
記住我

Intestinal ischemia/necrosis is a disease with a high mortality rate because of the difficulty in making an early diagnosis.1,2 Physical examination and laboratory tests, such as white blood cell (WBC) count and lactate levels, are not highly specific for the diagnosis of intestinal ischemia.2–4 Reports suggest that when l-lactate levels are elevated, necrosis has likely already set in, and the mortality rate may be as high as 75%;5–7 therefore, a diagnosis is often made by combining blood tests and imaging modalities, such as computed tomography.6 Recent studies have demonstrated that serum markers such as intestinal fatty acid-binding protein (I-FABP), alpha-glutathione S transferase (α-GST), d-lactate, and smooth muscle protein of 22 kDa (SM22) can aid in the diagnosis of intestinal ischemia.8–11 However, they are not generally used clinically because of their high invasiveness, low speed, and high cost.2
Prostaglandin E2 (PGE2) is a major inflammatory mediator derived from cyclooxygenase. Its levels reflect the degree of inflammation; however, PGE2 is rapidly metabolized, making its measurement in peripheral blood difficult. Therefore, recent attention has been given to prostaglandin E2 major urinary metabolite (PGE-MUM), which is excreted in the urine. Prostaglandin E2 major urinary metabolite has good stability in urine, and its association with certain diseases, such as ulcerative colitis (UC) and interstitial pneumonia, has been reported.12–15 However, despite some reports on the utility of PGE-MUM in the diagnosis of intestinal inflammation, the detailed mechanism by which this biomarker is involved in the disease process has not been identified.
Therefore, the present study investigated the relationship between PGE-MUM levels and the degree of intestinal ischemia in rats.
MATERIALS AND METHODS AnimalsMale Sprague-Dawley rats with body weights between 300 g and 350 g (Sankyo Labo Service Corporation, Inc., Tokyo, Japan) were used for all experiments. Animals were housed in an environment maintained at an average temperature of 22°C (±2°C), with a 12-hour light/dark cycle. They were provided standard laboratory chow and water ad libitum until just before anesthesia.
The experimental procedures adhered to the ARRIVE guidelines and the National Institutes of Health Guide for the Care and Use of Laboratory Animals. The institutional Animal Care Committee approved the protocols per institutional guidelines. The ARRIVE checklist is uploaded as Supplemental Digital Content 1 (https://links.lww.com/TA/D559).
Ischemia-Reperfusion ModelRats were divided into seven groups: four intestinal superior mesenteric artery occlusion (SMAO) groups (30-minute ischemia and 6-hute reperfusion [n = 7]; 60-minute ischemia and 3-hour reperfusion [n = 7]; 60-minute ischemia and 6-hour reperfusion [n = 7]; and 60-minute ischemia and 1-hour reperfusion [n = 7]) and three sham groups (30-minute observation and 6-hour observation [n = 7]; 60-minute observation and 3-hour observation [n = 7]; and 60-minute observation and 6-hour observation group [n = 7]). In the SMAO group, a microvascular clamp using an AM-1-30 microvascular clip (Bear Medic Corp., Ibaraki, Japan) was used to cause complete occlusion of the superior mesenteric artery (SMA) for either 30 minutes or 60 minutes to induce intestinal ischemia. The abdomen was temporarily closed using a 4-0 silk suture. The abdomen was then reopened 30 minutes or 60 minutes after SMAO, and the clamp was removed to allow reperfusion. The abdominal incision was reclosed with a 4-0 silk suture, and 45 mL/300 g normal saline and 0.05 mg/kg buprenorphine were administered via subcutaneous injections, as shown in Figure 1. The reperfusion period lasted for either 1 hour, 3 hours, or 6 hours. In the sham group, the SMA was not clamped; however, all other procedures were performed for the same duration. A segment of the small intestine (10 cm of the distal ileum) was removed, and hematoxylin and eosin (H-E) staining was performed for histological evaluation. The degree of histopathological injury was graded according to the Chiu score.16
 Figure 1:
Figure 1: Time course of the experiment. The superior mesenteric artery was clamped for 30 or 60 minutes. The reperfusion phase was either 1, 3, or 6 hours after the superior mesenteric artery was declamped. Urine samples were collected after resuscitation.
