1. IntroductionChronic hepatitis B virus (HBV) infection is the main risk factor for the development of liver cirrhosis and hepatocellular carcinoma (HCC). Accordingly, around 2–5% of patients with HBV-related liver cirrhosis develop HCC per year and globally, approximately 54% of HCC cases can be attributed to HBV infections [
1,
2]. The risk of developing HCC is variable and driven by several host factors such as the presence of liver cirrhosis, older age and male sex, as well as by HBV factors such as high HBV DNA and HBV surface antigen (HBsAg) levels, certain HBV variants and HBV genotype [
3]. However, apart from those risk factors, host genomic variants have been shown to be associated with the risk of HCC development. Thus, several candidate gene-based case-control association studies have reported that common single nucleotide polymorphisms (SNPs) in various interleukin (IL) genes such as IL-12, IL-10, and IL-4 are associated with HBV susceptibility and HBV persistence or with the risk of HBV-related HCC [
4,
5,
6,
7].The cytokine IL-1β is known to participate in both systemic and local inflammatory processes and to mediate several immune responses [
8,
9]. In carcinogenesis, IL-1β is suggested to increase angiogenesis and promote tumour invasiveness and metastasis [
10]. In the promoter region within the IL-1β gene, three SNPs were described at position rs1143623, rs1143627 and rs16944. Previous studies reported that the IL-1β SNPs were linked to the development and pathogenesis of numerous chronic inflammatory diseases [
11,
12,
13] as well as the progression towards chronic hepatitis B [
14,
15,
16].
In this study, we aimed to assess the association of the common SNPs rs1143623, rs1143627, and rs16944 in the IL-1β gene with the development of liver cirrhosis and HCC in a large multicenter cohort of Caucasian patients with chronic HBV infection.
4. DiscussionIn the present study, we showed for the first time a strong association of the common SNPs rs1143627 and rs16944 in the IL-1β gene with HBV-related HCC in this large multicentre Caucasian population study. The association of the IL-1β polymorphisms with HCC was independent of the known risk factors, such as the presence of liver cirrhosis, older age, male sex and high HBV DNA levels [
3], and independent from the phases of chronic HBV infection, in detail HBeAg-positive or HBeAg-negative CHB and HBeAg-negative infection. In our study, patients carrying the IL-1β rs16944 CC variant had more than seven times higher risk of being diagnosed with HCC than individuals carrying other variants. This finding is in accordance with previous studies performed in Asian populations in which the presence of the rs1644 CC variant increased the HCC risk up to 2.6-fold [
24,
25,
26]—adjusting the analysis to the known risk factors of HCC development, such as the presence of liver cirrhosis, older age and male sex as well as high HBV DNA [
3], a strong association with hepatocarcinogenesis was also observed in patients who were >50 years old and carried the rs16944 CC variant. Similar to the rs16944 SNP, the TT variant of IL-1β rs1143627 was also associated with HCC development in chronic HBV infection. However, the association was not independent of the rs16944 SNP, supporting the possible relationship between both IL-1β polymorphisms. The combination of both genotypes rs1143627 TT and rs16944 CC strengthened the power of HCC risk prediction. Furthermore, in haplotype analysis, the IL-1β rs1143627T/rs16944C haplotype, associated with increased hepatocarcinogenesis, was present in almost 70% of patients with HCC. In our population, the overall risk of HCC development was increased up to 12% in chronically infected patients carrying the IL-1β TC haplotype compared to 8% in patients carrying the CT haplotype. