
記住我
Question: Is there a difference in the in-hospital mortality rates and/or occurrence rate of adverse effects when using baricitinib versus tocilizumab in management of severe COVID-19?
Findings: In this study of a large retrospective cohort of 582 propensity score-matched adult patients, there was no significant difference in the in-hospital mortality when baricitinib or tocilizumab was used for the management of severe COVID-19. However, there was a significantly higher rate of adverse effects with tocilizumab.
Meaning: Our results may provide guidance for clinicians in choosing between the two agents.
Severe COVID-19 is caused by immune dysregulation resulting from complex interactions between the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus and host immune system (1). Although release of inflammatory cytokines can aid virus elimination, uncontrolled secretion can lead to host cell damage. In particular, dysfunction of the interleukin (IL)–6, Janus kinase (JAK), signal transducer, and activator of transcription (STAT) pathway can cause a massive hyperinflammatory phase that eventually leads to multiple organ damage and death (2). Several large studies have shown IL-6 and C-reactive protein (CRP) levels to be predictive of severe disease and death (3–5). Corticosteroids have been shown to have a mortality benefit in severe COVID-19, and other immunosuppressive therapies targeting these specific inflammatory pathways have also showed significant benefit (6).
Baricitinib is a JAK inhibitor that prevents phosphorylation of STAT proteins, causing blunting of immune activation and inflammatory response and may also have direct antiviral activity (7). Although the use of baricitinib with remdesivir showed shorter time to recovery in the Adaptive COVID-19 Treatment Trial 2 (ACTT-2), the Efficacy and Safety of Baricitinib for the Treatment of Hospitalized adults with COVID-19 (COV-BARRIER) study showed a mortality benefit when baricitinib was used in combination with corticosteroids (8,9). Currently, both the National Institutes of Health (NIH) and Infectious Diseases Society of America (IDSA) guidelines recommend baricitinib 4 mg daily for 14 days or until discharge in addition to corticosteroids for patients with severe COVID-19 not on mechanical ventilation (MV) or extracorporeal membrane oxygenation (ECMO) (10,11).
Tocilizumab is a monoclonal antibody that acts as an IL-6 receptor antagonist thereby reducing production of cytokines and acute phase reactants (12). Data from the RECOVERY and Randomized, Embedded, Multifactorial Adaptive Platform Trial for Community-acquired Pneumonia (REMAP-CAP) trials showed that tocilizumab, in combination with corticosteroids, offered a mortality benefit in the subset of patients with severe or critical COVID-19 who were rapidly progressing or had increasing inflammatory markers, including those on MV or ECMO (13,14). Use of a one-time, weight-based tocilizumab dose with corticosteroids in patients with severe or critical COVID-19 and elevated inflammatory markers is currently recommended by NIH and IDSA guidelines. A second dose may be considered at the discretion of the treating physician (10,11). Although tocilizumab has not been approved by the U.S. Food and Drug Administration (FDA) for this indication, it has been issued an Emergency Use Authorization (15).
The combination of both tocilizumab and baricitinib is currently not recommended (10,11). Besides patients on MV or ECMO, it remains unclear which of the two agents offers greater benefit. Although there are studies underway to compare these two agents in the treatment of severe COVID-19, there has been no large-scale peer-reviewed study published to date. The purpose of our study is to retrospectively compare the mortality, clinical outcomes, and adverse effects of baricitinib versus tocilizumab in addition to standard of care in patients with severe COVID-19.
MATERIALS AND METHODSWe conducted a retrospective, observational study of adult patients with severe COVID-19 admitted to an acute care facility within a large health system in Georgia from June 2021 to October 2021 and treated with either baricitinib or tocilizumab.
The protocol for this study, Outcomes and Adverse Effects of Baricitinib versus Tocilizumab in Severe COVID-19, was reviewed and approved by the Wellstar Institutional Review Board (approval number: 1835220; approval date: November 18, 2021). Due to the retrospective, observational design, waivers of informed consent and HIPAA authorization were granted. Procedures followed in this study were in accordance with the ethical standards of the Wellstar Institutional Review Board and the Helsinki Declaration of 1975, as most recently amended (16). The reporting of this study adheres to the STrengthening and Reporting of OBservational studies in Epidemiology statement (17) (Supplemental Appendix 1, https://links.lww.com/CCM/H263).
SettingOur health system includes 11 acute care hospitals located throughout the northwest region in the state of Georgia. Per policy, all admitted patients were tested for COVID-19 via polymerase chain reaction (PCR). Treatment strategies were based on institutional protocols that were updated weekly by a multidisciplinary panel, based on NIH COVID-19 guidelines.
