
記住我


The functional community cohort was established in 2010 in urban Beijing. All participants have received routine annual physical examinations in the physical examination center of Beijing Xuanwu Hospital, Capital Medical University. Most participants (over 80%) are employees of various school companies or local governmental organizations. Both the hospital and university research ethical committees approved the study protocols, and all participants were informed at enrollment. The methods of this study have been described in the previous study [21].
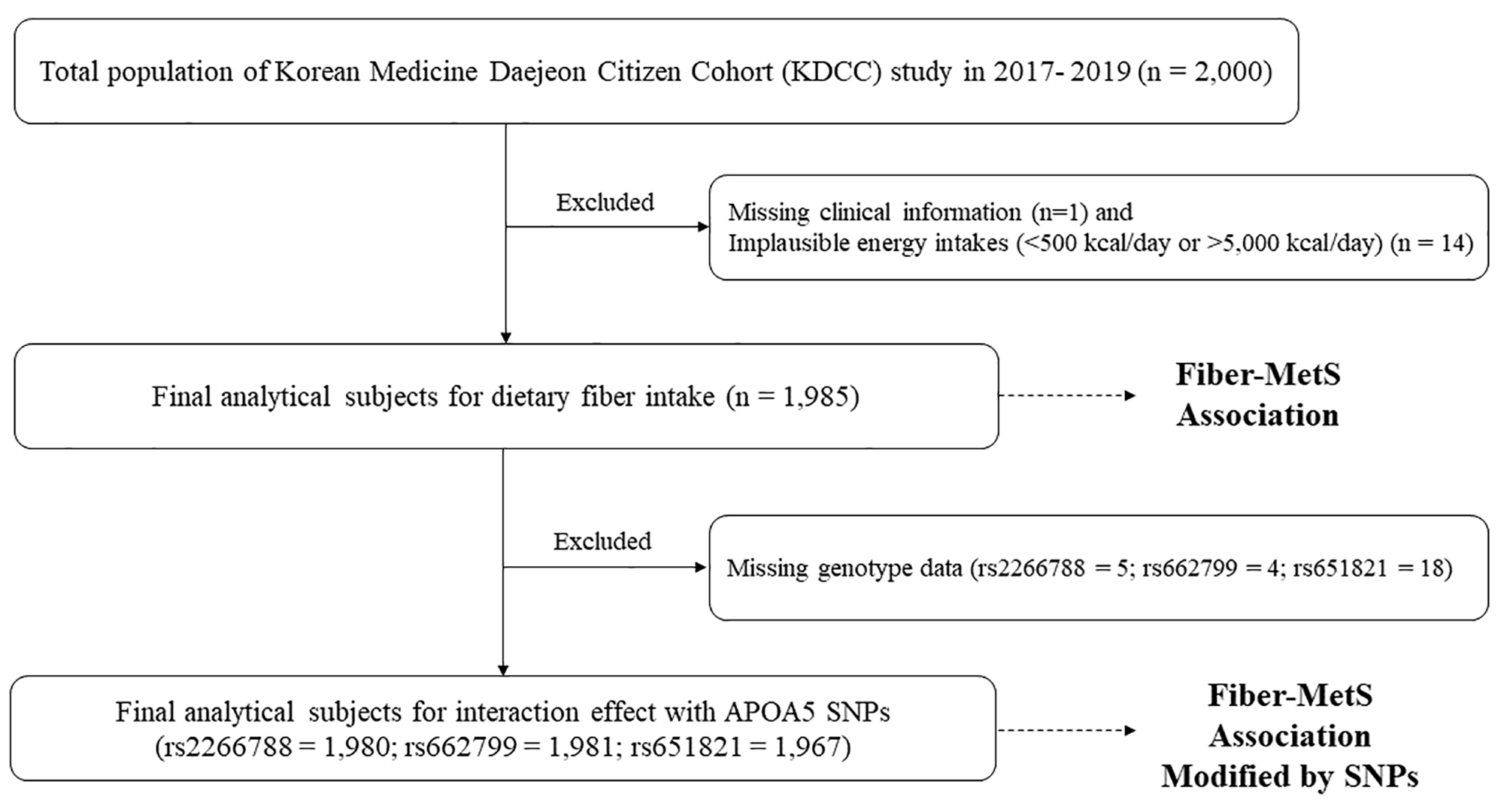
The present study used survey data from 2015 to 2019. Participants were excluded if they miss simultaneously during follow up from 2016 to 2019 [n = 1555, (FPG: n = 341, blood pressure: n = 226, BMI/WC: n = 581; blood lipids: n = 407)] and diagnosed T2D or hypertension in 2015 (n = 1693), leaving 4234 subjects for our analysis (Fig. 1a).
Fig. 1
Flow charts illustrating the criteria for participant recruiting and exclusion. FPG, fasting plasma glucose; BMI, body mass index; WC, waist circumference; T2D, type 2 diabetes. a The functional community cohort; b The China Health and Retirement Longitudinal Study
As most of the participants in the functional community cohort are employees in Beijing, we also analyzed the data extracted from China Health and Retirement Longitudinal Study (CHARLS) to further confirm our conclusions. Briefly, CHARLS is a large-scale longitudinal survey with participants of 45 years of age or older in China. This ongoing cohort study recruited 17,708 participants from 28 provinces in 2011–2012 and follow-up surveys were conducted every 2 years. Details of this study have been described in the previous study [22]. The present study was evaluated based on the cohort from 2011 to 2015. Participants were excluded if they miss simultaneously during follow up from wave 2 (2013) to wave 3 (2015) [n = 11,314, (FPG: n = 10,220, blood pressure: n = 1016, BMI/WC: n = 68; blood lipids: n = 10)] and diagnosed T2D or hypertension in 2011 (n = 1736), leaving 4658 subjects for our analysis (Fig. 1b).
