
記住我
KEY POINTS
Question: Is fixed-dose regimen feasible in vitamin K antagonist (VKA) reversal in comparison to variable-dose regimen in VKA reversal?
Findings: The overall analysis revealed that a fixed-dose regimen led to reduced four-factor prothrombin complex concentrate (4-PCC) dosage, faster administration, and higher likelihood of achieving clinical hemostasis. However, while both dose regimens had comparable results when achieving the target international normalized ratio (INR) less than 2, a fixed-dose strategy was less likely to achieve an INR less than 1.5. Importantly, a fixed-dose regimen was associated with a lower mortality and fewer thromboembolic events than a variable-dose regimen. Subgroup analyses of patients based on weight, baseline INR, and 4-PCC indication provide exploratory data to support future studies.
Meaning: The 4-PCC fixed-dose regimen has advantages in terms of cost-effectiveness, administration time, patient outcomes, and safety.
Vitamin K antagonists (VKAs) are the most common anticoagulants used in the management or prophylaxis of thromboembolic events (TEEs [1]). However, VKA use is associated with a significant risk of hemorrhage, which can occur in 10–16% of patients taking VKAs, or even more for patients undergoing emergency surgery (2–4). Furthermore, there is a 1–2% risk of intracerebral hemorrhage (ICH) per year, which rises to 4.2% among elderly patients (5). Urgent VKA reversal may therefore be required in the case of life-threatening hemorrhage or emergency surgery. Four-factor prothrombin complex concentrate (4-PCC) is considered the first-line treatment for VKA reversal due to its superior safety and efficacy over fresh frozen plasma (FFP) but a well-defined strategy for 4-PCC dosing has not been established, especially in emergency situations (6,7). The 2020 American College of Cardiology Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants recommended reversal of VKAs with 4-PCC using either a fixed-dose regimen (1000–1500 international unit [IU]) or a manufacturer-recommended variable-dose regimen based on a patient’s weight and international normalized ratio (INR). Other fixed-dose regimens ranging from 1000 to 2500 IU have been proposed, with inconsistent outcomes (8–10).
Conversely, other studies suggest that a variable-dose regimen has a higher efficacy in achieving INR goals but may be associated with a greater risk of TEEs and mortality (9,11–14). To further determine a suitable fixed-dose and evaluate the safety and efficacy of fixed- vs. variable-dose regimens, we conducted a systematic review and meta-analysis of clinical studies comparing fixed- and variable-dose regimens of 4-PCC for the emergent reversal of VKAs.
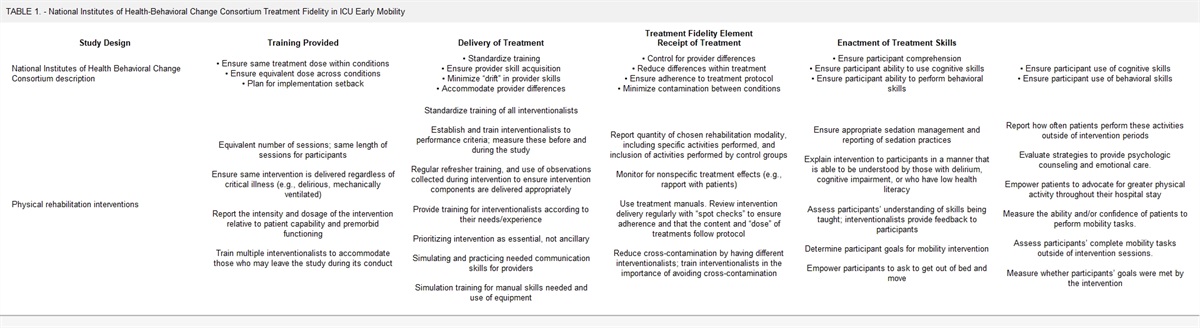
MATERIALS AND METHODS Systematic ReviewA systematic review was conducted according to Cochrane Collaboration and the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines to identify studies comparing fixed- and variable-dose regimens of 4-PCC for the emergent reversal of VKAs (15).
Search StrategyWe searched PubMed (National Library of Medicine), Embase (Elsevier), and Ovid MEDLINE (Wolters Kluwer) databases from January 2000 to August 2023 for articles using keywords associated with vitamin K reversal using 4-PCC (Supplementary Table 1, https://links.lww.com/CCM/H489). No restrictions on language, date, or article type were applied. This protocol was not registered, and no funding was received.
Study Selection and Inclusion CriteriaTwo reviewers (A.A., M.B.P.) independently performed study selection using prespecified inclusion and exclusion criteria. Initial search results were screened by title for the removal of duplicates. The remaining articles were then screened for relevance based on title and abstract. Articles progressing to full-text review were screened for final inclusion based on the following prespecified inclusion criteria: 1) written in or translated into the English language, 2) unique population of patients on VKAs, 3) intervention of VKA reversal using a fixed-dose regimen of 4-PCC, and 4) comparator of VKA reversal using a variable-dose regimen of 4-PCC.