Criteria for use of tocilizumab included hospitalized patients with COVID-19 requiring high-flow (HF) nasal cannula, noninvasive ventilation (NIV), MV, or ECMO if within 3 days of hospital admission or 24 hours of ICU admission. Tocilizumab could also be considered for patients with CRP greater than 7.5 mg/dL or greater than 50% increase in 2 days, with the same time-from-admission considerations.
Criteria for baricitinib use included hospitalized patients with COVID-19 requiring respiratory support with HF, NIV, or those with rapidly increasing oxygen needs. Baricitinib could also be considered for patients who were not candidates for tocilizumab or when tocilizumab was not available due to a national shortage. It was recommended that baricitinib be avoided in patients with a glomerular filtration rate less than 15 mL/min. In patients meeting criteria that overlapped between the two agents, namely those requiring respiratory support with HF or NIV or with rapidly increasing oxygen needs, in the absence of a contraindication to either medication, the selection of baricitinib or tocilizumab was guided by provider preference or drug availability.
Screening for latent tuberculosis and hepatitis B virus was recommended for any patient who received either baricitinib or tocilizumab. Neither agent was recommended for patients in whom there was high suspicion of secondary infection, those with immunocompromising conditions, and those with positive screen for latent tuberculosis or hepatitis B, unless the benefit greatly outweighed the risk in the opinion of the treating physician.
In addition to baricitinib or tocilizumab, other standard of care therapies included corticosteroids for all COVID-19 patients requiring oxygen supplementation and remdesivir for patients presenting within 10 days of symptom onset and requiring oxygen supplementation. During the study period, the Delta variant of SARS-CoV-2 was the dominant variant in our region.
PopulationWe included all adult patients 18 years old and older admitted with PCR positive, symptomatic COVID-19 to an acute care facility within our health system between June and October 2021, who received at least one dose of baricitinib or tocilizumab for management of COVID-19, and survived at least 24 hours from hospital admission. Patients receiving both baricitinib and tocilizumab were excluded, and those who did not receive either agent were not included in the study.
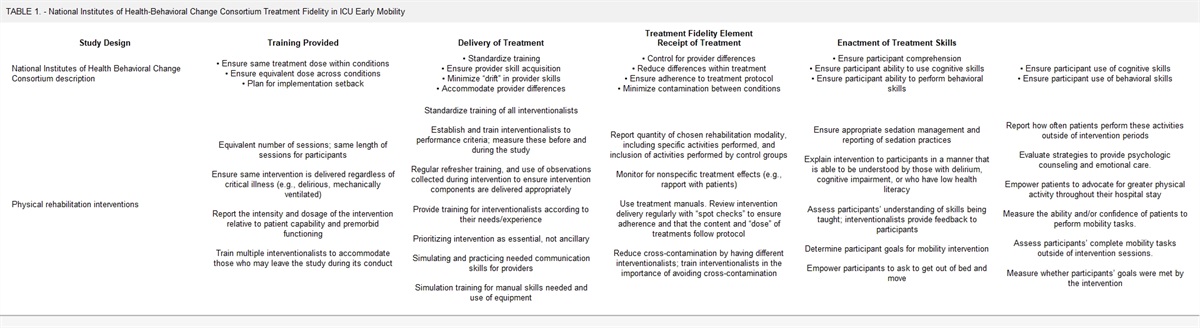
Data Collection and OutcomesData were extracted from electronic medical records (EMRs) by a combination of drug utilization reports and manual chart reviews. Baseline data points included demographics, vaccination status, pre-existing medical conditions, timing of drug initiation from symptom onset, laboratory values, and concomitant use of corticosteroids and remdesivir. Severity of illness was described using the National Institute for Allergy and Infectious Diseases Ordinal Scale (OS) and was documented from drug initiation through day 14 or discharge, whichever occurred first (8) (Table 1; and Supplemental Appendix 2, https://links.lww.com/CCM/H263).
TABLE 1. - National Institute for Allergy and Infectious Diseases Ordinal Scale (8) Ordinal Scale Clinical Status 1 Not hospitalized, no limitations on activities 2 Not hospitalized, limitation on activities and/or requiring home O2 3 Hospitalized, not requiring supplemental O2—no longer requires ongoing medical care 4 Hospitalized, not requiring supplemental O2—requiring ongoing medical care 5 Hospitalized, requiring supplemental O2 6 Hospitalized, on noninvasive ventilation or high-flow O2 devices 7 Hospitalized, on mechanical ventilation or extracorporeal membrane oxygenation 8 DeathOutcome measures included in-hospital mortality, adverse effects, need for MV or ECMO if not on MV or ECMO at baseline, hospital length of stay (LOS), ICU LOS, and comparison of changes in OS over the first 14 days of treatment. Assessment of adverse effects was accomplished via chart review and limited to secondary infection, venous thromboembolism, hypersensitivity, gastrointestinal perforation, acute kidney injury, or acute liver injury. For secondary infections, antibiotic use and positive cultures were considered to avoid inclusion of potential colonizers and strictly empiric antibiotic use. Acute kidney injury was defined according to the Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease criteria (18). Acute liver injury was defined as alanine transaminase or aspartate increase to more than five times the upper limit of normal (Supplemental Appendix 2, https://links.lww.com/CCM/H263).
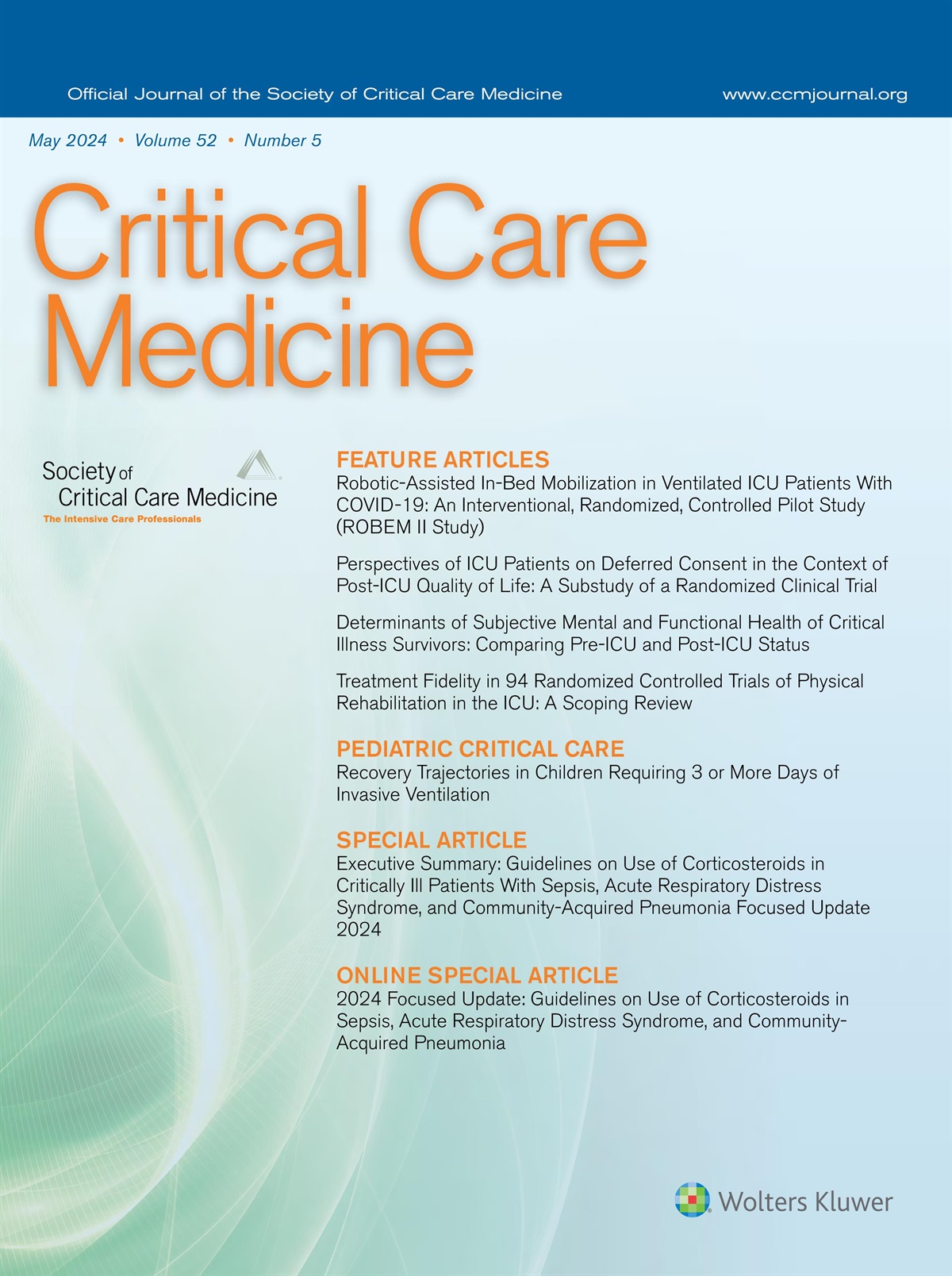
Statistical AnalysisContinuous variables were expressed as median and interquartile range with differences between groups evaluated using Mann-Whitney tests, whereas categorical variables were reported as counts and percentages with differences evaluated using chi-square tests and odds ratios (ORs). A p value of less than 0.05 was considered statistically significant. Given that the study was observational without ability to randomize subjects for treatment, propensity score matching (PSM) using logistic regression was applied to control for differences in baseline attributes and patient characteristics receiving either tocilizumab or baricitinib. For the logistic regression propensity score model, tocilizumab or baricitinib was modeled as the dependent variable and independent variables were age, body mass index (BMI), sex, number of pre-existing conditions, use of corticosteroids, use of remdesivir, OS on day 1 of therapy (OSD1), and ICU status on day 1 of therapy. These variables were chosen based on evidence that they contribute to COVID-19 outcomes and their ability to describe the clinical status of the patient (19). Due to the high number of missing values, laboratory data were not imputed and were excluded from PSM. PSM was used to address the lack of randomization in this observational study and was selected over inverse probability treatment weighting because of the extreme weights generated using this method (20–22). A greedy algorithm PSM was used with a caliper setting of 0.25. The resulting matched groups demonstrated no significant differences in baseline demographics or characteristics (Fig. 1).
 Figure 1.:
