
記住我

Concomitant major extremity fractures and truncal injuries have received special emphasis in the management of multiply injured patients.1,2 Over the last three decades, the indications for fracture fixation have become more data driven and associated with endpoints of resuscitation.3 These changes occurred in parallel with changes in intravascular volume replacement,4 more careful mechanical ventilation techniques, and assessment strategies that respect the patient condition more precisely (e.g., serial lactate levels than just admission value, implementation of resuscitation protocols5); similar protocols were used for treatment options in the intensive care unit (ICU).6,7
To assess and validate the patient's clinical risk profile, the Injury Severity Score (ISS)8 and laboratory parameters have been used. Lactate values on admission are part of the standard workup of any critically ill patient.9 More recently, the lactate clearance within 24 hours after admission is of value for patients with a variety of injury conditions including, but not limited to, multiple injuries and hemorrhagic shock.10,11 The initial ISS is inaccurate and does not add to the initial risk prediction or to the ideal management sequence of a patient.12 Eventually, a combination of injury burden, physical signs (vital signs, temperature), and laboratory values (lactate, arterial blood gases, and coagulation parameters) used to monitor the adequacy of resuscitation becomes a better predictor of risk and outcomes than each one.2,13 For example, the use of this strategy for risk determination has been applied to multiple-injury patients to determine if a patient is cleared to go to the operating room for early fixation of major fractures.14 Data suggest that this comprehensive assessment results in minimal complication rates and improved patient safety (safe definitive surgery [SDS]).15 However, it remains unclear if different injury patterns affect risk prediction in multiple-injury patients.
Therefore, the goal of this study is to test well-known parameters that are recommended to define the clinical status of the multiple-injury patients and a possible association with certain surgical treatment strategies in the management of multiple-injury patients.
Therefore, we hypothesized that injury distribution is associated with a certain surgical approach and that the mortality rate is independent of the surgical strategy and timing applied in the management of multiply injured patients with major fractures.
PATIENTS AND METHODSThe study protocol of this retrospective cohort study was approved by the local institutional review board (number 2020-00703). The reporting of our results was performed according to the STrengthening the Reporting of OBservational studies in Epidemiology criteria.16 The STrengthening the Reporting of OBservational studies in Epidemiology checklist is included as Supplemental Digital Content (Supplementary Data 1, https://links.lww.com/TA/D528).
This study was performed at an academic Level I trauma center, where eligible patients were included after the implementation of a new protocol for early surgical management of major truncal and extremity fractures, as previously described.15
DefinitionsMajor surgeries were defined for both, fractures and truncal injuries, as we aimed to achieve a complete image of the trauma-induced load to the human body,17 regardless of the surgical subspecialty involved. Therefore, the following minor interventions were excluded: for general trauma, these included insertion of a chest tube or suturing a minor external injury; for orthopedics, this included fixation of ankle fractures or plating of a wrist fracture. This is accordance with the revised Abbreviated Injury Scale (AIS) (AIS 2015).
The treatment strategy was determined according to the timing of surgical interventions. Timing of surgery was calculated as the time between emergency department admission and the beginning of surgery (skin incision), as documented in the operative report. Patients were stratified into three groups: damage-control (DC) surgery, early total care (ETC), and SDS.
Damage-control surgery included temporal surgical intervention, such as external fixation of fractures, temporary measures to control hemorrhage of a solid organ (e.g., packing), or resection of hollow visceral organs without simultaneous anastomosis.3
Early total care included definitive surgical intervention of major fractures and axial injuries (e.g., abdomen, spine, pelvis/acetabulum) within 24 hours of admission for orthopedic injuries. For truncal injuries, it included definitive surgery of injuries of abdominal organs (e.g., suture of hollow visceral organs, stoma installation with primary anastomosis). Patients who had a definitive surgical intervention (e.g., splenectomy, stoma, resection with anastomosis, nail or plate fracture fixation) where included in the group ETC. This did not include that the wound was closed in every situation (e.g., open abdomen, open wound therapy, negative pressure wound treatment after fasciotomy)
Safe definitive surgery included definitive surgical intervention of one or more major injuries within 48 hours of admission.
