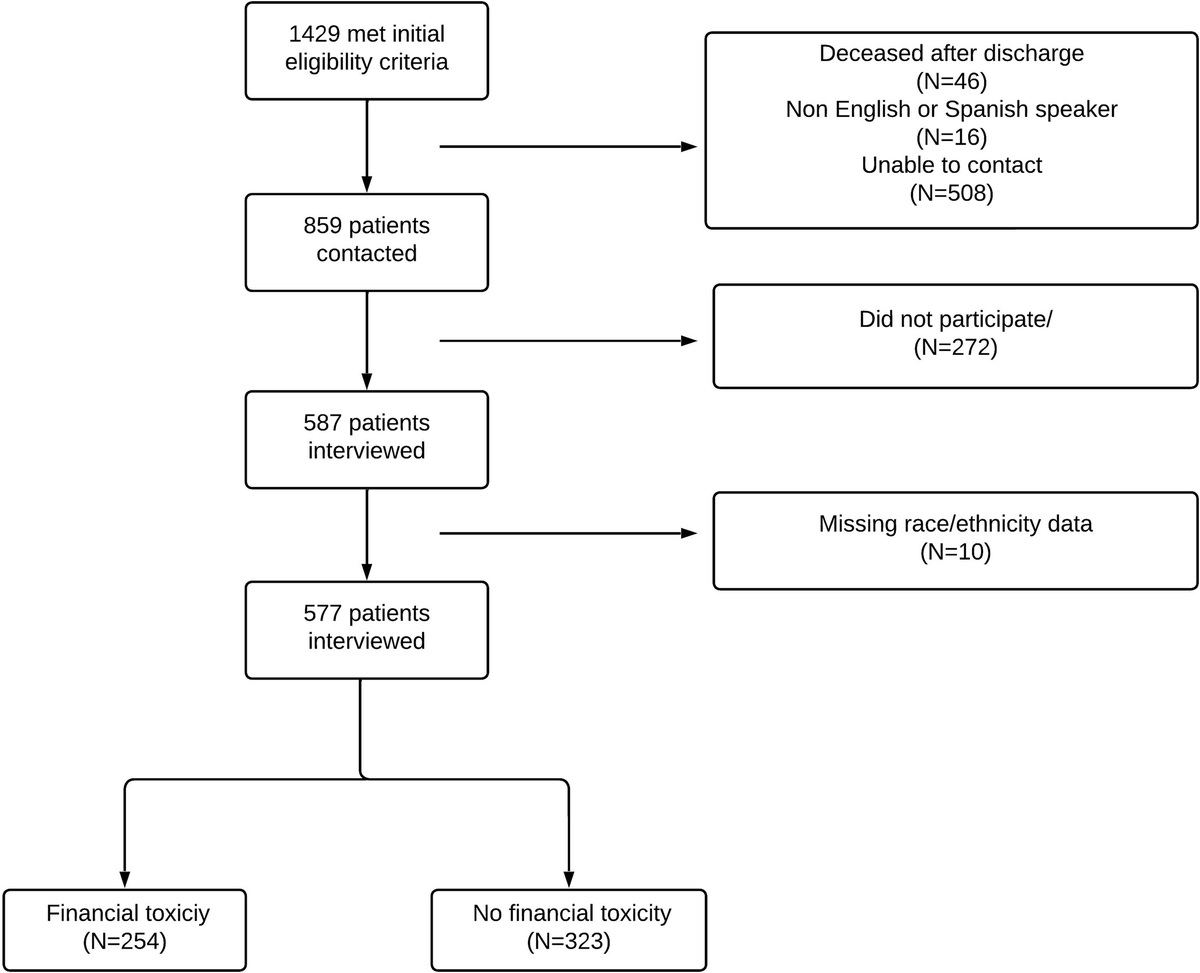
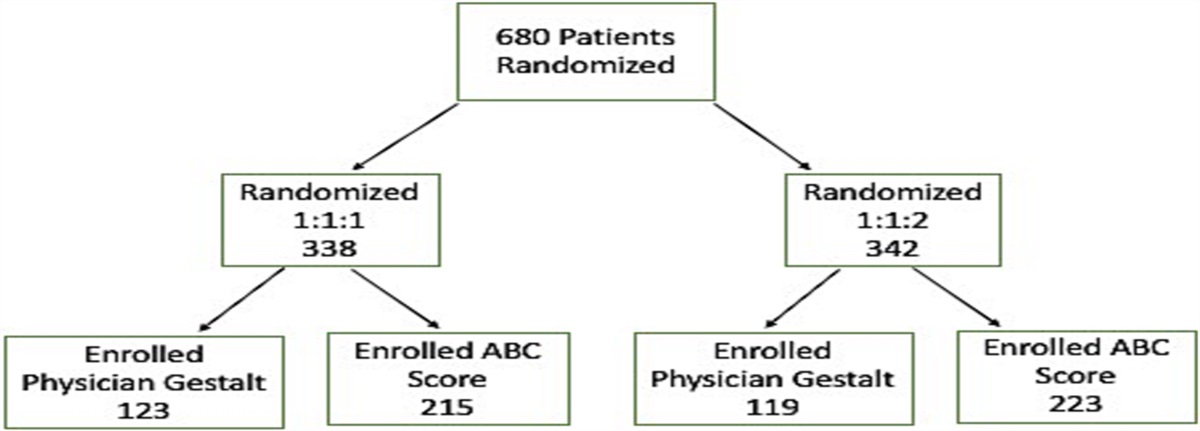
METHODSThis retrospective study included the 2017 to 2018 iterations of the ACS-TQP database, which is a large national database containing trauma registry information from participating level I and II US trauma centers.9 The TQP database was queried for all patients at least 65 years of age. Patients were excluded if they died within 24 hours of admission or if age data was missing (Fig. 1). Study design was formed using a Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist (supplemental information: STROBE checklist, https://links.lww.com/TA/C809).10
 Figure 1:
Figure 1: Flowchart of study design.