Figure 1.: Standardized mean differences. Illustrates differences seen between groups for each listed data point before propensity score matching (yellow diamonds) and after (green circles). After propensity score matching, all listed data points were similar between groups. Data for all observations (Obs) are described by the blue crosses.
RESULTS Baseline CharacteristicsThe overall population included a total of 956 patients, 665 of whom received baricitinib, whereas 291 received tocilizumab (Supplemental Table S1, https://links.lww.com/CCM/H263). Demographics were comparable between the two groups. The median age of the population was 57 years, and 53% were of male sex. The median BMI was 33.5, and more than 94% of the population were unvaccinated. A majority of the population had at least one risk factor for severe disease. Use of remdesivir and use of corticosteroids were similar in both groups. The median OSD1 was the same in each group at 6.0 (p = 1.00). However, ICU status at baseline differed with 39.6% of baricitinib patients requiring ICU care when treatment was initiated compared with 65.6% of tocilizumab patients. Laboratory values were reported; however, due to the large number of missing values, differences between the groups were not calculated. The median time from hospitalization to treatment initiation was 2 days in the baricitinib group versus 1 day in the tocilizumab group. Most tocilizumab patients received only one dose, with only five receiving a second. The median duration of baricitinib therapy was 8 days.
The variables of age, sex, BMI, number of pre-existing conditions, use of remdesivir, use of corticosteroids, OSD1, and ICU status on day 1 of therapy were used to develop the propensity score model (Fig. 1 and Table 2). A propensity score–matched subgroup of 582 was obtained. All 291 tocilizumab recipients were retained, whereas 291 matched baricitinib recipients were retained of the original 665 patients who received baricitinib. There were no significant differences in the baseline characteristics between the two propensity score–matched groups.
TABLE 2. - Characteristics of Propensity Score-Matched Groups Characteristic Baricitinib, N = 291 Tocilizumab, N = 291 p Agea, median (IQR) (yr) 56.0 (44.0–65.0) 55.0 (44.0–65.0) 0.70 Sexa, n (%) Female 152 (52.2) 141 (48.4) 0.36 Male 139 (47.8) 150 (51.6) Body mass indexa, median (IQR) 34.6 (44.0–65.0) 34.5 (29.2–40.7) 0.39 Pre-existing condition(s)a, n (%) 236 (81.1) 231 (79.4) 0.46 Diabetes mellitus 169 (58.1) 174 (59.8) Essential hypertension 156 (53.6) 127 (43.6) Kidney disease 30 (10.3) 47 (16.2) Immunocompromised state 0 (0.0) 2 (0.7) Pregnancy 2 (0.7) 7 (2.4) Sickle cell disease 0 (0.0) 1 (0.3) Neurodevelopmental disorder 0 (0.0) 1 (0.3) Presence of risk factor(s)b, n (%) 273 (93.8) 274 (94.2) 0.73 0 18 (6.2) 17 (5.8) 1 51 (17.5) 58 (19.9) 2 95 (32.6) 88 (30.2) 3 98 (33.7) 99 (34.0) 4 29 (10.0) 27 (9.3) 5 0 (0.0) 2 (0.7) Ordinal Scale on day 1 of therapya, median (IQR) 6.0 (6.0–6.0) 6.0 (6.0–6.0) 1.00 Remdesivira, n (%) 249 (85.6) 249 (85.6) 1.00 Steroidsa, n (%) 291 (100.0 291 (100.0) 1.00 ICU at baselinea, n (%) 190 (65.3) 191 (65.6) 0.93IQR = interquartile range.
aIncluded in propensity score matching.
bRisk factors include the following: age ≥ 65, body mass index ≥ 30, pre-existing conditions.
After data analysis of the overall population and generation of the propensity score–matched groups, the study outcomes were compared.
Primary OutcomeThere was no difference in the in-hospital mortality rate between the two propensity score–matched groups with this outcome occurring in 30.9% of the baricitinib group versus 32% of the tocilizumab group (OR 0.95; 95% CI, 0.7–1.4; p = 0.79) (Table 3).
TABLE 3. - Outcomes for Propensity Score-Matched Groups Outcome Baricitinib, N = 291 Tocilizumab, N = 291 Adjusted OR (95% CI) p Primary outcome In-hospital mortality, n (%) 90 (30.9) 93 (32.0) 0.95 (0.7–1.4) 0.79 Secondary outcomes Adverse effects, n (%) 102 (35.1) 143 (49.1) 0.6 (0.4–0.8) < 0.01 Infection 64 (22.0) 92 (31.6) 0.6 (0.4–0.9) < 0.01 Thrombotic events 47 (16.2) 71 (24.4) 0.6 (0.4–0.9) < 0.01 Acute kidney injury 19 (6.5) 22 (7.6) 0.9 (0.5–1.6) 0.63 Acute liver injury 9 (3.1) 24 (8.3) 0.4 (0.2–0.8) < 0.01 Time to OS < 5 or discharge (d), median (IQR)a 5.0 (0.0–13.0) 5.0 (0.0–15.0) NA 0.63 Change in OS from day 1 to day 14, median (IQR) –1.0 (–6.0 to 1.0) 0.0 (–6.0 to 1.0) NA 0.98 Hospital LOS (d), median (IQR) 14.0 (9.0–23.0) 13.0 (8.0–22.0) NA 0.26 ICU LOS (d), median (IQR) 5.0 (0.0–13.0) 5.0 (0.0–15.0) NA 0.76 Progression to MV or extracorporeal membrane oxygenation, n (%) 69 (23.7) 71 (24.4) 1.0 (0.7–1.4) 0.85LOS = length of stay, NA = not available, OR = odds ratio, OS = Ordinal Scale.
an for this data point differs from that listed in the column header.
Further subgroup analysis by OSD1 also did not show a statistically significant difference in the in-hospital mortality rate between groups (Table 4).
TABLE 4. - In-hospital Mortality by Ordinal Scale on Day 1 in the Propensity Score-Matched Groups Ordinal Scale on Day 1 of Therapy Baricitinib, N Tocilizumab, N Baricitinib In-Hospital Mortality, n (%) Tocilizumab In-Hospital Mortality, n (%) Adjusted OR (95% CI) p 4 2 2 0 (0.0) 0 (0.0) NA NA 5 16 17 1 (6.3) 1 (5.9) 1.1 (0.1–18.6) 0.96 6 241 218 69 (28.6) 69 (31.6) 0.9 (0.6–1.3) 0.48 7 32 54 20 (62.5) 23 (42.6) 2.2 (0.9–5.5) 0.07NA = not available, OR = odds ratio.
Adverse effects were noted to be lower with baricitinib as compared to tocilizumab in the propensity score–matched groups (OR 0.6; 95% CI 0.4–0.8; p < 0.01) (Table 3 and Fig. 2). Specifically, occurrence rate of secondary infection (OR 0.6; 95% CI 0.4–0.9; p < 0.01), thrombotic events (OR 0.6; 95% CI 0.4–0.9; p < 0.01), and acute liver injury (OR 0.4; 95% CI 0.2–0.8; p < 0.01) were statistically significant. Time to OS less than 5 or discharge was a median of 5 days in each group (p = 0.63). The change in OS from day 1 to day 14 was –1 for the baricitinib group versus 0 for the tocilizumab group (p = 0.98). The median hospital LOS was 14 days for the baricitinib group and 13 days for the tocilizumab group (p = 0.26), whereas the median ICU LOS was the same at 5 days in each group (p = 0.76). Last, progression to MV or ECMO in patients not on MV or ECMO at baseline occurred in 23.7% of patients in the baricitinib group and 24.4% of the tocilizumab group (p = 0.85).