Data Collection and OutcomesData collected included baseline patient characteristics such as age, sex, weight, body mass index, reason for reversal, and baseline INR. Treatment variables collected included the dose of 4-PCC used, time to 4-PCC administration, and administration of additional 4-PCC, other VKA reversal products (vitamin K, FFP), or blood products. Time to 4-PCC administration was defined in two ways in the included studies: 1) the time from hospital presentation to 4-PCC administration (“door-to-needle”) or 2) the time between order entry and 4-PCC administration (“order-to-needle.”) Efficacy was assessed by the overall INR achieved by 4-PCC administration as well as the achievement of specific goal INR values. Given the heterogeneity of reported goal INRs, we pooled INR targets into INR less than 2 and INR less than 1.5. Additionally, four studies (10,14,16,17) evaluated the efficacy outcome of “clinical hemostasis,” which was defined as the absence of major bleeding criteria as set by the International Society on Thrombosis and Hemostasis (18). Lower INR targets were not included in our analysis. Safety outcomes included in-hospital mortality, occurrence of TEEs, and hospital length of stay.
Risk-of-Bias Appraisal and Certainty of the EvidenceA quality assessment of observational cohort and randomized clinical trial studies was conducted using the Newcastle-Ottawa Scale (NOS) and the Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I), respectively (19,20). The NOS assesses the quality of observational cohort studies based on eight items that are categorized into three groups: 1) the selection of the study groups (0–4 points), 2) the comparability of the groups (0–2 points), and 3) the study outcomes (0–3 points). An NOS score of 7 or higher indicates a high-quality study. Supplementary Figures 1 and 2 (https://links.lww.com/CCM/H489) illustrate the Risk of Bias Assessments conducted using the Robvis Shinyapp (https://mcguinlu.shinyapps.io/robvis/). Supplementary Figures 4 and 5 (https://links.lww.com/CCM/H489) display the evaluation of publication bias through funnel plots (20,21). In case any bias was detected, additional quantification of bias was performed using the Begg-Mazumdar test, Egger test, and the Duval-Tweedie trim-and-fill method (22–24).
Statistical AnalysesMeta-analyses were conducted using the meta-package in R (http://CRAN.R-project.org/package=meta). For studies where continuous variables were reported as median and interquartile range (9,25–27), or median and range (10,28–30), conversion to mean and sd was performed using the methods described by Wan et al (31). In cases where continuous variables were presented as mean and 95% CI, the sd was computed using the Cochrane methodology as follows: sd = √n × (upper limit–lower limit)/4.128, where n represents the sample size (32,33). DerSimonian-Laird random-effects models were performed for all factors. Effect size was measured as the standardized mean difference (measure = “SMD”) between the fixed- and variable-dosing groups for continuous data and as the odds ratio (measure = “OR”) for binary data. For descriptive purposes, weighted pooled raw means (measure = “MN”) of the fixed- and variable-dose groups were also calculated for continuous variables. Statistical significance was set at a p value of less than 0.05. No correction was made for multiple comparisons for this exploratory analysis. Of note, one study was excluded from the baseline INR calculation because it reported a range of INR values (34).
HeterogeneityCochrane’s Q test and the I2 statistic were used to measure heterogeneity across the included studies (35). Heterogeneity is considered significant when the I2 exceeds 50% and Cochrane’s Q test is performed with p value of less than 0.1 (36). Given the small number of randomized controlled trials (RCTs) identified in our systematic review, we also performed separate meta-analyses on cohort studies evaluating 4-PCC dosing regimens. The certainty of the evidence was graded by using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool using GRADEpro Guideline Development Tool (Software). McMaster University and Evidence Prime, 2023. Available at: gradepro.org (37). Evidence outcomes were graded as “high,” “moderate,” “low,” or “very low,” it depends on the evaluation of the risk of bias, inconsistency, indirectness, imprecision, and publication bias. Two reviewers (M.B.P. and A.A.) did the evaluation independently.
To proactively assess potential bias discrepancies, a priori subgroup analyses were also undertaken for various variables based on: 1) study type (RCT and cohort), 2) indication for VKA reversal (all indications, non-ICH patients only, and ICH patients only), 3) mean baseline INR (INR ≥ 4 and INR < 4), 4) patient weight (≥ 80 and < 80 kg), and 5) the administered dose of 4-PCC (1000–1500, 1500–2000, or 2000–2500 IU).
