During the Sars-CoV-2 pandemic, a dramatic decrease in viral infections has been described in the pediatric population [11], due to social-distancing, closure of schools, implementation of hand washing and the usage of face-masks [4, 5, 7, 27]. This phenomenon included bronchiolitis and has been described in Italy as well [8, 9], and the present findings confirm what observed between September 2020 and April 2021.
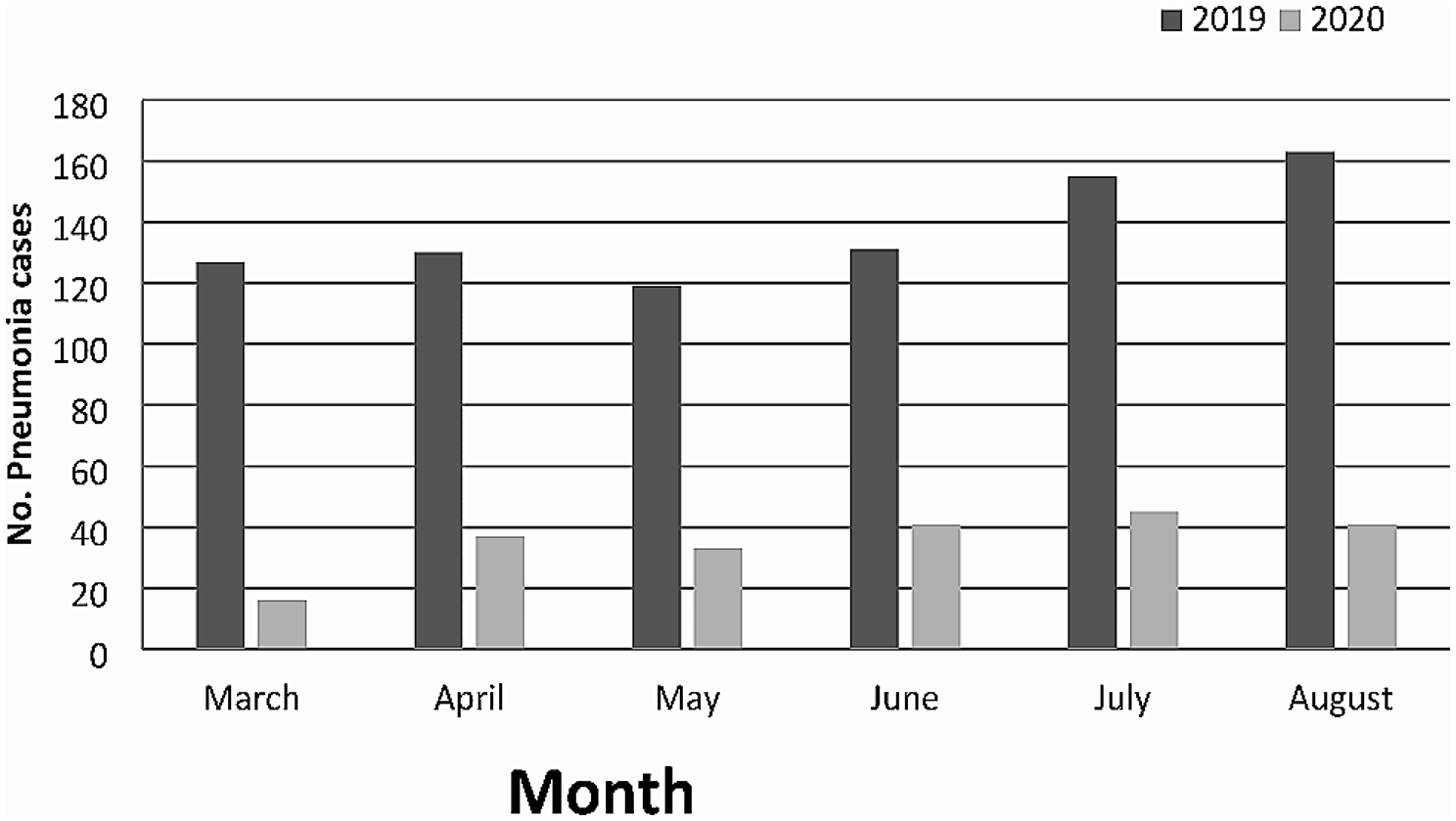
During the summer of 2021, alerts were released concerning an outbreak of an abnormal bronchiolitis season in terms of overall numbers and distribution. It was initially anticipated by pediatricians in the Southern Hemisphere [18], followed by worldwide studies, which reported an increase in overall incidence and an anticipation of the usual peak [6, 15,16,17]. In our results, after a disappearance of bronchiolitis during the first lockdown, an increase in overall incidence during September 2021 and April 2022 was observed. Moreover, this study confirms the anticipated peak and shorter duration of the season described by other Italian reports [19, 20] (Fig. 1).
In the 2021–2022 season, there was a double increase in severity at presentation based on the colour of assignment from triage nurses at admission in ED. Even so, the admission rate did not change throughout the five years.
Guitart et al. [16] describe a more severe 2021 bronchiolitis season in comparison to the previous ten years in terms of length of stay and need of pediatric intensive care unit. Whereas, in Italy, Camporesi et al. [19] do not confirm an unusual disease severity. In our sample, a three time increase after adjustment was observed in intensive care admission during 2021–2022 season in agreement with Guitart et al. findings [16]. It is not possible to completely exclude that the increase in ICU admission in 2021/22 may be due to different criteria adopted by health professionals, but in our opinion it is unlikely, since the availability of beds was scant.