Patients were categorized based on the presence of an ADLC as captured from TQP variables. Advance directives limiting care was defined per TQP definitions as a written document limiting life-sustaining therapy that was present upon presentation to the TQP submitting facility. The primary outcome was WLSS, which was defined in TQP as a withdrawal or decision to withhold life-supporting treatment. Secondary outcomes included time to WLSS, hospital length of stay (LOS), ICU LOS, unplanned admission to the ICU, unplanned surgery, in-hospital cardiac arrest, ventilator LOS, and discharge disposition. Variables of interest included age, gender, race/ethnicity, mechanisms of injury, Injury Severity Score (ISS), prehospital cardiac arrest, and preexisting conditions, such as heart failure, dementia, cirrhosis, and disseminated cancer. Race and ethnicity groups, as collected in TQP, were included as adjustor variables for regression, as it is known that the use of ADLC differs between social and demographic groups.11 Patients were characterized as being of White, non-Hispanic race and ethnicity group or of a non-White race, non-Hispanic ethnicity or of Hispanic ethnicity group. Descriptive analysis was performed to delineate the study population's demographic characteristics relative to presence of ADLC. Categorical and binary variables were compared using χ2 testing. Continuous variables were reported as medians with interquartile ranges and compared using the Wilcoxon rank-sum test. Multivariate modeling was also performed to determine demographic and clinical factors associated with WLSS. Variables for multivariable regression were included if considered clinically salient. Further multivariable analyses of individual racial or ethnicity groups were not performed.
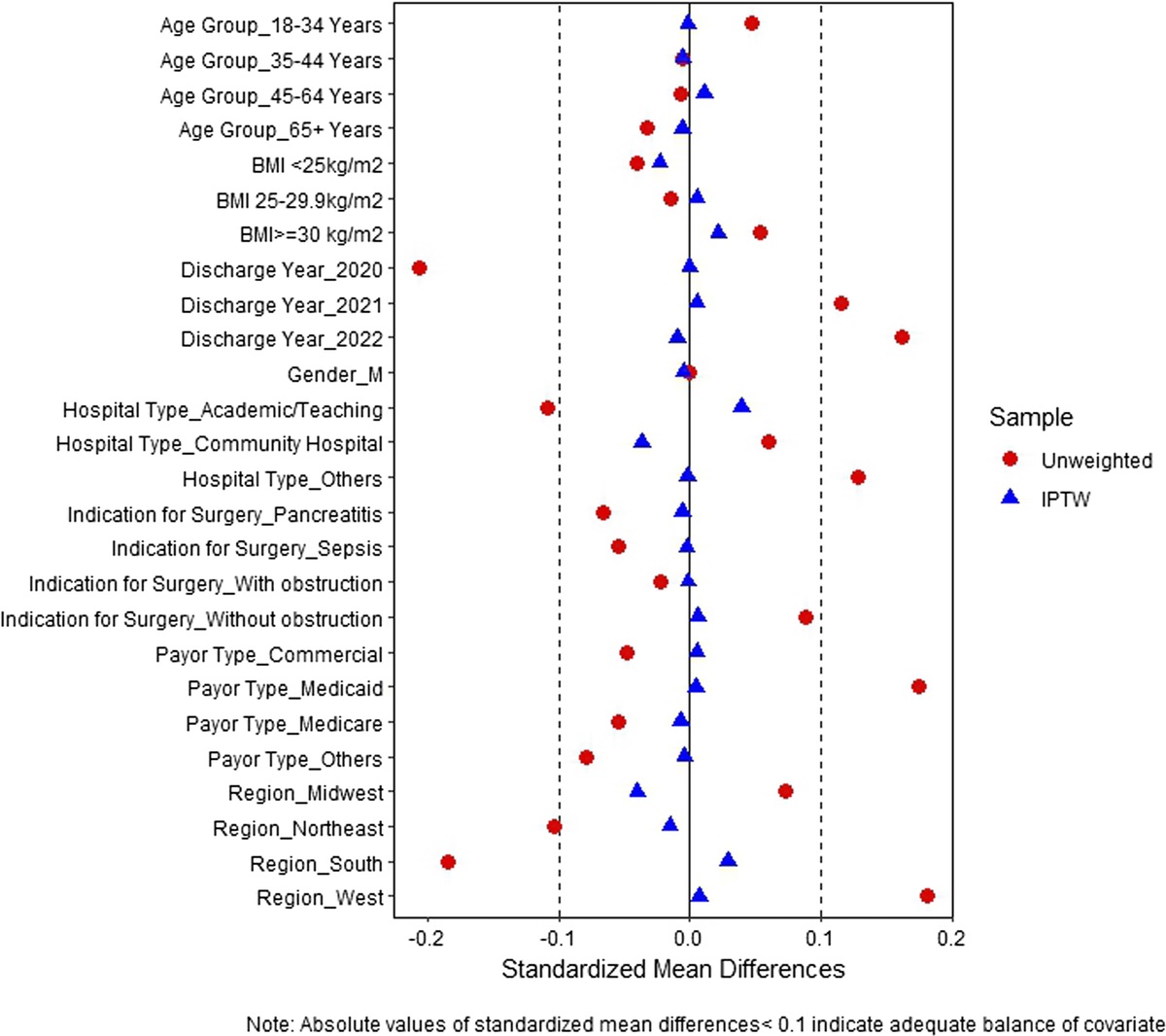
Propensity score matching was performed to control for confounding variables between the unmatched ADLC group and non-ADLC group, given the differences in size of the groups. A 1:1 propensity matching model was created on the basis of presence of ADLC with age, race/ethnicity, gender, injury type, and ISS as covariates. Nearest neighbor matching was performed without replacement and a caliper size of 0.05 to generate a cohort of patients with and without ADLC. Standardized differences were used to estimate the balance of covariates used in propensity scoring. A standardized difference between −0.1 and 0.1 for each covariate was considered to indicate a good balance between the two groups. A mixed-effect logistic regression was then performed using the matched cohorts to determine differences in outcomes.12
All analyses were performed using STATA SE/14 (StataCorp, College Station TX). Results are presented as odds ratio (OR) with 95% confidence intervals (95% CI). Findings were considered significant if p ≤ 0.05. p Values were not corrected for multiple hypothesis testing. This study was considered exempt by the local institutional review board (IRB 20211390).
RESULTSA total of 597,840 patients older than 65 years were identified, of whom 44,001 (7.36%) had an ADLC. Patients with ADLC, in an unmatched analysis, were significantly younger, female, and of White race, non-Hispanic ethnicity compared with those without ADLC (Table 1). Patients in both groups were more likely to have Medicare insurance. Patients with ADLC were significantly more likely to have a history of dementia (32.05% vs. 11.30%, p < 0.001).
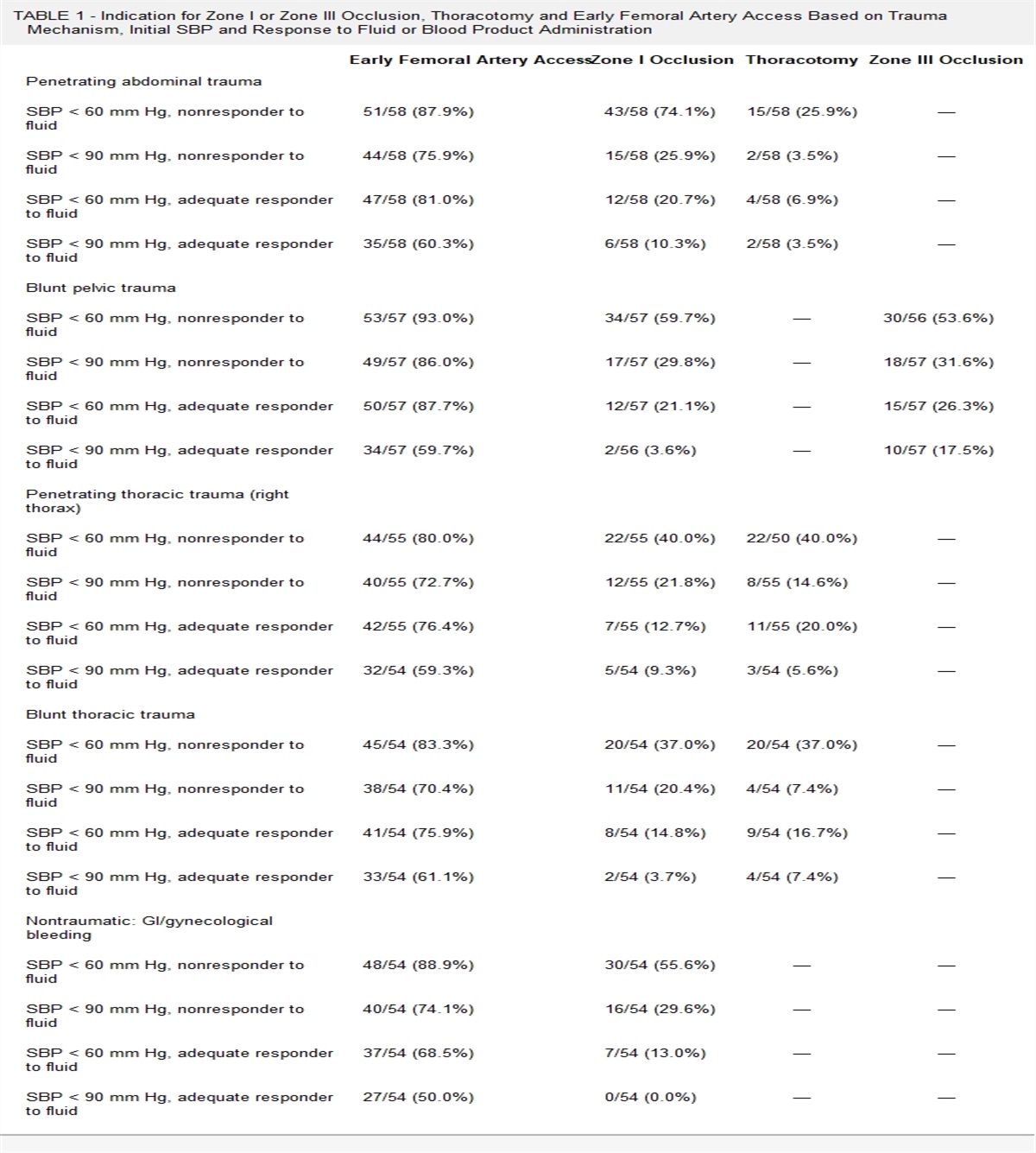