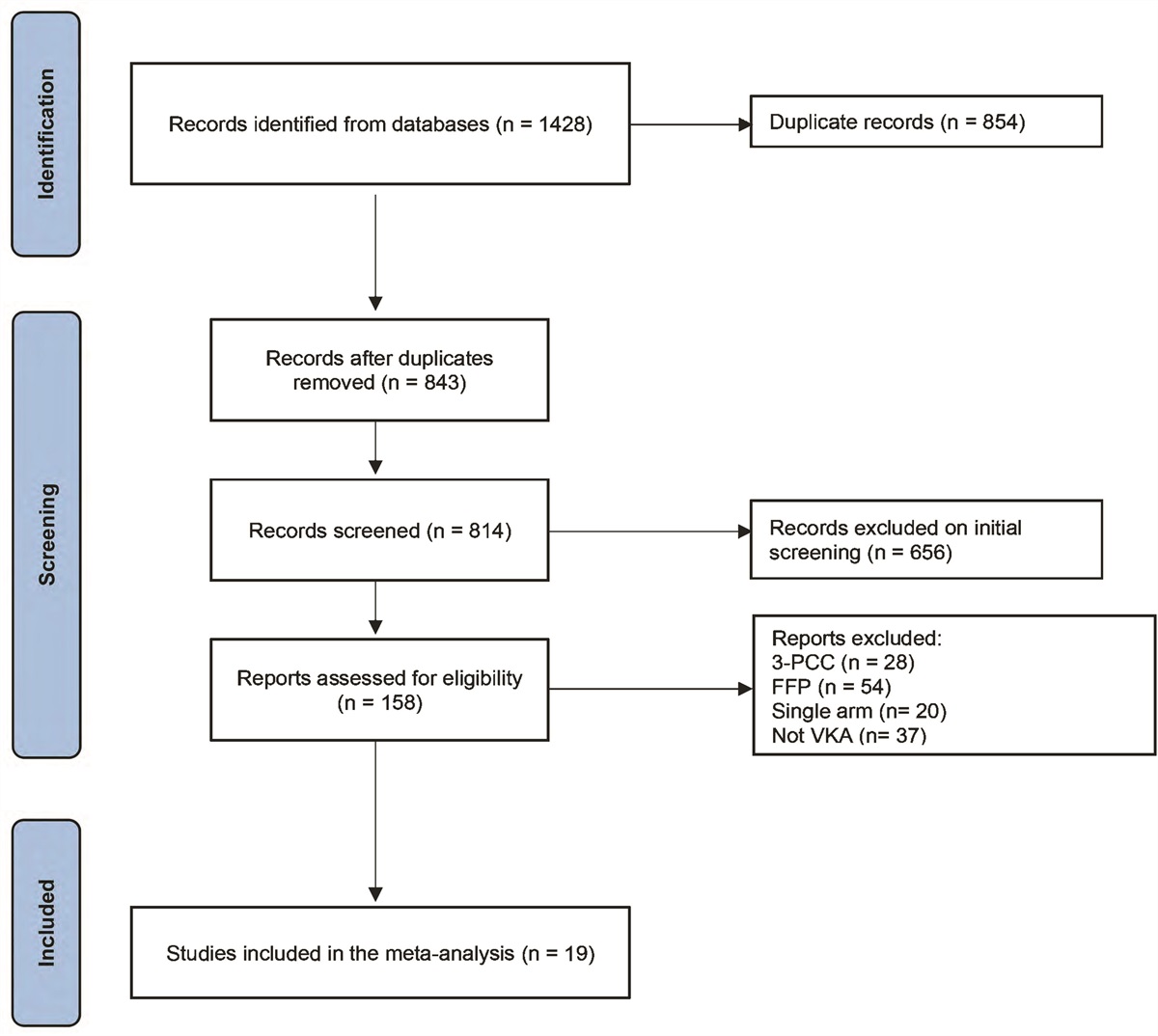
RESULTS Literature Search and Study CharacteristicsWe identified 1428 articles, 19 of which met the prespecified inclusion criteria (Fig. 1; and Supplementary Table 2, https://links.lww.com/CCM/H489). Three studies were prospective RCTs (8–10), one was a prospective cohort of both treatment regimens (29), two were prospective cohorts treated with a fixed-dose regimen compared with historical data (28,38), and the remainder were retrospective studies (13,14,16,17,25–27,30,32,34,39–41). All studies were conducted in the United States or The Netherlands. The U.S. studies used KCentra (CSL Behring, Marburg, Germany) while most of the Dutch studies used Cofact (Sanquin BV, Amsterdam, The Netherlands). One additional Dutch study used Beriplex (CSL Behring, Marburg, Germany) and Cofact (10), whereas two studies did not specify the 4-PCC used (32,39). The fixed-dose regimens varied from 750 to 3000 IU. Variable-dose regimens all followed the respective manufacturers’ recommendations. Four studies included only patients with ICH (27,30,32,39), whereas another three studies included subgroup analysis for ICH patients (17,25,34). ICH patients were specifically excluded from four studies (10,14,28,29). Detailed results of the quality assessment of the included studies are shown in Supplementary Table 2 (https://links.lww.com/CCM/H489). The cohort studies demonstrated high quality, with NOS scores ranging from 7 to 9. Each of the three RCTs included in the review demonstrated a lower risk of bias according to the ROBINS-I tool, suggesting a high level of quality.