Urine and Blood CollectionUrine samples were collected via bladder puncture following reperfusion. Urine samples for urine creatinine (Cr) and PGE-MUM evaluations and the supernatants were stored at −80°C. The urine Cr level was measured to determine the effect of the PGE-MUM concentration on urine volume (urine concentration). A urine sample (90 μL) was used to analyze the urine Cr level using an enzymatic method employed by Oriental Yeast Co., Ltd., Nagahama, Shiga (outsourced data).
Blood samples were withdrawn through a catheter (1.0 × 1.5 mm silicon tube; Ebihara Rubber, Co., Ltd., Tokyo, Japan) inserted into the right internal jugular vein after reperfusion. A complete blood count (Celltacα, MEK-6400; Nihon Koden Co., Ltd., Tokyo, Japan) and blood gas analysis (ABL 800 FLEX; RADIOMETER Co., Ltd., Tokyo, Japan) were performed.
Spike Recovery Test of PGE-MUM in Rat UrineA spike recovery test was performed to evaluate the stability of PGE-MUM in rat urine. Tetranor PGEM (Tetranor Prostaglandin E Metabolite, Cayman Chemical, Ann Arbor, MI), which is a formal name for PGE-MUM, was used as the spike antigen in spike recovery. Tetranor PGEM or sample diluent was added to each of the three urine samples from two normal rats (rats A and B) at a 1 (tetranor PGEM/sample diluent):9 (urine sample) ratio by volume. Antigen-spiked (test) and non-spiked (control) samples were assayed (N = 2). Spike recovery was calculated as follows: spike recovery (%) = [(assayed level in test sample − assayed level in control sample) / (final tetranor PGEM concentration/10)] × 100.
Dilution Linearity Test of PGE-MUM in Rat UrineDilution linearity tests were performed to determine the measurement range of the PGE-MUM. Four urine samples (from normal rats [rats A and B] and SMAO rats [rats C and D]) were diluted with sample diluent to create a dilution series (2-, 4-, 8-, 16-, 32-, and 64-fold).
Measurement of PGE-MUM LevelsThe PGE-MUM level was measured by a chemiluminescence enzyme immunoassay (CLEIA) using Lumipulse Presto PGE-MUM and an automated immunoassay system, Lumipulse L2400 (Fujirebio Inc., Tokyo, Japan). In the analytical instrument, 15 μL of urine was dispensed into a sample pretreatment solution containing sodium hydroxide to convert PGE-MUM in the sample to bicyclic PGE-MUM. Antigen-bound and enzyme-labeled antibodies were added to the mixture. Bicyclic PGE-MUM on ferrite particles and bicyclic PGE-MUM in the sample solution competed to react with alkaline phosphatase-labeled anti-bicyclic PGE-MUM antibodies to form an immune complex. After washing the particles, a substrate solution was added, and luminescence was measured. The PGE-MUM concentration of a specimen was determined based on a calibration curve created by measuring the luminescence of standard PGE-MUM solutions prepared from a bicyclic PGE-MUM solution standardized based on a tetranor PGEM. Furthermore, the PGE-MUM value was corrected by the concentration of urinary Cr and expressed as PGE-MUM (μg/g Cr) because its concentration depends on the urinary volume.
Statistical AnalysesIn this study, the sample size in each experimental group of the intestinal ischemia-reperfusion (I/R) model was n = 7. Since there is no relevant literature on PGE-MUM in rats, the study was conducted with reference to previous studies on I/R models.17–19 The observed mortality rate of SMAO was 15% (5/33); SMAO (60 minutes to 6 hours), 0% (0/7); SMAO (60 minutes to 3 hours), 12.5% (1/8); SMAO (30 minutes to 6 hours), 0% (0/7); and SMAO (60 minutes to 1 hour), 36.4% (4/11).
Data are presented as the mean ± standard deviation (SD). An analysis of variance was performed with a post hoc analysis using Tukey's test among the six groups, including the three intestinal SMAO groups (a 30-minute ischemia and 6-hour reperfusion group [n = 7], a 60-minute ischemia and 3-hour reperfusion group [n = 7], and a 60-minute ischemia and 6-hour reperfusion group [n = 7]) and three sham groups (a 30-minute observation and 6-hour observation group [n = 7], a 60-minute observation and 3-hour observation group [n = 7], and a 60-minute observation and 6-hour observation group [n = 7]). Differences were considered statistically significant at p < 0.05. All statistical analyses were performed using the three software program, version 9 (GraphPad Software, San Diego, CA).
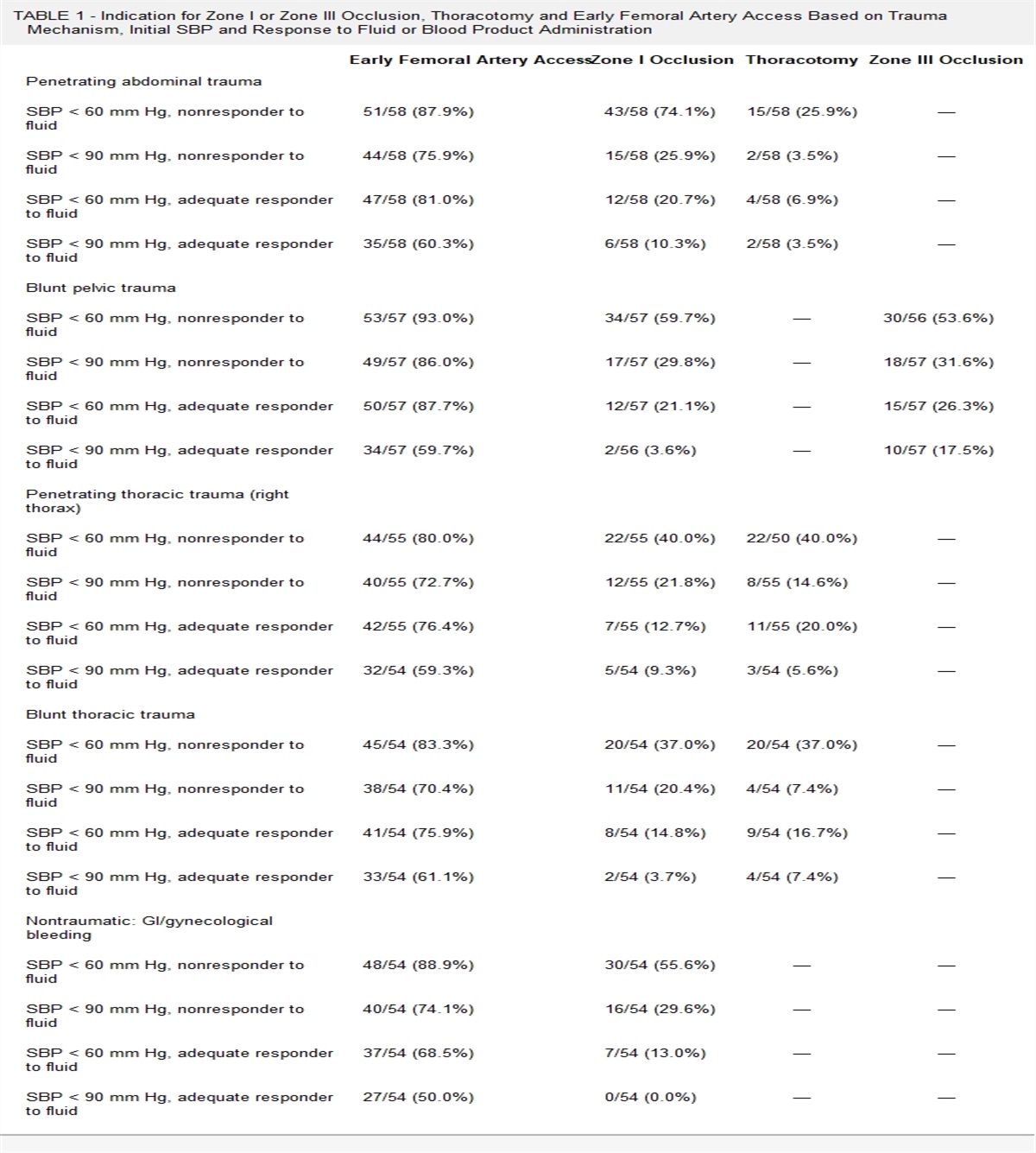
RESULTS Laboratory TestsWhite blood cells (/μL), pH, bicarbonate (HCO3) (mmol/L), base excess (BE), and lactate (mmol/L) are shown in Table 1. Although the SMAO groups tended to have higher lactate levels than the sham groups, there were no statistically significant differences. The pH, HCO3, and BE values significantly differed among the sham groups and 60-minute ischemia and 3-hour reperfusion groups, and the 60-minute ischemia and 6-hour reperfusion groups (p < 0.05).
TABLE 1 - Laboratory Tests SHAM SMAO SMAO SHAM SMAO SHAM SMAO 30 min to 6 h 30 min to 6 h 60 min to 1 h 60 min to 3 h 60 min to 3 h 60 min to 6 h 60 min to 6 h N 7 7 7 7 7 7 7 Body weight (g) 335.9 (±32.5) 322.8 (±22.3) 331.1 (±10.4) 350.7 (±45.7) 328 (±41.1) 338.6 (±12.2) 342.2 (±12.9) WBC (/μL) 4,214 (±1,661) 5,686 (±997) 5,562 (±1,794) 6,971 (±734) 6,414 (±2,195) 6,286 (±1,843) 5,300 (±1,377) pH 7.31 (±0.09) 7.26 (±0.17) 7.15 (±0.06) 7.27 (±0.09) 7.05 (±0.1)* 7.27 (±0.14) 7.02 (±0.17)* HCO3 (mmol/L) 24.4 (±1.9) 21.6 (±3.3) 20.7 (±0.5) 20.9 (±1.4) 16.4 (±3.5)* 25 (±2.1) 15.7 (±4.7)* BE −3.5 (±3.6) −5.7 (±4.2) −9.3 (±1.9) −5.9 (±1.9) −16.2 (±6.6)* −2.7 (±4.6) −17.6 (±8.9)* Lac (mmol/L) 1.9 (±0.8) 3.1 (±2.2) 2.3 (±1.0) 1.6 (±0.9) 3.2 (±2.5) 2.4 (±2.2) 3.6 (±2.6)Blood samples were obtained, and WBC, pH, HCO3, BE, and lactate levels were analyzed. Data are presented as mean (SD).
*Significant change (p < 0.05).
Tissue examinations of the sham and SMAO groups were compared. Histology grading in the SMAO group (60-minute ischemia and 6-hour reperfusion group, 4.7 ± 0.5) was significantly higher than that in the sham groups (0.4 ± 0.7). In addition, the intestinal injury score of the 60-minute ischemia and 6-hour reperfusion group was significantly higher than that in the 30-minute ischemia and 6-hour reperfusion group (1.8 ± 0.4, p < 0.05), suggesting that intestinal ischemia occurred in the SMAO group (Fig. 2). Similarly, the intestinal injury score of the 60-minute ischemia and 1-hour reperfusion group was 4.3 ± 1.0, indicating intestinal ischemia. A blinded pathologist assessed the area of ischemic changes in the stained tissue specimens and graded the degree of injury.
 Figure 2:
Figure 2: Gut histology. After the resuscitation phase, a segment of the small intestine was harvested and fixed in formalin for histopathological evaluation. Representative histological findings are shown (A). Grading was performed based on the Chiu score (B). An asterisk indicates a significant change (p < 0.05).
Stability of PGE-MUM in UrineWe conducted a stability test of PGE-MUM in rat urine. The assay range for PGE-MUM was 2.0 ng/mL to 200.0 ng/mL. Spike recovery test results were good for all three urine samples from normal rats (rats A and B), with results ranging from 86% to 97%, suggesting that PGE-MUM is stable in rat urine (Supplemental Digital Content 2, https://links.lww.com/TA/D560). All dilutions (normal rat A, normal rat B, SMAO rat C, and SMAO rat D) were within 100 ± 20% of the theoretical levels calculated based on the highest concentration entering the range, confirming the dilution linearity of the assay. These findings showed that the PGE-MUM levels in rat urine were within the measurement range (Fig. 3).
 Figure 3:
Figure 3: Dilution linearity test. Four urine samples were used to create a dilution series (2-, 4-, 8-, 16-, 32-, and 64-fold) for assaying (N = 2).
PGE-MUM In Urine After Intestinal I/R InjuryPGE-MUM levels at different ischemic times (30 minutes vs. 60 minutes) with the same reperfusion time (6 hours) were compared with investigate the effect of ischemic time on PGE-MUM levels. The PGE-MUM levels in the 30-minute ischemia group (n = 7, 483 ± 256 ng/mL) were significantly higher than those in the sham group (n = 7, 73 ± 32 ng/mL; p < 0.05). Furthermore, the PGE-MUM levels in the 60-minute ischemia group (n = 7, 889 ± 402 ng/mL; p < 0.05) were higher than that in the 30-minute ischemia group (Supplemental Digital Content 3, https://links.lww.com/TA/D561). The PGE-MUM/urine Cr levels in the SMAO group (30-minute ischemia and 6-hour reperfusion group, 8.3 ± 4.2 μg/g·Cr; 60-minute ischemia and 6-hour reperfusion group, 15.6 ± 6.5 μg/g·Cr) were significantly higher than in the sham group (30-minute and 6-hour reperfusion group, 1.9 ± 0.4 μg/g·Cr, and 60-minute and 6-hour reperfusion group, 2.1 ± 0.8 μg/g·Cr, p < 0.05) (Fig. 4A). These findings suggest that PGE-MUM levels are associated with the duration of intestinal ischemia. We then compared the PGE-MUM levels at different reperfusion times (3 hours vs. 6 hours) with the same ischemic time (60 minutes) to investigate the effect of reperfusion time on PGE-MUM levels. In the SMAO group, the PGE-MUM level in the 3-hour reperfusion group (1401 ± 760 ng/mL) was significantly higher than that in the 6-hour reperfusion group (889.2 ± 402 ng/mL, p < 0.05) (Supplemental Digital Content 3, https://links.lww.com/TA/D561). The PGE-MUM/urine Cr level in the SMAO group 3-hour reperfusion group (20.7 ± 8.9 μg/g·Cr) was significantly higher than in the 6-hour reperfusion group (15.6 ± 6.5 μg/g·Cr, p < 0.05) (Fig. 4B). These findings indicate that PGE-MUM can be used as a marker of intestinal ischemia 3 hours after an ischemic event. In the 60-minute ischemia and 1-hour reperfusion group, the PGE-MUM/urine Cr level was 9.0 ± 1.8 μg/g-Cr, indicating that PGE-MUM may peak after 1 hour of reperfusion, most likely at 3 hours.
 Figure 4:
Figure 4: Effects of the duration of ischemia and duration of reperfusion on PGE-MUM/urine Cr levels. The SMA was clamped for 30 or 60 minutes to induce intestinal ischemia. The reperfusion phase lasted for 6 hours. Urine samples were collected after reperfusion. PGE-MUM levels were measured using a CLEIA. The PGE-MUM value was corrected by the urinary Cr concentration and expressed as PGE-MUM/urine Cr because its concentration depends on the urinary volume (A). Asterisks indicate p < 0.05. In the sham group, all procedures were identical, without SMA clamping. The SMA was clamped for 60 minutes to induce intestinal ischemia. The reperfusion phase lasted either 1, 3, or 6 hours. Urine samples were collected after reperfusion. The PGE-MUM value was corrected by the urinary Cr concentration and expressed as PGE-MUM/urine Cr because its concentration depends on the urinary volume (B). Asterisks indicate p < 0.05. In the sham group, all procedures were identical, without SMA clamping.
DISCUSSIONOur study showed that intestinal ischemia is associated with PGE-MUM levels when studied using a rat intestinal ischemia model. Although most reports on PGE-MUM are based on human data,8,12–15,20–25 studies to determine the validity of PGE-MUM measurements in rodents after the induction of intestinal ischemia/necrosis are lacking. In the current study, we demonstrated the validity of the PGE-MUM test in rat samples using dilution linearity testing. These results may prove useful in future PGE-MUM research.