Inclusion CriteriaPatients were included when they were primarily admitted, had an ISS of ≥16, and needed surgical intervention following blunt trauma. Of note, abdominal and thoracic injuries were also included as major surgeries, if they required an operation.
This was performed, because previous studies showed that these injuries also contribute to the impact (bleeding, soft tissue injuries etc.) caused by the initial injury.13
Exclusion CriteriaPatients with penetrating injuries and secondary transfers and those with an incomplete data sets were excluded.
Variables of InterestVariables that might be associated with the determination of the treatment strategy include measures of injury distribution and injury severity, such as ISS and AIS.18–20 In addition, we tested measures of the pathophysiologic response to the injuries on admission that represent hemorrhagic shock, coagulopathy, and temperature.13 Injury Severity Score and AIS were calculated by professionally trained study nurses following local and international guidelines for the quantification of injury severity and injury distribution.21 Variables indicative of hemorrhagic shock and acid base changes included systolic blood pressure and lactate values on admission. Coagulopathy was determined by viscoelastic analyses, fibrinogen, and the international normalized ratio values. Soft tissue injuries included brain injury, chest trauma, and abdominal trauma.12
Each variable was automatically retrieved from the electronic patient medical record. These variables were used to determine unexpected outcome changes and to assess patients as stable, borderline, unstable, and in extremis,12 as discussed in the literature.2 The association of these parameters with the selected treatment strategy was analyzed by multivariate regression analyses.
Outcome MeasuresThe primary outcome measure was in-hospital mortality rate.