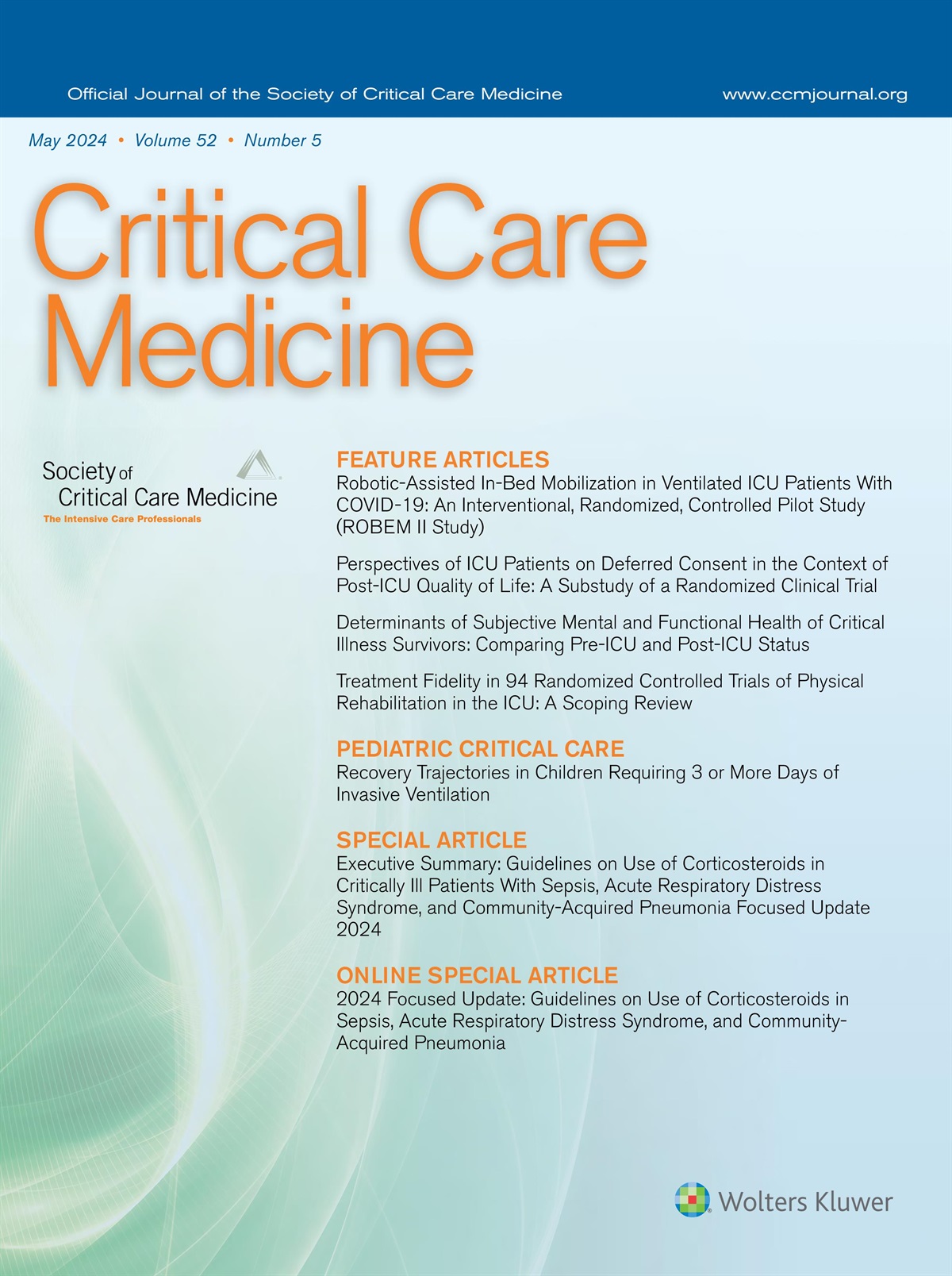
 Figure 2.:
Figure 2.: Description of Ordinal Scale per day of therapy. Illustrates the percentage of patients in each Ordinal Scale category per day of therapy (OSD) from day 1 to 14. Black = OS < 4, orange = OS 4, gray = OS 5, purple = OS 6, blue = OS 7, and green = OS 8.