Prostaglandin E2 is a major inflammatory mediator. When a biological stressor is present, arachidonic acid is generated from the phospholipids of the cell membrane by phospholipase A2. Arachidonic acid is converted to PGE2 by cyclooxygenase and PGE2 synthase.26 However, since PGE2 is metabolized in the blood within a few seconds, its measurement is generally difficult. Its metabolites are oxidized in the liver and kidneys and excreted in the urine. Urine is the main excretion route of PGE2, and it is considered a stable substance, similar to PGE-MUM. This stability is essential for the widespread use of these tests. In addition to its stability, the non-invasiveness of assessing PGE-MUM adds to its utility. There is no need for blood or pathological tissue examinations; a urine test alone is sufficient. The test using a urine sample takes approximately 30 minutes, making it very convenient. Its simplicity can also be considered an advantage.12
PGE2 levels increase in cases of intestinal ischemia.27 When ischemia occurs, PGE2 is produced via the arachidonic acid cascade. When PGE2 is produced, metabolites are thought to be excreted in the urine.28 Because of these features, PGE-MUM is already a biomarker applied clinically in humans for UC.12–14,20–22 Previous reports have suggested a correlation between PGE-MUM elevation and UC through a mechanism that involves an increase in PGE2. Therefore, the utility of PGE-MUM is also suggested in conditions related to the COX-2 enzyme, such as lung adenocarcinoma, interstitial pneumonia, and mesenteric adipose inflammation.23–25
In the present study, the SMAO group showed higher PGE-MUM levels than the sham group. Furthermore, even when the duration of reperfusion was the same, the duration of ischemia correlated with higher PGE-MUM levels, suggesting a potential correlation between the degree of intestinal ischemia and PGE-MUM levels independent of reperfusion. Furthermore, given the same duration of ischemia, PGE-MUM levels were higher when the reperfusion time was 3 hours (comparing 1 hour and 6 hours), suggesting the potential utility of PGE-MUM as a reliable marker of intestinal ischemia 3 hours after an ischemic event.
Laboratory test values such as lactate, liver enzymes, C-reactive protein, and lymphocytes, among others, have been investigated to identify markers of intestinal ischemia/necrosis.3–6,29,30 Although markers of intestinal ischemia such as i-FABP, d-lactate, and SM22 have been recently reported,2,8–11 their clinical application has not gained widespread acceptance. Because of its simplicity, PGE-MUM measurements can be easily applied to the assessment of intestinal ischemia as it is already being used clinically in patients with UC.
However, there are several issues associated with the use of PGE-MUM. First, it may be affected by drugs, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and sennosides, which affect PGE production.21,28,31 Therefore, these drug interactions require attention. For example, elderly patients taking NSAIDs may show a false-negative result for PGE-MUM, while those taking sennosides may show a false-positive result. Sennosides are thought to induce PGE production.21 The second issue is its low specificity. As PGE-MUM operates through a PGE2-related mechanism, it may increase in response to other biological stresses. Prostaglandin E2 is metabolized by the PG-degrading enzyme 15-HPGD, produced in the lungs. Therefore, if there is lung dysfunction, PGE metabolism may be disrupted, affecting PGE-MUM production. Indeed, in respiratory diseases, PGE-MUM is used not for the diagnosis but to monitor disease progression. The same potential exists for intestinal ischemia. Therefore, in the future, it will be necessary to consider these factors when applying this method clinically.
LimitationsSeveral limitations associated with the present study warrant mention. First, a few samples were analyzed because of the limited number of animals used in the experiments. Second, the results may have been influenced by the sex of the animals, collection time, and age. It has been reported that PGE-MUM levels are higher in males than in females and change with age. Female-specific hormones, such as estrogen, may influence PGE-MUM levels. Prostaglandin E2 major urinary metabolite levels also vary depending on the time of day.32 Third, the PGE2 level in urine would be expected to increase during the mesenteric ischemia phase. However, we could not collect enough urine samples to measure PGE-MUM levels during this phase. Fourth, we did not evaluate the correlation with I-FABP, α-GST, d-lactate, and SM22 with PGE-MUM levels, which are already considered markers of intestinal ischemia. Fifth, acute mesenteric ischemia might lead to AKI. In our study, the serum Cr level was not elevated in the SMAO model, and therefore, it seems that renal dysfunction/failure was not an issue in our experiments. Future studies are required to confirm our current findings.
CONCLUSIONThis study showed that PGE-MUM levels increase with the degree of intestinal ischemia. Despite the differences between rats and humans, the increase in PGE-MUM levels caused by ischemia shown in this study was extremely high compared with previous human studies. Therefore, if intestinal ischemia is suspected, high levels of PGE-MUM may be a reliable diagnostic marker. Additional studies are needed to confirm the clinical application of these findings in humans.
AUTHORSHIPK.S., T.A., P.T., and A.S. performed the experiments and collected the samples. K.S., K.M., T.A., A.S., K.Y., K.N., and M.A. performed the data collection and analysis. K.S., K.M., and R.C. conceived the study and participated in its design and coordination. K.S., K.M., M.K., R.C., and Y.O. drafted the article. All authors approved the final version of the article.