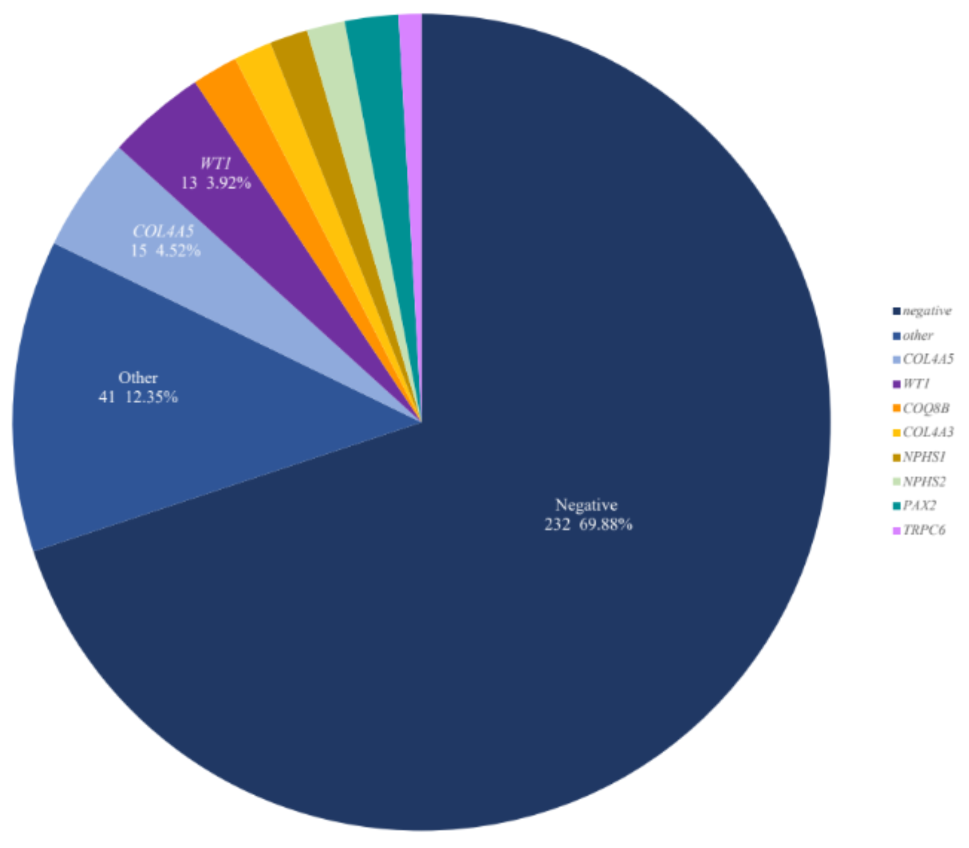
In our study RSV was the main etiological agent as reported in literature [1, 21, 22], except for 2020–2021. Bronchiolitis due to RSV resulted more severe in terms of respiratory support, intensive care and length of hospital stay in comparison to those with RSV negative bronchiolitis. In literature, there is no consensus whether this is true or not [20, 22, 28, 29]. An increase of intensive care accesses and nose-tube feeding, and older age at time of presentation was observed in children with RSV-bronchiolitis and risk factors (e.g. prematurity, other diseases), in accordance with previously reported data [24, 30, 31].
The abnormal bronchiolitis peak may be explained by a global loosening of Sars-CoV-2 prevention measures and an increase in social interactions, in association to a waned herd immunity to other viruses and an increase in RSV-naïve patients. In fact, children affected by bronchiolitis during 2021–2022 were born during the Sars-CoV-2 pandemic, with an immune system that was less stimulated by external agents (bacteria, virus and others) due to all the Sars-CoV2 restrictions; even their mothers were not exposed to infections and did not develop antibodies. Furthermore, Nenna et al. described an opposite hospital admission trend between RSV and Sars-CoV-2 during their study period (2021–2022) confirming a close relationship between these two viruses [20]. A hypothesis which has been addressed is that of “viral interference”: if a person is co-infected by two viruses at the same time, the immune responses toward one of them reduces the possibility to replicate of the other [16, 32, 33]. Another hypothesis that should be considered is that during the Sars-CoV-2 pandemic there may have been a genetic lineage shift in RSV, as previously observed [34]. Finally, an association with weather and air pollution has been hypothesized: climate factors could possibly influence RSV spread, as Nenna et al. [35] suggest on a ten-year study on Italian infants with RSV bronchiolitis before Sars-CoV2 outbreak. Manti et. al [36] argue this hypothesis as well during the 2020 lockdown, during which a 60% decrease of air pollutants was observed, as well as a reduction of RSV bronchiolitis. Further studies are needed.
Analysis of future seasons will allow a better understanding of the impact of Sars-CoV-2 on respiratory infections. Recent reports from the Southern Hemisphere and the United Kingdom describe abnormal Influenza and RSV seasons in terms of incidence and distribution of cases [37,38,39,40].
The limitations of this study are that it is a retrospective single centre study with a limited sample size. The diagnosis of bronchiolitis is clinical; few patients did not have a defined etiological agent. In those without an identified germ, extensive viral testing was not performed. However, the etiological agent, according to Italian and international guidelines, does not affect treatment.





留言 (0)