DISCUSSIONOur study compared real-world outcomes with baricitinib versus tocilizumab for treatment of severe COVID-19 in a large, retrospective cohort. Although either baricitinib or tocilizumab is recommended for treatment of severe COVID-19, selection is often dependent on disease severity, drug availability, and prescriber preference (10,11). The high percentage of unvaccinated patients experiencing severe disease noted in our study is consistent with the Centers for Disease Control and Prevention (CDC) incidence reports during the same time frame in which 98% of severe COVID-19 cases and 98% of COVID-19–associated deaths occurred in unvaccinated patients (23). Although the vaccination rates seen in our study were consistent with those seen across the country at the time, they are lower than current rates. Although vaccination may impact the likelihood of developing severe COVID-19, it is unlikely to significantly impact response to therapies like baricitinib and tocilizumab once severe COVID-19 has developed.
As tocilizumab is recommended for patients on MV or ECMO while baricitinib currently is not, there is greater likelihood of finding larger numbers of critically ill patients treated with tocilizumab. A national drug shortage and provider preference also impacted selection of tocilizumab or baricitinib, which are difficult to account for in a retrospective study design. Other factors that could impact outcomes in a retrospective study on COVID-19 treatments include age, BMI, and comorbidities like diabetes, which are known risk factors for severe COVID-19. Treatment with corticosteroids has been shown to have a mortality benefit in severe COVID-19, which can also influence the outcomes between groups (6,19,24). Given these potentially confounding variables and the retrospective, observational nature of the study, we used PSM to minimize bias. As a result, the outcomes were assessed between comparable groups, increasing validity.
The study did not show a significant difference in the in-hospital mortality between patients with severe COVID-19 treated with baricitinib versus those treated with tocilizumab. This finding was consistent in the propensity score–matched subgroups and subgroup analysis based on OSD1. The time to OS less than 5 or discharge, change in OS from days 1 to 14, hospital LOS, ICU LOS, and progression to MV or ECMO were also similar between the two treatment groups.
Adverse effects were seen more frequently in the tocilizumab group, specifically secondary infections, thrombotic events, and acute liver injury. Most of the evidence on adverse effects of baricitinib and tocilizumab comes from long-term use in rheumatologic conditions. These include increased risk of infections, hepatocellular injury, bone marrow suppression, gastrointestinal perforations, and thrombosis (7,12). In large-scale COVID-19 treatment trials of baricitinib and tocilizumab, respectively, there was no difference in adverse effects observed between the treatment and placebo groups (8,9,13,14). The lower rate of adverse effects seen in our study provides valuable insight into the relative safety of short-term use of baricitinib for severe COVID-19. The pharmacologic half-life of baricitinib is 12 hours and that of tocilizumab is up to 13 days (25,26). Although the full recommended course of tocilizumab for this indication is a one-time IV infusion, the full recommended course of baricitinib is 14 days. The median days of baricitinib treatment in our study was 8. Thus, a more prolonged drug effect may explain the increased adverse effects seen with tocilizumab.
A recently published single-center, retrospective, observational study found no difference in clinical outcomes or adverse effects with baricitinib or tocilizumab. The study considered several similar patient factors including age, sex, BMI, comorbid conditions, vaccination status, concurrent steroid or remdesivir use, and severity of COVID-19 illness at baseline. However, the groups were not matched for baseline characteristics, leading to a possibility of confounding bias. This study also differed from ours in that the only adverse effect assessed was development of secondary infections. Last, this study was much smaller, including only 98 total patients, and was likely significantly underpowered. Although lacking statistical significance, the rates of death and secondary infections were numerically lower in the baricitinib group (27).
Our study has several strengths. First, it includes a large population of patients admitted to 11 different acute care hospitals who are representative of hospitalized patients in the United States. This is also evident in that the rates of vaccination seen in our study are consistent with those reported by the CDC during the same time frame. Second, we addressed a significant knowledge gap in treatment of severe COVID-19 with real-world data. Third, we used PSM to compare the two treatment groups. Baseline demographics, risk factors, and clinical status were matched to minimize confounding bias, making our findings with respect to outcomes more like that which would be seen with a randomized, controlled trial. Fourth, combining automated data collection and manual chart review minimized gaps and strengthened the reliability of the data.