MeasurementsInformation of demographic variables including age (continuous), gender (female, male), education levels (primary or less, high school, university or higher), and health-related behaviors including smoking (yes, no), drinking (yes, no), exercise (yes, no) were collected by trained investigators using a structured questionnaire.
Anthropometric tests including weight, height, and waist circumference were measured by trained professionals. BMI was calculated as weight in kilograms divided by height in meters squared. Blood pressure was measured by trained nurses with an automatic blood pressure monitor. Laboratory examinations: Venous blood samples were obtained from the participants in the morning. Biochemical data including triglyceride (TG), total cholesterol (TC), high density lipoprotein cholesterol (HDL), low density lipoprotein (LDL), and fasting plasma glucose (FPG) were estimated by specialized instruments.
We divided the population into three groups based on WC and BMI. BMI ≥ 24 kg/m2 were considered overweight [23], WC ≥ 90 cm in males and ≥ 85 cm in female were considered central obesity [24]. Obesity groups include Group1 (not overweight and not centrally obesity), Group 2 (overweight or centrally obese), and group 3 (overweight and centrally obese). Dyslipidemia is defined as TC ≥ 200 mg/dL and/or TG ≥ 200 mg/dL and/or LDL ≥ 130 mg/dL and/or HDL < 40 mg/dL [25].
TyG index was calculated as ln (fasting TG[mg/dL]*fasting glucose[mg/dL]/2). TG/HDL index was calculated as TG [mg/dL]/HDL-C [mg/dL]; METS-IR index was calculated as (ln [(2*FPG) + TG]*BMI)/ (ln [HDL-c]).
OutcomeT2D was defined as (1) FPG ≥ 7.0 mmol/L; (2) and/or participants told T2D history; (3) and/or participants were currently using antidiabetic medication.
Hypertension was defined as (1) systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg; (2) and/or participants told hypertension history; (3) and/or participants currently using antihypertension medication.
Statistical analysesThe data of continuous variables were described by means and standard deviations (SDs). Categorical variables were expressed as proportions. Cox proportional hazards models adjusted for age, gender, education, smoking, drinking, exercise, obesity, and dyslipidemia, were used to evaluate the relationship between the surrogate indicators of IR and T2D/hypertension/T2D combined with hypertension. The adjusted hazard ratios (HR) and 95% confidence intervals (CI) were calculated. The predictive value of BMI, TyG, and Mets-IR index for T2D/hypertension/T2D combined with hypertension were evaluated by the area under curves (AUCs) at 4 years which were calculated by time-dependent receiver operating characteristic (ROC) curves for censored survival data. Next, Cox regression models of the restricted cubic spline with 3 knots of baseline TyG index, adjusted for age, gender, education, smoking, drinking, exercise, obesity, and dyslipidemia, were used to examine the shape of the association between the surrogate indicators of IR with incident T2D/hypertension/T2D combined with hypertension. In addition, subgroup analysis was conducted to evaluate the differential association between TyG index with T2D/hypertension/T2D combined with hypertension among age groups (≤45 or 45–65 or > 65 years), gender (male or female), obesity groups, and dyslipidemia (yes or no).
The cross-lagged panel analysis was applied to analyze the association between baseline BMI/WC and follow-up TyG index and the impact of baseline TyG index on follow-up BMI/WC with adjustment for age, gender, education, smoking, drinking, and exercise. The previous study has introduced the application of cross-lagged panel analysis [26], which is a statistical method to deal with the bidirectional relationship between two (or more) observed variables changing with time. In this present study, the cross-lagged panel analysis was conducted using variables measured at three time points in the functional cohort study and two time points in the CHARLS. Figure 2a illustrated the theoretical models, the path coefficients β1 and β3 describe the relationship between baseline TyG index and follow-up BMI, while the path coefficients β2 and β4 describe the relationship between baseline BMI and follow-up TyG index. Both BMI and TyG index values were standardized with Z-transformation (mean = 0; SD = 1). It shows that the standardized regression coefficient of BMI was greater than that of the TyG index. Besides, the comparative fitness index (CFI) was applied to assess the model fit, CFI > 0.90 indicating a relatively good fit.
Fig. 2
Cross-lagged panel analysis models of BMI and TyG index in two cohort studies, adjusted for age, gender, education, smoking, drinking, and exercise. a The functional community cohort, the comparative fitness index = 0.95; b The China Health and Retirement Longitudinal Study, the comparative fitness index = 0.95; TyG, triglyceride and glucose index; BMI, body mass index β1, β2, β3 and β4 indicate cross-lagged path coefficients; r1, indicates synchronous correlation; r2, r3, r4 and r5 indicates tracking correlations; R2 indicates variance explained; *P < 0.05, **P < 0.001
When the temporal relationships between BMI (WC) and TyG index had been established in the cross-lagged panel analysis, the mediation model would be fitted to explore whether the association of BMI (WC) with T2D/hypertension/T2D combined with hypertension was mediated by TyG index after adjusting for age, gender, education, smoking, drinking, and exercise. In the present mediation models, we used baseline BMI (WC) as the predictor variable, follow-up TyG index as the mediator variable, and T2D/hypertension/T2D combined with hypertension as the outcome.
The cross-lagged panel analysis and mediation analysis were performed by Mplus software version 7.0. Other analyses were performed using the SPSS software version 24.0, and R software version 4.0.3. All statistical tests were 2-sided, and statistical significance was set at P < 0.05.
留言 (0)