 Figure 1.:
Figure 1.: Preferred Reporting Items for Systematic reviews and Meta-Analyses flowchart for indicating the method for selection of articles included in the present study. 3-PCC = three-factor prothrombin complex concentrate, FFP = fresh frozen plasma, VKA = vitamin K anticoagulant.
The RCTs comprised a total of 323 subjects—161 receiving a fixed dose and 162 a variable dose. The cohort studies comprised a total of 1912 patients—858 receiving a fixed dose and 1054 a variable dose. Results from the RCTs were accessible for only 11 variables, whereas the cohort studies encompassed all variables.
Meta-AnalysesSupplementary Table 3 (https://links.lww.com/CCM/H489) shows the primary meta-analyses for both RCT and cohort studies. Supplementary Tables 4 and 5 (https://links.lww.com/CCM/H489) detail the GRADE quality of evidence of the meta-analyses of RCTs and cohort studies, respectively. There were no significant differences between the fixed- and variable-dose groups in terms of age, weight, sex, and baseline INR.
Four-Factor PCC AdministrationThe cohort studies evaluated 4-PCC dosing (Fig. 2) as well as administration time metrics between fixed- and variable-dose regimens. A fixed-dose regimen may be associated with a reduced 4-PCC dose compared with a variable-dose regimen (1537.3 vs. 2222.2 IU; SMD, –1.02; 95% CI, –1.3 to –0.8; low certainty). Similarly, the dose per weight may also be reduced with a fixed-dose regimen (22.1 vs. 27.7 IU/kg; SMD, –0.5; 95% CI, –1.03 to 0.0002; low certainty). A fixed-dose regimen results in a significant reduction in order-to-needle time (39 vs. 72 min; SMD, –0.4; 95% CI, –0.6 to –0.2; high certainty) as well as shorter PCC-to-INR time (147.4 vs. 192.5 min; SMD, –0.3; 95% CI, –0.5 to –0.1; high certainty) when compared with variable-dose regimens.
 Figure 2.:
Figure 2.: Forest plots for primary meta-analyses comparing fixed- vs. variable-dose four-factor prothrombin complex concentrate (4-PCC) administration. df = degrees of freedom, ICH = intracerebral hemorrhage, OR = odds ratio, RCT = randomized controlled trial, SMD = standardized mean difference.
Efficacy OutcomesClinical hemostasis was evaluated by cohort studies, which showed that a fixed-dose strategy likely results in increased clinical hemostasis compared with a variable-dose regimen (74.1% vs. 61.6%; OR, 1.7; 95% CI, 1.05–2.8; moderate certainty). Both cohort and RCT studies evaluated the ability of fixed- and variable-dose regimens to achieve goal INRs of less than 2 and less than 1.5 (Fig. 2) Among cohort studies, a fixed-dose regimen is probably slightly less likely to achieve a goal INR less than 2 than a variable-dose regimen (88.8% vs. 92.4%; OR, 0.7; 95% CI, 0.4–1.2; moderate certainty). The evidence among RCTs regarding the ability to achieve a goal INR is uncertain. Cohort studies showed that a fixed-dose regimen is probably less likely to achieve a goal INR less than 1.5 compared with a variable-dose regimen (64.6% vs. 74.3%; OR, 0.6; 95% CI, 0.5–0.8; moderate certainty) while in RCTs, a fixed-dose regimen results in a lower likelihood of achieving a goal INR less than 1.5 (66.7% vs. 88.6%; OR, 0.3; 95% CI, 0.09–0.8; high certainty).
Safety OutcomesA fixed-dose regimen was associated with lower mortality compared with a variable-dose regimen in both cohort studies (15.6% vs. 18.8%; OR, 0.8; 95% CI, 0.6–1.03; high certainty) and RCT studies (4.7% vs. 7.2%; OR, 0.6; 95% CI, 0.1–1.9; high certainty) (Fig. 3). Cohort studies showed that TEEs were reduced with a fixed-dose regimen compared with a variable-dose regimen (2.4% vs. 4.4%; OR, 0.5; 95% CI, 0.3–1; high certainty). Similarly, among RCTs, a fixed-dose regimen likely reduced the rate of TEEs compared with a variable-dose regimen (1.2% vs. 1.8%; OR, 0.7; 95% CI, 0.1–3.8; moderate certainty) (Fig. 3).
 Figure 3.:
Figure 3.: Forest plots for meta-analyses of safety outcomes comparing fixed- vs. variable-dose four-factor prothrombin complex concentrate (4-PCC). A, Mortality. B, Thromboembolic events. df = degrees of freedom, ICH = intracerebral hemorrhage, OR = odds ratio, RCT = randomized controlled trial.