The secondary outcome measures were ICU stay, hospital length of stay (LOS), and the association between physiological parameters listed previously and the choice of the surgical treatment strategy.
Minimization of risk of bias includes the utilization of maximum available data sets and the usage of multivariate logistic regression analysis. To minimize selection bias, the secondary outcome measures were analyzed in survivors only.
Statistical AnalysisContinuous variables are presented as mean and SD, while categorical variables are presented as count and percentage. Nonnormal distributed parameters, as visually detected by a histogram, are presented as median and interquartile range. Statistical significance was set at an α of 0.05. Group comparisons of continuous variables were performed using analysis of variance for continuous variables and Pearson χ2 for categorical variables. The sample size analysis with mortality being the primary outcome revealed a power of more than 88% (Fisher's exact test).
The prediction model includes multivariate generalized linear mixed-model analysis. Univariate analysis of demographic data was performed (p < 0.1). If these were different, they were included in the multivariate analysis. Furthermore, variables included in the multivariate analyses were chosen as they are discussed in the literature and routinely used as part of the initial assessment of the patient.14 The results of the prediction model are presented as odds ratios (ORs) and 95% confidence intervals (CIs). The significance level was set at an α of 0.05. All analyses were performed using R (R Core Team [2022]; R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/).
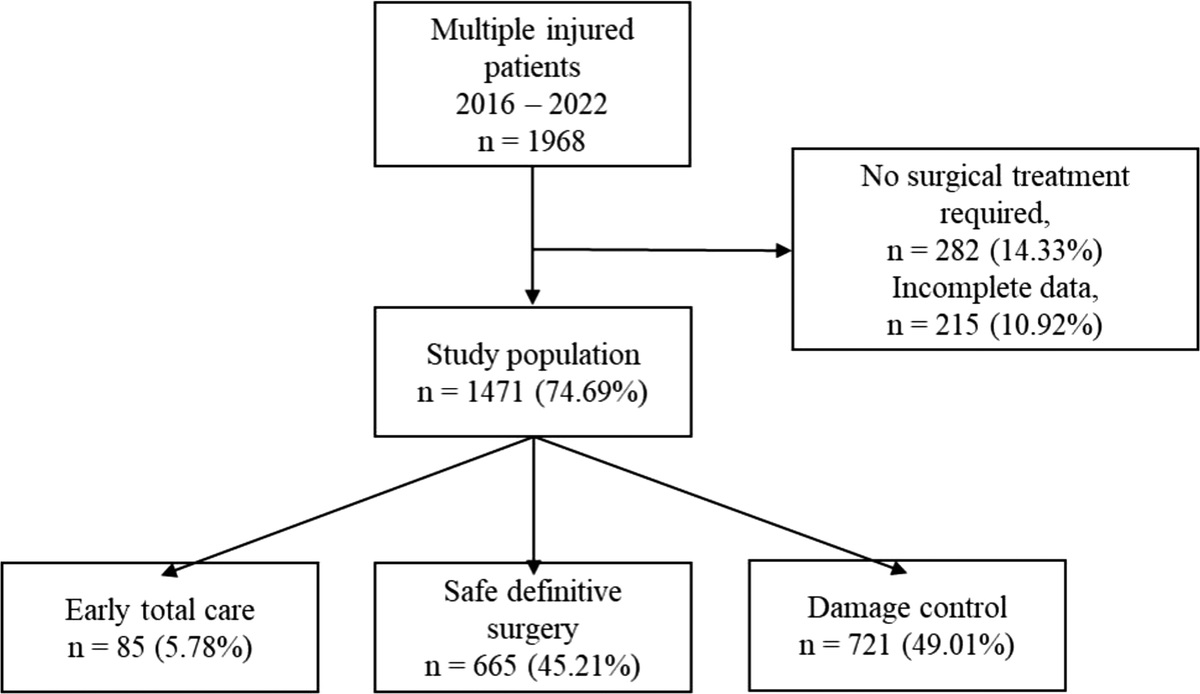
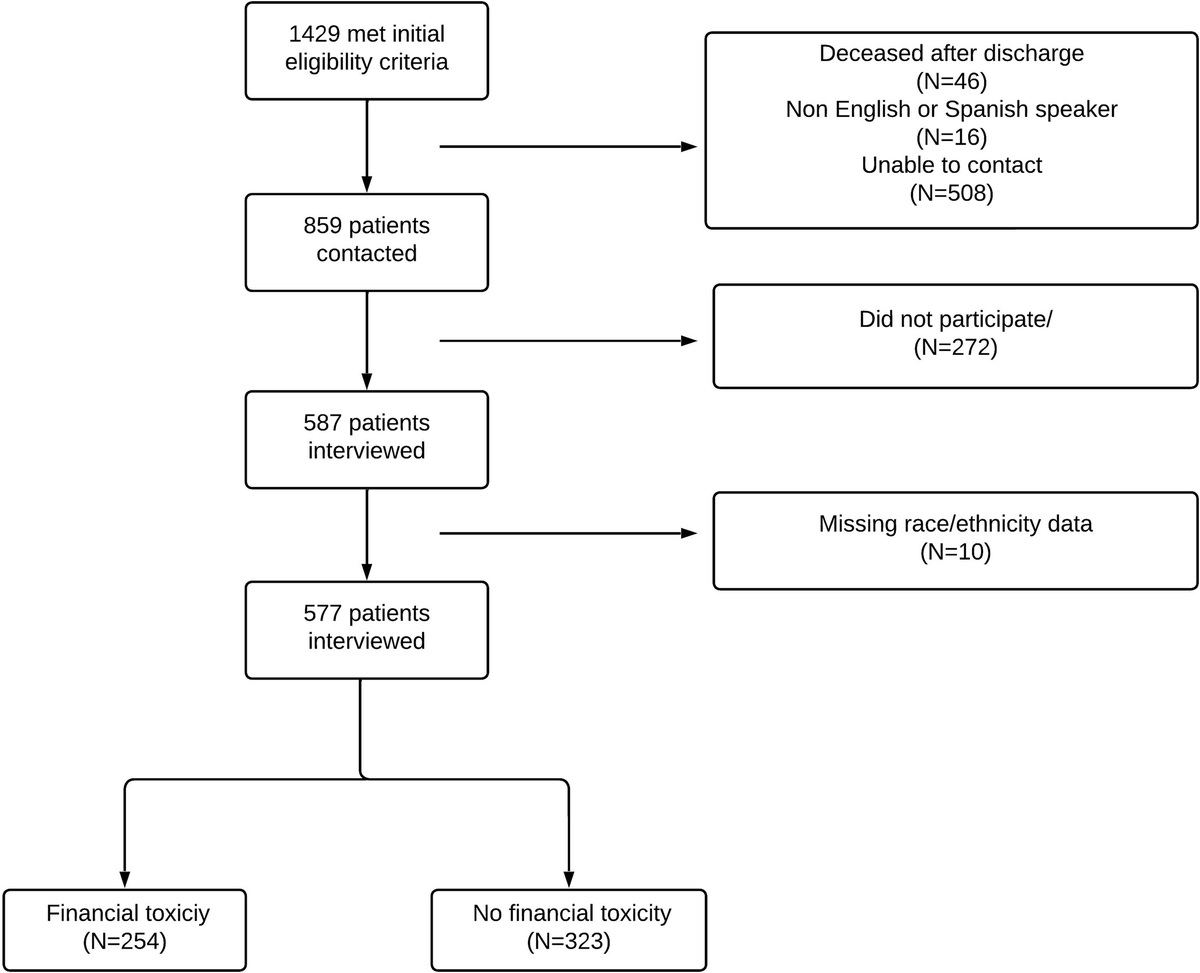
RESULTS Patient DemographicsBetween January 1, 2016, and December 31, 2022, of 1,968 eligible patients, 1,471 patients (74.7%) were included in this analysis. There were 85 patients (5.8%) in the ETC group, 665 (45.2%) in the SDS group, and 721 (49.0%) in the DC group (Fig. 1). Patients were 55.6 ± 20 years old, and the mean ± SD ISS was 23 ± 11. The overall mortality rate was 28.0% (Table 1). The distribution and severity of injuries are presented in Supplemental Digital Content (Supplementary Data 1, https://links.lww.com/TA/D529).
 Figure 1:
Figure 1: Flow chart of patient inclusion.
TABLE 1 - Demographics of Study Population n 1,471 Age, mean (SD), y 55.60 (20.38) Male sex, n (%) 986 (67.0) Mechanism of injury Penetrating trauma (Excluded) Blunt trauma 1,471 (100%) Motor vehicle injury, n (%) 512 (34.8) Sports injury, n (%) 360 (24.5) Assault or suicide, n (%) 66 (4.49) Injury during work, n (%) 112 (7.6) Injury at home, n (%) 287 (19.5) Unknown, n (%) 79 (5.4) Falls, n (%) 726 (49.32) <2 m 378 (52.07) <5 m 241 (33.20) <10 m 73 (10.06) Above 10 m 34 (4.68) Mortality, n (%) 412 (28.0) Death within 24 h, n (%) 93 (6.33) Death within 72 h, n (%) 129 (8.76) Death after 72 h, n (%) 190 (12.9) LOS ICU, mean (SD), d 4.91 (6.98) Duration of ventilation, mean (SD), h 51.12 (109.66) LOS, mean (SD), d 13.40 (13.98) ISS, mean (SD), points 23.05 (11.37)The highest ISS was found in group SDS (24.7 ± 11), when compared with ETC (20.0 ± 14; p < 0.001) and DC (21.9 ± 11.5; p < 0.001). Early total care patients sustained more severe abdominal injuries in comparison with group SDS and DC (p < 0.05). In addition, in group ETC, more severe spinal injuries were found in comparison with the SDS and the DC groups (p < 0.01). Patients in group SDS presented with more severe extremity injuries, while group DC presented with more severe head injuries when compared with the ETC and SDS groups (p < 0.001) (Table 2).