TABLE 1 - Demographics of Unmatched Trauma Patients, 65 y and Older Advance Directive Group (n = 44,001) (7.36%) No Advance Directive Group (n = 553,839) (92.64%) p Age, median (IQR), y 77 (70–83) 82 (76–86) <0.001 Male sex, n (%) 16,870 (38.34%) 246,397 (44.49%) <0.001 Non-Hispanic White, n (%) 39,556 (89.90%) 444,332 (80.23%) <0.001 Blunt mechanism, n (%) 43,080 (97.91%) 532,630 (96.17%) <0.001 ISS, median (IQR) 9 (5–10) 9 (4–10) <0.001 Preexisting conditions COPD, n (%) 7,905 (17.97%) 70,372 (12.71%) <0.001 CHF, n (%) 6,578 (14.95%) 47,043 (8.49%) <0.001 CKD, n (%) 1,936 (4.40%) 18,749 (3.39%) <0.001 Cirrhosis, n (%) 646 (1.47%) 5,856 (1.06%) <0.001 Disseminated cancer, n (%) 1,158 (2.63) 6,917 (1.25%) <0.001 Dementia, n (%) 14,102 (32.05%) 62,571 (11.30%) <0.001 Outcomes ICU LOS, mean (STD) 3 (2–5) 3 (2–5) <0.001 Ventilator days, mean (STD) 3 (2–8) 3 (2–6) <0.001 Unplanned return to the OR, n (%) 112 (0.25%) 1,401 (0.25%) 0.949 Unplanned admissions to the ICU, n (%) 1,382 (3.14%) 10,819 (1.95%) <0.001 WLSS, n (%) 3,381 (7.68%) 13,763 (2.48%) <0.001 Days to withdrawal, median (IQR) 3 (2–7) 4 (2–9) <0.001 Hospital LOS, median (IQR) 5 (3–7) 5 (3–7) <0.001 Disposition at discharge <0.001* Home (without HHC), n (%) 8,485 (19.87%) 160,385 (31.65%) LTACH, n (%) 5,395 (12.64%) 85,599 (16.89%) SNF, n (%) 16,875 (39.53%) 159,173 (31.42%) Hospice, n (%) 2,882 (6.75%) 6,917 (1.37%) Home (with HHC), n (%) 3,703 (8.67%) 55,540 (10.96%) Deceased/expired, n (%) 4,045 (9.47%) 18,444 (3.64%)IQR, interquartile range; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; CKD, chronic kidney disease; GCS, Glasgow Coma Scale; HHC, home health care; LSS, life sustaining support; OR, operating room; STD, standard deviation; WLSS, withdrawal of life sustaining support.
*p Value for associated block of variables.
Unmatched patients were further analyzed on clinical outcomes. Patients with advance directives had significantly lower ICU LOS, hospital LOS, and duration of ventilation (Table 2). There were no significant differences in incidences of in-hospital cardiac arrests or ventilator-associated pneumonia between patients with and without ADLC. While patients with ADLC were more likely to be unexpectedly admitted to the ICU (3.14% vs. 1.95%, p < 0.001), the presence of an advance directive had no effect on unplanned surgical interventions (0.25% vs. 0.25%, p = 0.949). Patients with ADLC underwent WLSS more often (7.68% vs. 2.48%, p < 0.001) and transition to comfort care occurred 24 hours earlier when compared with patients without ADLC (3 days vs. 4 days, p < 0.001). Patients with ADLC were also discharged to hospice more often than their counterparts without ADLC (6.75% vs. 1.37%, p < 0.001).
TABLE 2 - Demographics and Outcomes of Matched Trauma Patients Advance Directive Group (n = 39,138) No Advance Directive Group (n = 39,138) p Age, median (IQR) 82 (76–86) 82 (76–86) 0.722 Male sex, n (%) 15,204 (38.85%) 15,204 (38.85%) 1.000 Non-Hispanic White, n (%) 35,291(90.17%) 35,322 (90.25%) 0.709 Blunt mechanism, n (%) 38,298 (97.85%) 38,375 (98.05%) 0.052 ISS, median (IQR) 9 (5–12) 9 (5–12) 0.664 COPD, n (%) 6,903 (17.64%) 6,887 (17.60%) 0.881 CHF, n (%) 5,882 (15.03%) 5,897 (15.07%) 0.881 CKD, n (%) 1,647 (4.21%) 1,624 (4.15%) 0.681 Cirrhosis, n (%) 581 (1.48%) 520 (1.33%) 0.064 Disseminated cancer, n (%) 1,038 (2.65%) 991 (2.53%) 0.290 Dementia, n (%) 12,499 (31.94%) 12,470 (31.86%) 0.824 Outcomes Advance Directive Group (n = 39,138) No Advance Directive Group (n = 39,138) p ICU LOS, median (IQR) 3 (2–5) 3 (2–5) <0.001 Ventilator days, median (IQR) 3 (2–6) 3 (2–7) 0.002 Unplanned return to the OR, n (%) 106 (0.27) 107 (0.27) 0.945 Unplanned admissions to the ICU, n (%) 1,279 (3.27%) 1,013 (2.59%) <0.001 In-hospital cardiac arrest, n (%) 288 (0.74%) 298 (0.76%) 0.678 WLSS, n (%) 3,384 (8.64%) 1,722 (4.40%) <0.001 Days to withdrawal, median (IQR) 3 (2–7) 4 (2–8) <0.001 Hospital LOS, median (IQR) 5 (4–7) 4 (3–7) 0.167*p Value for associated block of variables.
From the initial study population, a total of 78,276 patients were matched to form 39,138 pairs for analysis. The propensity match was well balanced with standardized balances between −0.1 and 0.1 for each covariate used in the matching process (Fig. 2). Matched groups were similar in age, gender distribution, race/ethnicity, injury mechanism, ISS, and comorbidities (Table 2). However, patients with ADLC continued to undergo WLSS more often than those without (8.64% vs. 4.40%, p < 0.001) and at a time period approximately 24 hours earlier than those without ADLC (3 days vs. 4 days, p < 0.001). In an adjusted logistic regression of WLSS, matched patients were more likely to undergo WLSS if they were older, male, and more severely injured (Table 3). Patients were also more likely to undergo WLSS if they had a preexisting comorbidity of heart failure, chronic obstructive pulmonary disease, disseminated cancer, renal disease or cirrhosis. However, there was no association between dementia and WLSS. In this analysis, ADLC was associated with WLSS (OR, 2.38; 95% CI, 2.22–2.55), however, adverse hospital events including an unplanned ICU admission or in-hospital cardiac arrests were more associated with WLSS (Table 3).
 Figure 2:
Figure 2: Graph of standardized differences before and after propensity match.
TABLE 3 - Mixed Effects Logistic Regression of Odds of Progression to Withdrawal of Life Sustaining Support for 39,198 Matched Pairs Variables OR 95% CI p Age 1.02 1.01–1.02 <0.001 Male sex 1.43 1.36–1.56 <0.001 Blunt mechanism of injury 0.54 0.45–0.66 <0.001 White, non-Hispanic race 1.09 0.98–1.22 0.095 Comorbidities Dementia 1.05 0.97–1.13 0.154 CHF 1.29 1.18–1.42 <0.001 COPD 1.30 1.19–1.41 <0.001 Disseminated cancer 1.79 1.51–2.13 <0.001 ESRD 1.51 1.31–1.75 <0.001 Cirrhosis 1.84 1.47–2.32 <0.001 ISS (relative to score 1–9) 10–15 2.08 1.89–2.29 <0.001 16–24 4.62 4.1805.12 <0.001 25+ 23.84 21.57–26.36 <0.001 Unplanned return to OR 1.13 0.76–1.68 0.522 Unplanned ICU admission 3.29 2.89–3.75 <0.001 Advance directive limiting care 2.38 2.22–2.55 <0.001 In-hospital cardiac arrest 4.97 4.02–6.15 <0.001ESRD, end-stage renal disease.
Our results reveal that only a small percentage of older trauma patients have advance directives on file at the time of admission, which is significantly less than previous systematic reviews of advance directive completion.4 Other studies examining advance directives among trauma patients demonstrated an approximate rate of preinjury ADLC of 12%, which is greater than that noted in this study.13,14 This study's demographics are consistent with those seen in other investigations of ADLC, with more advance directives held by female patients, individuals from White non-Hispanic race and ethnicity groups, and patients with preexisting comorbidities.13,15,16
Despite the small number of patients who presented with ADLC, our study showed one intended benefit of advance care planning as patients with ADLC underwent WLSS approximately 24 hours earlier compared with those who did not have advance directives. This finding suggests that family members may have felt more at ease with transitioning to comfort care measures before another adverse event occurred, and in general, families may be more likely to make such transitions with clear advance directives. However, prior studies have highlighted the inherent limitations of advance directives' language and meaning.11,17–19 Gordy et al.6 note the vague wording and definition of medical futility in many advance directives. The meanings of “terminal condition” and “life-sustaining treatment,” terms that are often included in advance directives, may be subject to interpretation without specific medical explanations resulting in significant stress for patients and their families. As demonstrated by Thompson et al.,20 the interpretation of an example advance directive varied significantly between practitioners due to vague wording of the conditions that would prompt withholding treatment. In turn, the ambiguity in a document originally intended to eliminate indecision only adds to the anxiety of critical illness.
Certainly, early and forthright discussions initiated by healthcare providers could offset the ambiguity of advance directives. Studies demonstrate the importance of family discussions with physicians regarding updates and prognosis.21 Given the busy nature of critical care, physicians have competing demands and must balance providing intensive care with leading family discussions outlining prognosis and appropriate goals of care.22–24 As a result, physicians may delay such conversations in order to better assess patient and family readiness.25 Our study shows that adverse hospital events are more predictive of WLSS as they serve as objective evidence of patient frailty and decline. Physicians are compelled to present unexpected adverse events and their impact on a patient’s prognosis leading to subsequent conversations addressing goals of care. A national study of surgeons suggested they experience moral distress when providing non-beneficial invasive care to patients at the end of life, but may feel pressure to pursue these treatments to give the family or patient time to cope with a severe condition; an adverse event may be the precipitating factor which allows the treatment team to feel more confident to pursue difficult conversations about WLSS, particularly in cases where a patient does not have an advance directive limiting care or treatment (ADLC/T).26 This “waiting for the sky to fall” may seem easier in terms of presenting objective clinical data; however, it often comes at the cost of patient suffering. Thus, early discussions regarding palliative care are highly recommended in an effort to preserve patient autonomy and to delineate their wishes prior to a decline in clinical condition.6,27
International studies of palliative care trends demonstrate that increased awareness of palliative care intervention via public health strategies, insurance coverage, and local laws may lead to increased advance care planning.28 Formulation of laws regulating ADLC practices also demonstrated decreased uncertainty and ambiguity in the formulation and wording of such documents.29 In addition, proposed interventions to aid clinician communication have demonstrated improved completion of ADLC.30 Prior studies have suggested that the presence of an ADLC was associated with adverse events such as mortality, but these effects are not apparent after propensity matching, suggesting that trauma surgeons do not simply “give up” on patients with preexisting ADLC.5
Our study demonstrated an increased rate of unexpected ICU admissions in patients with advance directives. Previous studies have demonstrated higher rates of undertriage in geriatric trauma patients, suggesting deterioration after a floor admission as a possible reason for this increase.31–33 Other studies demonstrated that approximately 16% of low-risk geriatric patients required an unplanned ICU admission during their hospitalization, with increased risk in patients with preexisting comorbidity.34 However, the exact reason for these unplanned ICU admissions is not well identified using this dataset and would warrant study in a population with ADLC.