Additional 4-PCC and Blood ProductsA fixed-dose regimen is probably associated with a higher likelihood of administering additional 4-PCC, as shown in both cohort studies (5.2% vs. 3.1%; OR, 1.5; 95% CI, 0.8–2.6; moderate certainty) and RCT studies (17.4% vs. 2.5%; OR, 8.6; 95% CI, 3–24.6; moderate certainty). There were minor differences in FFP administration between fixed-dose and variable-dose regimens in both cohort (16.3 vs. 17.8%; OR, 0.8; 95% CI, 0.5–1.2; low certainty) and RCT studies (5.5% vs. 0.8%; OR, 4.7; 95% CI, 0.7–30.6; low certainty). Additional blood products and vitamin K administration results are detailed in Supplementary Tables 3 and 4 (https://links.lww.com/CCM/H489).
ICU and Hospital Lengths of StayThere is uncertain evidence regarding the effect of a fixed- vs. variable-dose regimen on ICU and hospital length of stays (Supplementary Table 3, https://links.lww.com/CCM/H489).
Subgroup Meta-AnalysesFurther exploratory meta-analyses based on various subgroups are detailed in Supplementary Tables 6–10 (https://links.lww.com/CCM/H489). Safety outcomes based on fixed-dose subgroup are illustrated in Figure 4. Supplementary Figure 3 (https://links.lww.com/CCM/H489) shows forest plots illustrating the results of meta-analyses within the 4-PCC overall dose subgroup. The quality of evidence for these subgroups is provided in Supplementary Tables 11–21 (https://links.lww.com/CCM/H489).
 Figure 4.:
Figure 4.: Forest plots for meta-analyses of safety outcomes comparing fixed- vs. variable-dose four-factor prothrombin complex concentrate (4-PCC) by fixed-dose subgroup. A, Mortality. B, Thromboembolic events. df = degrees of freedom, ICH = intracerebral hemorrhage, OR = odds ratio, RCT = randomized controlled trial.
DISCUSSIONVKA therapy is associated with a risk of life-threatening hemorrhage, which necessitates establishing a standardized protocol to rapidly reverse anticoagulation. While 4-PCC manufacturers recommend a variable-dose regimen of 4-PCC administration, fixed-dose regimens have also been proposed. We, therefore, conducted a comprehensive meta-analysis to evaluate the efficacy and safety of a fixed-dose regimen of 4-PCC compared with a manufacturer-recommended variable-dose regimen. Overall, our findings support the advantages of fixed-dose regimens in several aspects. We observed that fixed-dose regimens were associated with lower 4-PCC doses, which may have implications for cost-effectiveness and efficient utilization of resources. Furthermore, the fixed-dose regimen demonstrated faster administration (“order-to-needle”) times. Our analysis revealed that a fixed-dose regimen may be superior to a variable-dose in achieving clinical hemostasis. Conversely, a fixed-dose regimen seems less likely to achieve a goal INR of less than 1.5, although the evidence if uncertain that there is a difference in these two regimens in their ability to achieve a goal INR less than 2. These data suggest that a fixed-dose regimen may be sufficient to achieve hemostasis in most cases but that it may be less suitable for achieving a more stringent INR target.
In terms of safety, we found with high certainty that a fixed-dose regimen is associated with a lower mortality compared with a variable-dose regimen. Similarly, a fixed-dose regimen was associated with lower TEE rates with high certainty among cohort studies and moderate certainty among RCTs. These findings indicate that fixed-dose regimens may offer better patient outcomes and safety profiles in comparison to variable-dose regimens.
Fixed-Dose RegimensThere have been several fixed-dose regimens reported in the literature. Mohammadi et al (42) concluded that a fixed dose of 1000–1500 IU is safe, effective, and timesaving for VKA reversal in the setting of emergent surgery or major hemorrhage. Additionally, the Prothrombin complex concentrate Prospective Evaluation and Rationalization, study number 3 (PROPER-3) trial compared a fixed-dose regimen of 1000 IU to a variable-dose regimen in patients without intracranial hemorrhage (ICH) and reported similar outcomes (10). Stoecker et al (9) found that 61.8% of patients treated with a fixed dose of 1500 IU achieved an INR less than 1.5 within 15 minutes after receiving the treatment. Similarly, Klein et al (43) reported that a fixed dose of 1500 IU succeeded in achieving the INR less than 2 in 92% of patients and less than or equal to 1.5 in 72% of patients without any associated TEEs.
In the present study, subgroup analyses of fixed-dose regimens of 1000–1500, 1500–2000, and 2000–2500 IU suggest that there is progressive efficacy with increasing dose (Supplementary Fig. 3 and Supplementary Table 9, https://links.lww.com/CCM/H489). The 1000–1500 IU fixed-dose exhibited moderate outcomes when compared with the variable-dose, achieving the goal INR less than 2 (85% vs. 95%) and greater than 1.5 (60% vs. 75%). Furthermore, there is a low certainty of evidence suggesting a potential increase in mortality risk associated with the 1000–1500 IU fixed-dose. On the contrary, the 1500–2000 IU fixed-dose did not outperform the variable-dose in achieving the goal INR less than 2 (88% vs. 91%) and 1.5 (67% vs. 77%), but it surpassed the 1000–1500 IU regimen. Crucially, there is high certainty evidence pointing toward a reduction in overall mortality (14% vs. 21%). In contrast, the 2000–2500 IU fixed-dose demonstrated enhanced outcomes in achieving the goal INR less than 2 (94% vs. 83%) and greater than 1.5 (87% vs. 83%) compared with both the variable-dose and lower fixed-dose regimens. However, this observation is associated with low certainty evidence. Importantly, this higher fixed-dose regimen maintained a lower mortality and TEE rate, supported by moderate certainty evidence. Overall, these data may suggest that a fixed dose of at least 2000 IU may be optimal, although these studies did not directly compare the different fixed-dose regimens.
VKA Reversal for ICHICH in the setting of VKA use is associated with a high mortality (44–46). Subgroup analysis based on indication for VKA reversal (ICH or non-ICH) revealed few significant differences between fixed- and variable-dose regimens in the ICH subgroup. There is moderate-certainty evidence suggesting that using a fixed-dose regimen in ICH leads to a reduction in 4-PCC administration time (“order-to-needle” time) compared with a variable-dose, with an equivalent rate of achieving the goal INR less than 2 and a nearly identical proportion of patients achieving clinical hemostasis. However, there is low-certainty evidence indicating that the fixed-dose approach falls short in achieving the goal INR less than 1.5 (80% vs. 89%). A fixed-dose strategy may also contribute to a reduction TEEs (moderate-certainty evidence). The evidence regarding mortality differences between fixed- and variable-dose regimens in ICH patients is uncertain.
Defining 4-PCC Outcome EndpointsThe optimal INR goal in the setting of VKA-related hemorrhage remains unknown. The primary INR endpoints for previously published studies of 4-PCC in the treatment of VKA-related hemorrhage have therefore varied. Several studies chose an arbitrary INR, ranging from 1.3 up to 2.0 (16,17,28,29). In contrast, only five studies incorporated clinical hemostasis as an outcome, either with or without a specific INR goal. All of these were cohort studies, three of which evaluated clinical homeostatic efficacy as a primary endpoint instead of a specific INR (10,14,16). In the overall analysis and across all subgroups, the fixed-dose regimen demonstrated superior clinical hemostasis compared with the variable-dose, except for ICH subgroup, where there was minimal difference (76.8% vs. 77.4%). Importantly, the fixed-dose regimen exhibited superior safety outcomes, suggesting that achieving clinical hemostasis or an INR less than 2 may be sufficient in most cases. Future studies are needed to better define optimal goals for VKA reversal using 4-PCC.
Use of Standardized Initial Fixed DoseIn summary, these findings suggest that a fixed dose of 4-PCC can be administered more rapidly than a variable dose, may be more effective at achieving clinical hemostasis, and is likely similarly effective at normalizing the INR to less than 2. While it is not clear precisely why a fixed-dose regimen may be superior to a variable-dose regimen in terms of clinical hemostasis, mortality, and TEEs, a potential reason is the improved speed with which a fixed dose can be administered. Eliminating the need for weight-based calculations and patient-specific medication preparation means that a fixed dose of 4-PCC can be given faster and therefore reverse the underlying VKA more rapidly. Further analysis of specific fixed-dose subgroups suggests that a dose of at least 2000 IU may yield optimal results. Based on these data, it is possible that a protocol using a fixed-dose of 2000 IU could therefore provide rapid and effective VKA reversal. Additional 4-PCC could then be given in a variable-dose fashion for specific subgroups, such as patients presenting with ICH or an INR greater than 4, or those weighing greater than or equal to 80 kg.
LimitationsThis study has several limitations that must be considered. First, there were few RCTs included in this meta-analysis and the majority of included trials were retrospective in nature. We separated our analyses by study type (cohort vs. RCT) to address any potential bias from pooling observational and RCT studies. Second, there was variability in the primary outcomes from these studies. This included goal INRs, which we addressed by using composite goal INRs. It also included clinical hemostasis, which was variably defined across studies. Third, some outcomes were only reported by a few studies, limiting patient numbers in subgroup analyses. Finally, despite the low publication bias among the included studies, several of our analyses revealed moderate to high heterogeneity. In a total of 19 primary meta-analyses (Supplementary Table 3, https://links.lww.com/CCM/H489), 10 had an I2 value above 50%, which signifies moderate heterogeneity. Furthermore, 14 had an I2 greater than 21%, the median measure of heterogeneity in the Cochrane library. Nevertheless, it is important to note that all these limitations are considered in the GRADE recommendations, which assess the quality of evidence with a mixed quality of evidence.