As is the case with most retrospective, observational projects, our study also has some limitations. Although every effort was made to include true data points, some characteristics, such as pre-existing conditions and vaccination status, may have been incomplete in the medical records. Significant percentages of baseline laboratory values were missing, precluding multiple imputation and making comparisons difficult. As a result, they were excluded from PSM. Accurate estimation of race could not be done via EMRs and was not included in the study. As all patients who met criteria were included, we did not perform power and sample size calculations. Due to creation of makeshift ICU units during periods of COVID-19 surge, it is possible that the number of ICU admissions reported in this study were slightly lower than true numbers. Although certain events such as discharge, in-hospital mortality, and adverse effects occurring during the admission but after the 14 days of OS monitoring were captured, interim changes in OS that occurred beyond day 14 were not. Patients were not contacted in follow-up, therefore an accurate estimation of outcomes and adverse effects post hospital discharge could not be done. Specific reasons for why a patient received a certain drug or the number of patients who received baricitinib because they were not candidates for tocilizumab were not captured. Last, along the same lines, there are certainly biases introduced due to factors such as confounding by indication that are difficult to control; however, PSM was used to minimize bias. In addition to these limitations associated with the retrospective, observational design, there are limitations arising from general lack of knowledge surrounding pathophysiology of COVID-19 at this time. Although we matched patients for potential confounding variables that are known to influence COVID-19 outcomes, there may be others that have yet to be determined and were not included in our data collection or PSM scheme.
CONCLUSIONSWe conducted a retrospective, observational study of 956 patients hospitalized with severe COVID-19 who were treated with either baricitinib or tocilizumab at a large health system in Georgia. Our outcome analysis with the propensity score–matched group of 582 patients showed no difference in the in-hospital mortality rate or time to recovery between the two treatments. However, the baricitinib group experienced significantly fewer adverse effects. Although additional prospective, randomized trials are needed to further assess this association, our data suggest that baricitinib may be a better choice when treating patients with severe COVID-19.
ACKNOWLEDGMENTSWe thank Jessica Smith, Rina Nath, Anna Parker, Qiana Boes, and Cristina McLeod.
REFERENCES 1. Mehta P, McAuley DF, Brown M, et al.; HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet. 2020; 395:1033–1034 2. Rabaan AA, Al-Ahmed SH, Muhammad J, et al.: Role of inflammatory cytokines in COVID-19 patients: A review on molecular mechanisms, immune functions, immunopathology and immunomodulatory drugs to counter cytokine storm. Vaccines (Basel). 2021; 9:436 3. Yitbarek GY, Walle Ayehu G, Asnakew S, et al.: The role of C-reactive protein in predicting the severity of COVID-19 disease: A systematic review. SAGE Open Med. 2021; 9:20503121211050755 4. Liu F, Li L, Xu M, et al.: Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J Clin Virol. 2020; 127:104370 5. Lavillegrand JR, Garnier M, Spaeth A, et al.: Elevated plasma IL-6 and CRP levels are associated with adverse clinical outcomes and death in critically ill SARS-CoV-2 patients: Inflammatory response of SARS-CoV-2 patients. Ann Intensive Care. 2021; 11:9. Erratum in: Ann Intensive Care 2021 Jun 9; 11(1):93 6. RECOVERY Collaborative Group; Horby P, Lim WS, Emberson JR, et al.: Dexamethasone in hospitalized patients with COVID-19. N Engl J Med. 2021; 384:693–704 7. Zhang X, Zhang Y, Qiao W, et al.: Baricitinib, a drug with potential effect to prevent SARS-COV-2 from entering target cells and control cytokine storm induced by COVID-19. Int Immunopharmacol. 2020; 86:106749 8. Kalil AC, Patterson TF, Mehta AK, et al.; ACTT-2 Study Group Members: Baricitinib plus remdesivir for hospitalized adults with Covid-19. N Engl J Med. 2021; 384:795–807 9. Marconi VC, Ramanan AV, de Bono S, et al.; COV-BARRIER Study Group: Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): A randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir Med. 2021; 9:1407–1418. Erratum in: Lancet Respir Med. 2021; 9:e102 10. COVID-19 Treatment Guidelines Panel: Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available at https://www.covid19treatmentguidelines.nih.gov/. Accessed April 7, 2022 11. Bhimraj A, Morgan RL, Shumaker AH, et al.: Infectious Diseases Society of America guidelines on the treatment and management of patients with COVID-19. Clin Infect Dis. 2020; 27:ciaa478 12. Mihara M, Ohsugi Y, Kishimoto T: Tocilizumab
留言 (0)