There are several limitations to this retrospective study. First, this study relies on an administrative database and, as such, the accuracy of individual entries cannot be verified by the study team. The listing of ADLC may also be affected by this loss in data given that some patients may not have a precompleted ADLC available due to electronic medical record differences. Advance directives may also encompass several different types of documents, which may have different limitations in treatment which cannot be examined by an aggregated database. In addition, the use of an administrative database does not allow for the full assessment of complex clinical decisions, such as determining whether certain outcomes were “appropriate” or the factors that directly led to WLSS. We also recognize that, given the large sample size in this study, some variables appear statistically significant although they are not clinically significant. Despite such limitations, we believe that the impact of potential inaccuracies on the findings is limited by the large cohort of patients analyzed in this study. The complex medical and social decisions that are involved in the withdrawal of life-sustaining support in a critically injured patient are often unique to the patient and their family and cannot be well described by a de-identified database.
Only a small proportion of geriatric trauma patients have ADLC on admission. While ADLC was predictive of WLSS, adverse hospital events were more strongly associated with WLSS. To ensure patient-centered care, surgeons should delineate goals of care early regardless of whether or not the patient has an advance directive. Consequently, this may lead to a decrease in futile interventions. The discussion of end-of-life care in the trauma ICU remains a fluid field that requires more investigation.
AUTHORSHIPAll authors were involved in the conception or design of this work. A.B., V.P.H., and A.R. collected data and performed statistical analysis. A.B. and A.R. created figures and tables All authors drafted and revised the abstract. All authors drafted the article. All authors edited and critically reviewed the final article.
ACKNOWLEDGMENTThis publication was made possible by the Clinical and Translational Science Collaborative of Cleveland, KL2TR000440 from the National Center for Advancing Translational Sciences (NCATS) component of the National Institutes of Health and NIH roadmap for Medical Research.
DISCLOSUREV.P.H.'s spouse is a consultant for Atricure, Zimmer Biomet, Sig Medical and Medtronic, but these relationships have not influenced this work in any way.
This study was funded by the Northern Ohio Trauma System and Ohio Department of Public Health.
V.P.H. is supported by the CTSC of Cleveland (KL2TR002547).
This study was funded by the Ohio Department of Public Health, Division of EMS (grant 17504).
REFERENCES 1. Hashmi A, Ibrahim-Zada I, Rhee P, Aziz H, Fain MJ, Friese RS, et al. Predictors of mortality in geriatric trauma patients: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2014;76(3):894–901. 2. Gioffrè-Florio M, Murabito LM, Visalli C, Pergolizzi FP, Famà F. Trauma in elderly patients: a study of prevalence, comorbidities and gender differences. G Chir. 2018;39(1):35–40. 3. Suwanabol PA, Li Y, Abrahamse P, De Roo AC, Vu JV, Silveira MJ, et al. Functional and cognitive decline among older adults after high-risk surgery. Ann Surg. 2022;275(1):e132–e139. 4. Yadav KN, Gabler NB, Cooney E, Kent S, Kim J, Herbst N, et al. Approximately one in three US adults completes any type of advance directive for end-of-life care. Health Aff. 2017;36(7):1244–1251. 5. Jawa RS, Shapiro MJ, McCormack JE, Huang EC, Rutigliano DN, Vosswinkel JA. Preadmission do not resuscitate advanced directive is associated with adverse outcomes following acute traumatic injury. Am J Surg. 2015;210(5):814–821. 6. Gordy S, Klein E. Advance directives in the trauma intensive care unit: do they really matter?Int J Crit Illn Inj Sci. 2011;1(2):132–137. 7. Bhangu JK, Young BT, Posillico S, Ladhani HA, Zolin SJ, Claridge JA, et al. Goals of care discussions for the imminently dying trauma patient. J Surg Res. 2020;246:269–273. 8. Cooper Z, Rivara FP, Wang J, MacKenzie EJ, Jurkovich GJ. Racial disparities in intensity of care at the end-of-life: are trauma patients the same as the rest?J Health Care Poor Underserved. 2012;23(2):857–874. 10. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. 11. Haines KL, Nguyen BP, Antonescu I, Freeman J, Cox C, Krishnamoorthy V, et al. Insurance status and ethnicity impact health disparities in rates of advance directives in trauma. Am Surg. 2021;31348211011115. 