CONCLUSIONSThe findings of this meta-analysis indicate that a fixed-dose regimen of 4-PCC may offer advantages in terms of cost-effectiveness, administration time, efficacy, and safety. Furthermore, exploratory subgroup meta-analyses provide further insights into the safety and efficacy of fixed- vs. variable-dose regimens. Despite the mixed quality of evidence, these findings may provide the basis for future studies, offering valuable insights that may contribute to a more precise definition of optimal 4-PCC dosing for emergent VKA reversal.
REFERENCES 1. Holbrook A, Schulman S, Witt DM, et al.: Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141:e152S–e184S 2. Roetker NS, Lutsey PL, Zakai NA, et al.: All-cause mortality risk with direct oral anticoagulants and warfarin in the primary treatment of venous thromboembolism. Thromb Haemost. 2018; 118:1637–1645 3. Wysowski DK, Nourjah P, Swartz L: Bleeding complications with warfarin use: A prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007; 167:1414–1419 4. Healey JS, Eikelboom J, Douketis J, et al.; RE-LY Investigators: Periprocedural bleeding and thromboembolic events with dabigatran compared with warfarin: Results from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) randomized trial. Circulation. 2012; 126:343–348 5. Hart RG, Tonarelli SB, Pearce LA: Avoiding central nervous system bleeding during antithrombotic therapy: Recent data and ideas. Stroke. 2005; 36:1588–1593 6. Witt DM, Nieuwlaat R, Clark NP, et al.: American Society of Hematology 2018 guidelines for management of venous thromboembolism: Optimal management of anticoagulation therapy. Blood Adv. 2018; 2:3257–3291 7. Tomaselli GF, Mahaffey KW, Cuker A, et al.: 2020 ACC expert consensus decision pathway on management of bleeding in patients on oral anticoagulants: A report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020; 76:594–622 8. van Aart L, Eijkhout HW, Kamphuis JS, et al.: Individualized dosing regimen for prothrombin complex concentrate more effective than standard treatment in the reversal of oral anticoagulant therapy: An open, prospective randomized controlled trial. Thromb Res. 2006; 118:313–320 9. Stoecker Z, Van Amber B, Woster C, et al.: Evaluation of fixed versus variable dosing of 4-factor prothrombin complex concentrate for emergent warfarin reversal. Am J Emerg Med. 2021; 48:282–287 10. Abdoellakhan RA, Khorsand N, Ter Avest E, et al.: Fixed versus variable dosing of prothrombin complex concentrate for bleeding complications of vitamin K antagonists-the PROPER3 randomized clinical trial. Ann Emerg Med. 2022; 79:20–30 11. Dager WE: Using prothrombin complex concentrates to rapidly reverse oral anticoagulant effects. Ann Pharmacother. 2011; 45:1016–1020 12. Makhoul T, Kelly G, Kersten B, et al.: Incidence of thromboembolic events following administration of four-factor prothrombin complex concentrate (4F-PCC) for oral anticoagulation reversal. Thromb Res. 2020; 194:158–164 13. Bizzell AC, Mousavi MK, Yin E: Fixed- versus variable-dose prothrombin complex concentrate protocol for vitamin K antagonist reversal. Int J Hematol. 2021; 114:334–341 14. Bajdas H, Handzel M, Uttaro E, et al.: Evaluation of fixed-dose versus variable-dose prothrombin complex concentrate for warfarin reversal. Thromb Res. 2022; 214:76–81 15. Moher D, Liberati A, Tetzlaff J, et al.: Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J Clin Epidemiol. 2009; 62:1006–1012 16. Kim C, Cottingham L, Eberwein K, et al.: Comparison of hemostatic outcomes in patients receiving fixed-dose vs weight-based 4-factor prothrombin complex concentrate. J Emerg Med. 2020; 59:25–32 17. McMahon C, Halfpap J, Zhao Q, et al.: Evaluation of a fixed-dose regimen of 4-factor prothrombin complex concentrate for warfarin reversal. Ann Pharmacother. 2021; 55:1230–1235 18. Khorsand N, Majeed A, Sarode R, et al.; Subcommittee on Control of Anticoagulation: Assessment of effectiveness of major bleeding management: proposed definitions for effective hemostasis: Communication from the SSC of the ISTH. J Thromb Haemost. 2016; 14:211–214 19. Lo CK, Mertz D, Loeb M: Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med Res Methodol. 