TABLE 2 - Demographic Stratified According to Treatment Strategy ETC SDS DC ETC vs. SDS, p ETC vs. DC, p SDS vs. DC, p p n (%) 85 665 721 Age, mean (SD), y 54.65 (20.95) 50.20 (19.44) 60.70 (19.88) 0.049 0.008 <0.001 <0.001 Male sex, n (%) 61 (71.8) 473 (71.1) 452 (62.7) 1 0.127 0.001 0.002 Mortality n (%) 19 (22.4) 107 (16.1) 286 (39.7) 0.194 0.003 <0.001 <0.001 AIS head, mean (SD), points 1.88 (0.85) 2.16 (1.12) 2.65 (1.33) 0.065 <0.001 <0.001 <0.001 AIS face, mean (SD), points 1.40 (0.50) 1.31 (0.57) 1.34 (0.58) 0.415 0.597 0.51 0.631 AIS neck, mean (SD), points 1.20 (0.45) 1.64 (0.99) 1.73 (1.03) 0.338 0.279 0.77 0.555 AIS thorax, mean (SD), points 2.47 (0.88) 2.47 (0.91) 2.54 (1.06) 0.985 0.71 0.328 0.61 AIS abdomen, mean (SD), points 2.70 (1.13) 2.19 (1.07) 2.05 (0.94) 0.043 0.007 0.252 0.037 AIS spine, mean (SD), points 2.88 (1.21) 2.46 (0.87) 2.27 (0.62) 0.016 <0.001 0.023 0.001 AIS upper extremity, mean (SD), points 1.52 (0.51) 1.76 (0.55) 1.39 (0.53) 0.012 0.212 <0.001 <0.001 AIS lower extremity, mean (SD), points 2.09 (1.17) 1.90 (0.90) 1.52 (0.80) 0.181 <0.001 <0.001 <0.001 ISS, mean (SD), points 19.98 (13.76) 24.67 (10.62) 21.92 (11.54) <0.001 0.15 <0.001 <0.001The subgroup analysis of survivors revealed increased ICU LOS in the DC group when compared with the ETC and SDS groups (p < 0.001). A longer hospital LOS was also observed in the DC group when compared with the ETC and SDS groups (p < 0.001) (Table 3).
TABLE 3 - In Hospital Course of Surviving Patients Stratified According to Treatment Strategy ETC SDS DC p n 66 558 435 ICU LOS, median (IQR), d 1.00 (0.66–1.83) 1.67 (0.83–3.70) 3.46 (1.42–7.71) <0.001 In-hospital LOS, median (IQR), d 7.00 (3.00–12.00) 9.00 (5.00–17.50) 16.00 (11.00–24.75) <0.001IQR, interquartile range.
There was a significant association between ETC and increased AIS abdomen, and with increased AIS spine. The association of ETC and the severity of abdominal injury increased after the inclusion of the admission lactate values, and it increased even more when additional pathophysiologic parameters (hemoglobin, fibrinogen, and temperature) were added (Table 4).
TABLE 4 - Sensitivity to Be Treated in a Surgical Category by AIS (Univariate) Versus AIS Plus Pathophysiologic Parameters (Multivariate Analysis Including Admission Values of Lactate, Hemoglobin, Temperature, Fibrinogen) OR (95% CI) OR (95% CI) OR (95% CI) (AIS) Univariate (AIS + Lactate) (AIS + Pathophysiology) ETC AIS abdomen 1.6 (1.1–2.38)* 1.76 (1.16–2.68)** 2.2 (1.39–3.49)† AIS spine 1.64 (1.21–2.24)** 1.57 (1.02–2.4)* 1.61 (1.2–2.2)† SDS AIS upper extremity 1.83 (1.06–2.89)* 2.11 (1.53–2.92) ** 2.45 (1.81–3.30)† AIS lower extremity 1.52 (1.11–2.14)* 1.63 (1.34–1.96)** 1.73 (1.38–2.17)† DC AIS head 1.4 (1.34–1.51)† 1.03 (0.97–1.09) 1.25 (1.12–1.39)†*p < 0.05.
**p < 0.01.
†p < 0.001.
The association of major fractures with SDS increased after the inclusion of admission lactate value. This association increased even more when additional pathophysiologic parameters (hemoglobin, fibrinogen, and temperature) were included (OR, 1.73; 95% CI, 1.38–2.17).
Patients undergoing DC had an increased AIS head. The inclusion of additional pathophysiologic parameters decreased the association between DC and head injury (OR, 1.25; 95% CI, 1.12–1.39).
Thereby, in comparison with elevated lactate alone, the addition of different pathophysiologic parameters (hemoglobin, fibrinogen, and temperature) improved the association between injury type and the treatment strategy compared with lactate alone (Table 4).
