Pleomorphic Ventricular Tachycardia in Dilated Cardiomyopathy Predicts Ventricular Tachycardia Recurrence After Ablation Independent From Cardiac Function: Comparison With Patients With Ischemic Heart Disease
BACKGROUND:
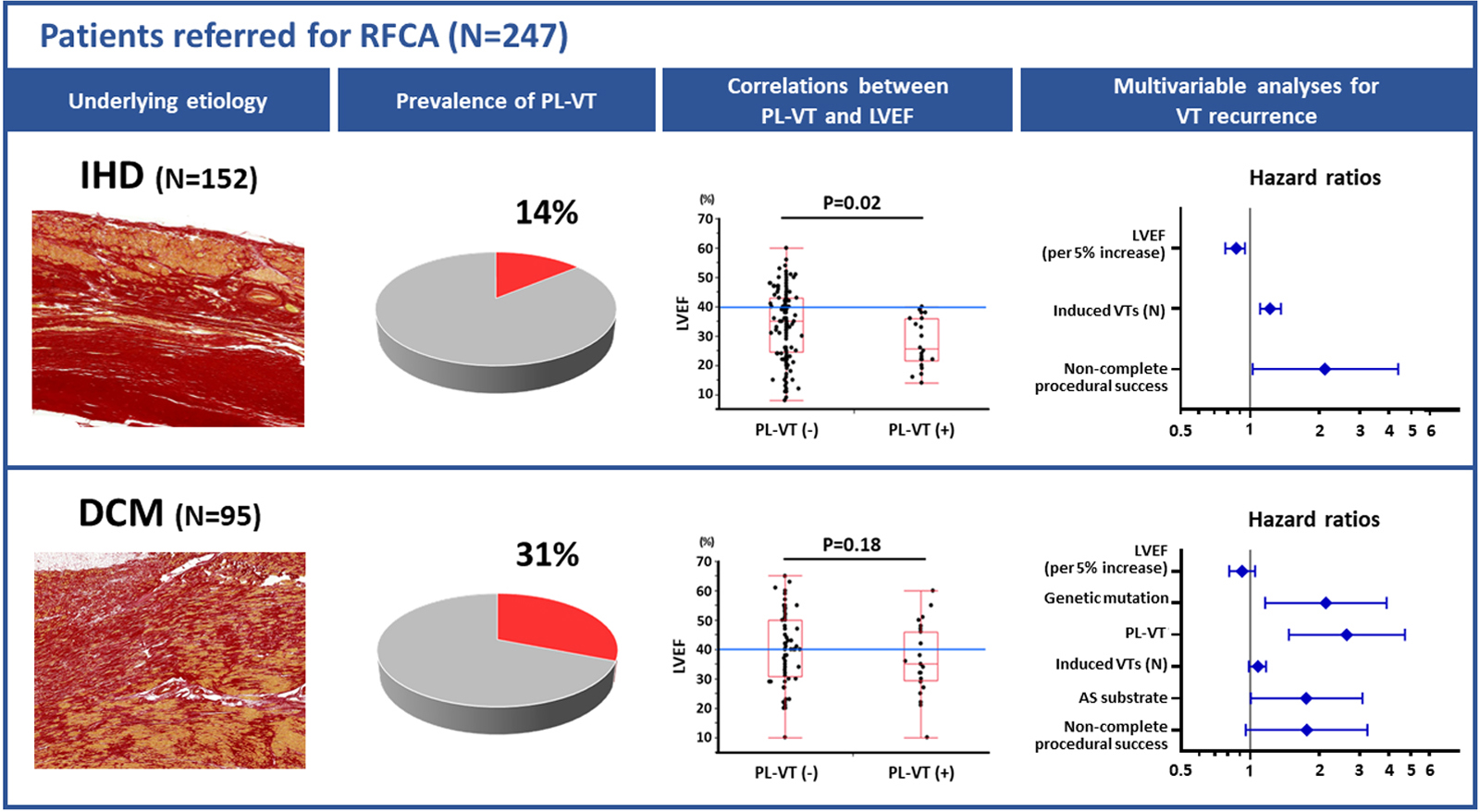
In dilated cardiomyopathy (DCM), outcome after catheter ablation of ventricular tachycardia (VT) is modest, compared with ischemic heart disease (IHD). Pleomorphic VT (PL-VT) has been associated with fibrotic remodeling and end-stage heart failure in IHD. The prognostic role of PL-VT in DCM is unknown.
METHODS:
Consecutive IHD (2009–2016) or DCM (2008–2018) patients undergoing ablation for monomorphic VT were included. PL-VT was defined as ≥1 spontaneous change of the 12-lead VT-morphology during the same induced VT episode. Patients were followed for VT recurrence and mortality.
RESULTS:
A total of 247 patients (86% men; 63±13 years; IHD n=152; DCM n=95) underwent ablation for monomorphic VT. PL-VT was observed in 22 and 29 patients with IHD and DCM, respectively (14% versus 31%, P=0.003). In IHD, PL-VT was associated with lower LVEF (28±9% versus 34±12%, P=0.02) and only observed in those with LVEF<40%. In contrast, in DCM, PL-VT was not related to LVEF and induced in 27% of patients with LVEF>40%. During a median follow-up of 30 months, 79 (32%) patients died (IHD 48; DCM 31; P=0.88) and 120 (49%) had VT recurrence (IHD 59; DCM 61; P<0.001). PL-VT was associated with mortality in IHD but not in DCM. In IHD, VT recurrence was independently associated with LVEF, number of induced VTs, and procedural noncomplete success. Of note, in DCM, PL-VT (HR, 2.62 [95% CI, 1.47–4.69]), pathogenic mutation (HR, 2.13 [95% CI, 1.16–3.91]), and anteroseptal VT substrate (HR, 1.75 [95% CI, 1.00–3.07]) independently predicted VT recurrence.
CONCLUSIONS:
In IHD, PL-VT was associated with low LVEF and mortality. In DCM, PL-VT was not associated with mortality but a predictor of VT recurrence independent from LVEF. PL-VT in DCM may indicate a specific arrhythmic substrate difficult to control by current ablation techniques.

留言 (0)