2014; 14:45 20. Sterne JA, Hernan MA, Reeves BC, et al.: ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016; 355:i4919 21. Sterne JA, Sutton AJ, Ioannidis JP, et al.: Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011; 343:d4002 22. Egger M, Davey Smith G, Schneider M, et al.: Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–634 23. Duval S, Tweedie R, Tweedie R: Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000; 56:455–463 24. Begg CB, Mazumdar M: Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994; 50:1088–1101 25. Zemrak W, Manuel F, Smith KE, et al.: Low-dose compared to manufacturer-recommended dose four-factor prothrombin complex concentrate for acute warfarin reversal. J Thromb Thrombolysis. 2019; 47:263–271 26. Elsamadisi P, Cepeda MAG, Yankama T, et al.: Weight-based dosing versus a fixed-dose regimen of 4-factor prothrombin complex concentrate in obese patients requiring vitamin K antagonist reversal. Am J Cardiovasc Drugs. 2021; 21:355–361 27. Dietrich SK, Mixon MA, Rech MA: Fixed-dose prothrombin complex concentrate for emergent warfarin reversal among patients with intracranial hemorrhage. Am J Emerg Med. 2021; 49:326–330 28. Khorsand N, Veeger NJ, Muller M, et al.: Fixed versus variable dose of prothrombin complex concentrate for counteracting vitamin K antagonist therapy. Transfus Med. 2011; 21:116–123 29. Khorsand N, Veeger NJ, van Hest RM, et al.: An observational, prospective, two-cohort comparison of a fixed versus variable dosing strategy of prothrombin complex concentrate to counteract vitamin K antagonists in 240 bleeding emergencies. Haematologica. 2012; 97:1501–1506 30. Abdoellakhan RA, Miah IP, Khorsand N, et al.: Fixed versus variable dosing of prothrombin complex concentrate in vitamin K antagonist-related intracranial hemorrhage: A retrospective analysis. Neurocrit Care. 2017; 26:64–69 31. Wan X, Wang W, Liu J, et al.: Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014; 14:135 32. Riha GM, Englehart MS, Walton KZ, et al.: A retrospective comparison of the emergent use of fixed-dose four-factor prothrombin complex versus weight-based dosing for intracranial hemorrhage assessing medication delivery time and cost. Int J Physiol Pathophysiol Pharmacol. 2023; 15:98–104 33. Higgins JPT, Thomas J, Chandler J, et al. (Eds): Choosing effect measures and computing estimates of effect. Cochrane Handbook for Systematic Reviews of Interventions. 6.4. Cochrane, 2023. Available at: https://training.cochrane.org/handbook/current/chapter-06. Accessed February 1, 2024 34. Gilbert BW, Morton L, Huffman JB, et al.: Modified version of the American College of Cardiology’s recommendation for low-dose prothrombin complex concentrate is effective for warfarin reversal. Am J Emerg Med. 2020; 38:806–809 35. Higgins JP, Thompson SG, Thompson SG: Quantifying heterogeneity in a meta-analysis. Stat Med. 2002; 21:1539–1558 36. Ioannidis JP, Patsopoulos NA, Evangelou E: Uncertainty in heterogeneity estimates in meta-analyses. BMJ. 2007; 335:914–916 37. Guyatt GH, Oxman AD, Vist GE, et al.: GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008; 336:924–926 38. Bitonti MT, Rumbarger RL, Absher RK, et al.: Prospective evaluation of a fixed-dose 4-factor prothrombin complex concentrate protocol for urgent vitamin K antagonist reversal. J Emerg Med. 2020; 58:324–329 39. Scott R, Kersten B, Basior J, et al.: Evaluation of fixed-dose four-factor prothrombin complex concentrate for emergent warfarin reversal in patients with intracranial hemorrhage. J Emerg Med. 2018; 54:861–866 40. Dietrich SK, Rowe S, Cocchio CA, et al.: Comparison of 3 different prothrombin complex concentrate regimens for emergent warfarin reversal: PCCWaR study. Ann Pharmacother. 2021; 55:980–987 41. Dietrich SK, Mixon M, Holowatyj M, et al.: Multi-centered evaluation of a novel fixed-dose four-factor prothrombin complex concentrate protocol for warfarin reversal. Am J Emerg Med. 2020; 38:2096–2100 42. Mohammadi K, Yaribash S, Sani MA, et al.: Efficacy and safety of the fixed-dose versus variable-dose of 4-PCC for vitamin K antagonist reversal: A comprehensive systematic review and meta-analysis. Cardiovasc Drugs Ther. 2022; 36:533–546 43. Klein L, Peters J, Miner J, et al.: Evaluation of fixed dose 4-factor prothrombin complex concentrate for emergent warfarin reversal. Am J Emerg Med. 2015; 33:1213–1218 44. Baharoglu MI, Coutinho JM, Marquering HA, et al.: Clinical outcome in patients with intracerebral hemorrhage stratified by type of antithrombotic therapy. Front Neurol. 2021; 12:684476 45. Rosand J, Eckman MH, Knudsen KA, et al.: The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med. 2004; 164:880–884 46. Huttner HB, Jüttler E, Hug A, et al.: Intracerebral hemorrhage related to anticoagulant therapy. Nervenarzt. 2006; 77:671–672, 674
留言 (0)