Late Complications and Risk Reduction of In-hospital MortalityWe compared the predictive ability of the treatment strategy in terms of its association with late complications. In the univariate analysis, patients in groups DC and ETC had an increased risk of pneumonia (OR, 1.6; 95% CI, 1.1–2.5 [p = 0.032]; OR, 1.3; 95% CI, 0.4–3.3 [p = 0.65], respectively) in comparison with group SDS (OR, 0.6; 95% CI, 0.4–0.9; p = 0.021).
Table 5 lists the results of the univariate analysis, where patients in the ETC and SDS groups had lower mortality rate when compared with the DC group (Table 5). In the multivariate analysis, SDS was associated with a 26% lower mortality after controlling for injury distribution, injury severity, and the initial pathophysiologic response to injury when compared with the DC group (Table 5).
TABLE 5 - Prediction of Mortality Treatment Strategy (Univariate) Versus Multivariate Univariate Including Only AIS Including Only Pathophysiology Including AIS and Pathophysiology OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI) DC Reference Reference Reference Reference ETC 0.44 (0.25–0.74)* NA 1.06 0.53 (0.29–0.97)** SDS 0.29 (0.23–0.38)* 0.44 (0.11–1.76) 0.58 (0.03–0.1)† 0.26 (0.18–0.36)*Abbreviated Injury Scale includes AIS 1, AIS 5, AIS 6, AIS 7, and AIS 8. Pathophysiology includes admission lactate, hemoglobin, fibrinogen, and temperature.
*p < 0.001.
**p < 0.05.
†p < 0.01.
Surgical procedures in trauma patients are common in the emergency setting.22,23 Timely fracture fixation can be achieved in most trauma patients, and it represents an important factor in achieving an uneventful clinical course. Therefore, the process of clearing multiple-injury patients for surgery has become highly important.12,24,25 Recent resuscitation guidelines are likely associated with a reduction in general complication rates, even when many of the injuries are considered life-threatening.26 In general, isolated orthopedic injuries (pelvic, spinal, extremity) are usually not acutely life-threatening, and therefore, the acute management of such injuries may not be a priority. In addition, these injuries may be influenced by hospital resource availability.27,28
Truncal and musculoskeletal injuries have been investigated as separate entities in most studies.12,29–31 To address this issue, the present investigation includes all surgical procedures and management strategies, performed by both general and orthopedic trauma surgeons in the same patients. We feel that this approach might provide new insights, as it looks at the clinical course from a patient perspective. Our main findings include the following;
Abdominal and spinal injuries appear to be associated with an ETC approach. In the presence of severe head injury, surgical interventions were performed later, regardless of the presence of other non–life-threatening injuries. When the combination of injury distribution and admission pathophysiologic parameters was taken into consideration, major fractures were managed definitively within 48 hours after admission. All these patients were thus treated according to a SDS approach.Our results are in line with recent publications suggesting that determining the overall injury burden by adding clinical and laboratory parameters and not limited to AIS or ISS values facilitates the safe clearance of patients safely for definitive major surgery.32 To allow separation between truncal and orthopedic injuries, we discuss them as separate entities as follows:
Truncal Injuries (Abdomen and Spine)The present study showed that nonlethal abdominal injury in patients with adequate physiological status was associated with an ETC approach. These results are not surprising, since, in abdominal injuries, any delay in performing an acute intervention to control severe hemorrhage and hollow viscous injuries is known to result in increased mortality rates and significant complications. The rapid stabilization by hemorrhage control can be achieved by both, a DC approach, and in those responding to resuscitation, definitive care and open abdomen treatment can be performed.33,34 It is important to notice that this study focused on the surgical intervention independent of the type of wound closure; that is, a definitive abdominal surgical intervention that was performed within the first 24 hours of the injury was regarded as an ETC approach, independent of the type of closure (open abdomen). According to the present data, the general surgeon appears to choose an ETC approach in selected severe abdominal injuries. The value of the DC approach in life-threatening conditions is not affected by our findings. Among the examples of a successful DC approach is the fact that liver injuries, if treated operatively, were packed rather than submitted to a liver resection (data not shown). In a similar fashion, the indication for surgery in splenic injuries has changed because of the availability of endovascular procedures. This fact would also require further analysis. Of note, we had excluded the patients who succumbed to their injuries from certain analyses. Therefore, this aspect may require further and more specific study.