12. Rosenbaum PR, Rubin DB. Constructing a Control Group Using Multivariate Matched Sampling Methods That Incorporate the Propensity Score. null. 1985;39(1):33–38. 13. Lee JS, Khan AD, Dorlac WC, Dunn J, McIntyre RC, Wright FL, et al. The patient’s voice matters: the impact of advance directives on elderly trauma patients. J Trauma Acute Care Surg. 2022;92(2):339–346. 14. Graw JA, Burchard R. Completion rates of advance directives in a trauma emergency room: association with age. Emerg Med Int. 2021;2021:5537599. 15. Inoue M, Ihara E, Terrillion A. Making your wishes known: who completes an advance directive and shares it with their health care team or loved ones?J Appl Gerontol. 2019;38(12):1746–1762. 16. Hill LA, Waller CJ, Borgert AJ, Kallies KJ, Cogbill TH. Impact of advance directives on outcomes and charges in elderly trauma patients. J Palliat Med. 2020;23(7):944–949. 17. Köstenberger M, Diegelmann S, Terlutter R, Bidmon S, Neuwersch S, Likar R. Advance directives in Austrian intensive care units: an analysis of prevalence and barriers. Resusc Plus. 2020;3:100014. 18. Glick KL, Mackay KM, Balasingam S, Dolan KR, Casper-Isaac S. Advance directives: barriers to completion. J N Y State Nurses Assoc. 1998;29(1):4–8. 19. Van Scoy LJ, Howrylak J, Nguyen A, Chen M, Sherman M. Family structure, experiences with end-of-life decision making, and who asked about advance directives impacts advance directive completion rates. J Palliat Med. 2014;17(10):1099–1106. 20. Thompson T, Barbour R, Schwartz L. Adherence to advance directives in critical care decision making: vignette study. BMJ. 2003;327(7422):1011–1010. 21. Verhaeghe S, Defloor T, Van Zuuren F, Duijnstee M, Grypdonck M. The needs and experiences of family members of adult patients in an intensive care unit: a review of the literature. J Clin Nurs. 2005;14(4):501–509. 22. Butler R, Monsalve M, Thomas GW, Herman T, Segre AM, Polgreen PM, et al. Estimating time physicians and other health care workers spend with patients in an intensive care unit using a sensor network. Am J Med. 2018;131(8):972.e9–972.e15. 23. Lund S, Richardson A, May C. Barriers to advance care planning at the end of life: an explanatory systematic review of implementation studies. PLoS One. 2015;10(2):e0116629. 24. Schickedanz AD, Schillinger D, Landefeld CS, Knight SJ, Williams BA, Sudore RL. A clinical framework for improving the advance care planning process: start with patients’ self-identified barriers. J Am Geriatr Soc. 2009;57(1):31–39. 25. Brighton LJ, Bristowe K. Communication in palliative care: talking about the end of life, before the end of life. Postgrad Med J. 2016;92(1090):466–470. 26. Zimmermann CJ, Taylor LJ, Tucholka JL, Buffington A, Brasel K, Arnold R, et al. The association between factors promoting nonbeneficial surgery and moral distress: a National Survey of Surgeons. Ann Surg. 2022;276(1):94–100. 27. Edsall A, Howard S, Dewey EN, Siegel T, Zonies D, Brasel K, et al. Critical decisions in the trauma intensive care unit: are we practicing primary palliative care?J Trauma Acute Care Surg. 2021;91(5):886–890. 28. Huemer M, Jahn-Kuch D, Hofmann G, Andritsch E, Farkas C, Schaupp W, et al. Trends and patterns in the public awareness of palliative care, euthanasia, and end-of-life decisions in 3 central European countries using big data analysis from Google: retrospective analysis. J Med Internet Res. 2021;23(9):e28635. 29. Rodríguez-Prat A, Monforte-Royo C, Porta-Sales J, Escribano X, Balaguer A. Patient perspectives of dignity, autonomy and control at the end of life: systematic review and meta-ethnography. PLoS One. 2016;11(3):e0151435. 30. Schaefer KG, Block SD. Physician communication with families in the ICU: evidence-based strategies for improvement. Curr Opin Crit Care. 2009;15(6):569–577. 31. Amoako J, Evans S, Brown NV, Khaliqdina S, Caterino JM. Identifying predictors of undertriage in injured older adults after implementation of statewide geriatric trauma triage criteria. Acad Emerg Med. 2019;26(6):648–656. 32. Adzemovic T, Murray T, Jenkins P, Ottosen J, Iyegha U, Raghavendran K, et al. Should they stay or should they go? Who benefits from interfacility transfer to a higher-level trauma center following initial presentation at a lower-level trauma center. J Trauma Acute Care Surg. 2019;86(6):952–960. 33. Anantha RV, Painter MD, Diaz-Garelli F, Nunn AM, Miller PR, Chang MC, et al. Undertriage despite use of geriatric-specific trauma team activation guidelines : who are we missing?Am Surg. 2021;87(3):419–426. 34. Tessler RA, Rangel MM, Rosser ML, Rivara FP, Bulger E, Vavilala MS, et al. Complications in low-risk older adult trauma patients: a case-control study. J Trauma Acute Care Surg. 2019;86(5):858–863.
留言 (0)