ACKNOWLEDGMENTWe thank Fujirebio, Inc. (Yuki Yonezawa, Hidekazu Nasu, Tomonao Ouki) for measuring PGE-MUM. The icons from the Noun Project (https://thenounproject.com and https://iconfinder.com) were used for the Visual abstract. This work was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (no. 22K09135; K.M.) and Public Trust Foundation of Marumo ER Medicine & Research Institute (K.S.). The funding source played no role in the study design, collection, analysis, or interpretation of data, in the writing of the report, or the decision to submit the article for publication.
DISCLOSUREConflicts of Interest: Author Disclosure forms have been supplied and are provided as Supplemental Digital Content (https://links.lww.com/TA/D562).
REFERENCES 1. Bala M, Kashuk J, Moore EE, Kluger Y, Biffl W, Gomes CA, et al. Acute mesenteric ischemia: guidelines of the World Society of Emergency Surgery. World J Emerg Surg. 2017;12:38. 2. Tilsed JVT, Casamassima A, Kurihara H, Mariani D, Martinez I, Pereira J, et al. ESTES guidelines: acute mesenteric ischaemia. Eur J Trauma Emerg Surg. 2016;42(2):253–270. 3. van den Heijkant TC, Aerts BA, Teijink JA, Buurman WA, Luyer MD. Challenges in diagnosing mesenteric ischemia. World J Gastroenterol. 2013;19(9):1338–1341. 4. Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD. Acute mesenteric ischemia: a clinical review. Arch Intern Med. 2004;164(10):1054–1062. 5. Nuzzo A, Maggiori L, Ronot M, Becq A, Plessier A, Gault N, et al. Predictive factors of intestinal necrosis in acute mesenteric ischemia: prospective study from an intestinal stroke center. Am J Gastroenterol. 2017;112(4):597–605. 6. Clair DG, Beach JM. Mesenteric ischemia. N Engl J Med. 2016;374(10):959–968. 7. Hmoud B, Singal AK, Kamath PS. Mesenteric venous thrombosis. J Clin Exp Hepatol. 2014;4(3):257–263. 8. Matsumoto S, Sekine K, Funaoka H, Yamazaki M, Shimizu M, Hayashida K, et al. Diagnostic performance of plasma biomarkers in patients with acute intestinal ischaemia. Br J Surg. 2014;101(3):232–238. 9. Treskes N, Persoon AM, van Zanten ARH. Diagnostic accuracy of novel serological biomarkers to detect acute mesenteric ischemia: a systematic review and meta-analysis. Intern Emerg Med. 2017;12(6):821–836. 10. Schellekens DHSM, Reisinger KW, Lenaerts K, Hadfoune M, Olde Damink SW, Buurman WA, et al. SM22 a plasma biomarker for human transmural intestinal ischemia. Ann Surg. 2018;268(1):120–126. 11. Derikx JPM, Schellekens DHSM, Acosta S. Serological markers for human intestinal ischemia: a systematic review. Best Pract Res Clin Gastroenterol. 2017;31(1):69–74. 12. Arai Y, Arihiro S, Matsuura T, Kato T, Matsuoka M, Saruta M, et al. Prostaglandin E-major urinary metabolite as a reliable surrogate marker for mucosal inflammation in ulcerative colitis. Inflamm Bowel Dis. 2014;20(7):1208–1216. 13. Arai Y, Matsuura T, Matsuura M, Fujiwara M, Okayasu I, Ito S, et al. Prostaglandin E-major urinary metabolite as a biomarker for inflammation in ulcerative colitis: prostaglandins revisited. Digestion. 2016;93(1):32–39. 14. Sakurai T, Akita Y, Miyashita H, Miyazaki R, Maruyama Y, Saito T, et al. Prostaglandin E-major urinary metabolite diagnoses mucosal healing in patients with ulcerative colitis in remission phase. J Gastroenterol Hepatol. 2022;37(5):847–854. 15. Ishida N, Sugiura K, Miyazu T, Tamura S, Suzuki S, Tani S, et al. Prostaglandin E-major urinary metabolite predicts relapse in patients with ulcerative colitis in clinical remission. Clin Transl Gastroenterol. 2020;11(12):e00289. 16. Chiu CJ, McArdle AH, Brown R, Scott HJ, Gurd FN. Intestinal mucosal lesion in low-flow states. I. A morphological, hemodynamic, and metabolic reappraisal. Arch Surg. 1970;101(4):478–483. 