Severe spinal injuries appear to trigger a comparable approach by orthopedic trauma surgeons. According to our results, increased severity of spine injuries is associated with the ETC protocol for these injuries. A recent publication performed in a large scaled registry demonstrated that the severity of spinal injuries is associated with additional major injuries and that early fixation of spinal injuries represents a common practice.35 In the present study, the association between ETC approach and spine injuries becomes more sustained when pathophysiologic parameters are considered as well. This is in keeping with previous results in a different patient population.14
Traumatic Brain InjuryThe major limiting factor for timely definitive surgical interventions was traumatic brain injuries. The choice toward DC surgery was independent from the pathophysiologic response to trauma. On one hand, severe traumatic brain injury (TBI) is discussed to represent a major cause of early death in multiple injuries,36,37 while, in patients who survive the first days, the issue of severe TBI is considered less fatal. On the other hand, even in patients who survived the first 72 hours after injury, DC was the treatment of choice in multiple-injury patients with severe TBI. This finding is surprising, although the outcome of multiple-injury patients in terms of quality of life is substantially affected by severe TBI.38 For these reasons, it may be understandable that severe TBI leads to a DC approach independent of the stability of the multiple-injury patient. More specific investigations should be performed, as timely fixation of fractures is well known to have other advantages (e.g., development of heterotopic ossifications).39
Extremity InjuriesIn multiple-injury cases with major injuries to the extremities, the pathophysiologic response dictates both the timing and the outcome of these patients. The present study provides further evidence that the combination of injury distribution and clinical parameters on admission improves the prediction of the outcome in severely injured patients when compared with individual parameters.10,30 A growing body of literature has recommended the use of different pathophysiologic parameters (“holistic physiologic status”).13,40 Among those is the description of the so-called “diamond of death,” which includes acidosis, hypothermia, coagulopathy, and hypocalcemia.41 The present study showed improved prediction of outcomes when both the anatomic injury distribution and a holistic pathophysiologic approach were applied.
The predictive ability of parameters collected on admission or shortly thereafter has been investigated in multiple studies. In this line, serial lactate levels have been described to be superior to admission lactate.11 Moreover, the inclusion of additional variables such as temperature, coagulation parameters, and metabolic measurements has been associated with a substantial improvement in the accuracy to predict late complications.13 The inclusion of clinical parameters improves the prediction of scoring systems to define multiple injuries,42 the risk of acute respiratory distress syndrome after chest trauma,43 and scores attempting to grade these patients according to the overall injury burden.44 Another study showed increased specificity after adding clinical and physiological parameter to the ISS values in multiply injured patients. It is understood that physiological parameters are not the sole influence on surgical decision making, but the presence of distinct injuries also affects the surgical approach and its timing.
LimitationsOur study has several limitations. The retrospective single-institution design represents a limitation, as individual or institutional bias may occur. In addition, the documentation about the specific reasons why the surgeon chose a certain treatment strategy is limited and may have interfered with our interpretation of data. However, the predictive factors mentioned previously have been described and used in numerous studies and are used internationally in the standardized assessment of multiply injured patients.45,46
CONCLUSIONIn multiply injured patients, severe spinal fractures and certain nonlethal abdominal injuries are associated with ETC, both of which were closely related with an adequate pathophysiologic status. In contrast, severe traumatic brain injuries were strongly associated with a delay in definitive surgical interventions; this was independent of the pathophysiologic response. Multiple-injury patients with major fractures have a higher survival rate when early definitive surgery was performed and all pathophysiologic parameters were taken into consideration (SDS approach).
AUTHORSHIPS.H., R.P., and H.-C.P. contributed in the conceptualization, data curation, formal analysis, investigation, methodology, project administration, supervision, validation, visualization, writing of original draft, and review and editing of manuscript. J.D. contributed in the language editing, writing of original draft, and review and editing of manuscript. F.K.L.K., Y.K., T.B., and V.N. contributed in the validation, methodology, writing of original draft, and review and editing of manuscript.
DISCLOSUREConflicts of Interest: Author Disclosure forms have been supplied and are provided as Supplemental Digital Content (https://links.lww.com/TA/D530).