17. da Costa Rocha B, da Silva Mendes RR, Lima GV, de Souza Albuquerque G, Araújo LL, da Silva de Jesus MN, et al. Experimental model of mesenteric ischemia: reperfusion by abdominal aorta clamping in Wistar rats. Rev Col Bras Cir. 2012;39(3):207–210. 18. Ballabeni V, Barocelli E, Bertoni S, Impicciatore M. Alterations of intestinal motor responsiveness in a model of mild mesenteric ischemia/reperfusion in rats. Life Sci. 2002;71(17):2025–2035. 19. Montero EFS, Abrahão MS, Koike MK, Manna MCB, Ramalho CEB. Intestinal ischemia and reperfusion injury in growing rats: hypothermia and N-acetylcysteine modulation. Microsurgery. 2003;23(5):517–521. 20. Ishida N, Matsuura T, Asai Y, Miyazu T, Tamura S, Tani S, et al. Predicting ulcerative colitis relapse in clinical remission with fecal immunochemical occult blood test or prostaglandin E-major urinary metabolite. Clin Transl Gastroenterol. 2022;13(7):e00501. 21. Fujiwara M, Okayasu I, Oritsu M, Komatsu J, Yoshitsugu M, Katoh Y, et al. Significant increase in prostaglandin E-main urinary metabolite by laxative administration: comparison with ulcerative colitis. Digestion. 2000;61(3):201–206. 22. Hagiwara S-I, Abe N, Hosoi K, Hara T, Ishige T, Shimizu H, et al. Utility of a rapid assay for prostaglandin E-major urinary metabolite as a biomarker in pediatric ulcerative colitis. Sci Rep. 2023;13(1):9898. 23. Kawamoto H, Hara H, Araya J, Ichikawa A, Fujita Y, Utsumi H, et al. Prostaglandin E-major urinary metabolite (PGE-MUM) as a tumor marker for lung adenocarcinoma. Cancers (Basel). 2019;11:768. 24. Horikiri T, Hara H, Saito N, Araya J, Takasaka N, Utsumi H, et al. Increased levels of prostaglandin E-major urinary metabolite (PGE-MUM) in chronic fibrosing interstitial pneumonia. Respir Med. 2017;122:43–50. 25. Mikubo M, Satoh Y, Ono M, Sonoda D, Hayashi S, Naito M, et al. Prognostic implications of prostaglandin E-major urinary metabolite in resected non-small-cell lung cancer. Interdiscip Cardiovasc Thorac Surg. 2023;36:ivac291. 26. Park JY, Pillinger MH, Abramson SB. Prostaglandin E2 synthesis and secretion: the role of PGE2 synthases. Clin Immunol. 2006;119(3):229–240. 27. Sparkes BL, Slone EEA, Roth M, Welti R, Fleming SD. Intestinal lipid alterations occur prior to antibody-induced prostaglandin E2 production in a mouse model of ischemia/reperfusion. Biochim Biophys Acta. 2010;1801(4):517–525. 28. Matsuda K, Yamazaki M. Urinary excretion of prostaglandin in rats: effect of non-steroidal anti-inflammatory drugs. J Inflamm. 1980;1:111–113. 29. Chen B, Cao J, Yan C, Zheng C, Chen J, Guo C. A promising new predictive factor for detecting bowel resection in childhood intussusception: the lymphocyte-C-reactive protein ratio. BMC Pediatr. 2021;21(1):577. 30. Woodford EP, Woodford HM, Hort AR, Pang TC, Lam VWT, Nahm CB. Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio use in detecting bowel ischaemia in adhesional small bowel obstruction. ANZ J Surg. 2022;92(11):2915–2920. 31. Murphey LJ, Williams MK, Sanchez SC, Byrne LM, Csiki I, Oates JA, et al. Quantification of the major urinary metabolite of PGE2 by a liquid chromatographic/mass spectrometric assay: determination of cyclooxygenase-specific PGE2 synthesis in healthy humans and those with lung cancer. Anal Biochem. 2004;334(2):266–275. 32. Okayasu I, Ohnishi H, Sarandi I, Shojima J, Komatsu J, Oritsu M, et al. Significant increase of prostaglandin E-major urinary metabolite in male smokers: a screening study of age and gender differences using a simple radioimmunoassay. J Clin Lab Anal. 2014;28(1):32–41.
留言 (0)