REFERENCES 1. Brasel KJ, Akason J, Weigelt JA. Dedicated operating room for trauma: a costly recommendation. J Trauma. 1998;44(5):832–836 discussion 6-8. 2. Pape HC, Halvachizadeh S, Leenen L, Velmahos GD, Buckley R, Giannoudis PV. Timing of major fracture care in polytrauma patients — an update on principles, parameters and strategies for 2020. Injury. 2019;50(10):1656–1670. 3. Pfeifer R, Kalbas Y, Coimbra R, Leenen L, Komadina R, Hildebrand F, et al. Indications and interventions of damage control orthopedic surgeries: an expert opinion survey. Eur J Trauma Emerg Surg. 2021;47(6):2081–2092. 4. Spahn DR, Bouillon B, Cerny V, Duranteau J, Filipescu D, Hunt BJ, et al. The European guideline on management of major bleeding and coagulopathy following trauma. Crit Care. 2019;23(1):1–74. 5. Stein P, Kaserer A, Sprengel K, Wanner GA, Seifert B, Theusinger OM, et al. Change of transfusion and treatment paradigm in major trauma patients. Anaesthesia. 2017;72(11):1317–1326. 6. Fawley JA, Tignanelli CJ, Werner NL, Kasotakis G, Mandell SP, Glass NE, et al. American Association for the Surgery of Trauma/American College of Surgeons Committee on trauma clinical protocol for management of acute respiratory distress syndrome and severe hypoxemia. J Trauma Acute Care Surg. 2023;95(4):592–602. 7. Michetti CP, Fakhry SM, Brasel K, Martin ND, Teicher EJ, Liu C, et al. Structure and function of a trauma intensive care unit: a report from the trauma intensive care unit prevalence project. J Trauma Acute Care Surg. 2019;86(5):783–790. 8. Butcher N, Balogh ZJ. The definition of polytrauma: the need for international consensus. Injury. 2009;40:S12–S22. 9. Dübendorfer C, Billeter AT, Seifert B, Keel M, Turina M. Serial lactate and admission SOFA scores in trauma: an analysis of predictive value in 724 patients with and without traumatic brain injury. Eur J Trauma Emerg Surg. 2013;39(1):25–34. 10. Abramson D, Scalea TM, Hitchcock R, Trooskin SZ, Henry SM, Greenspan J. Lactate clearance and survival following injury. J Trauma. 1993;35(4):584–588 discussion 8-9. 11. Dezman ZD, Comer AC, Smith GS, Narayan M, Scalea TM, Hirshon JM. Failure to clear elevated lactate predicts 24-hour mortality in trauma patients. J Trauma Acute Care Surg. 2015;79(4):580–585. 12. Pape HC, Giannoudis PV, Krettek C, Trentz O. Timing of fixation of major fractures in blunt polytrauma: role of conventional indicators in clinical decision making. J Orthop Trauma. 2005;19(8):551–562. 13. Halvachizadeh S, Baradaran L, Cinelli P, Pfeifer R, Sprengel K, Pape HC. How to detect a polytrauma patient at risk of complications: a validation and database analysis of four published scales. Plos One. 2020;15(1):e0228082. 14. Pfeifer R, Klingebiel FK, Halvachizadeh S, Kalbas Y, Pape HC. How to clear Polytrauma patients for fracture fixation: results of a systematic review of the literature. Injury. 2023;54(2):292–317. 15. Pape HC, Andruszkow H, Pfeifer R, Hildebrand F, Barkatali BM. Options and hazards of the early appropriate care protocol for trauma patients with major fractures: towards safe definitive surgery. Injury. 2016;47(4):787–791. 16. Skrivankova VW, Richmond RC, Woolf BAR, Davies NM, Swanson SA, VanderWeele TJ, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomisation (STROBE-MR): explanation and elaboration. BMJ. 2021;375:n2233. 17. Pape H-C, Moore E, Mckinley T, Sauaia A. Pathophysiology in patients with polytrauma. Injury. 2022;53:2400–2412. 18. Dienstknecht T, Rixen D, Giannoudis P, Pape HC. Do parameters used to clear noncritically injured polytrauma patients for extremity surgery predict complications?
留言 (0)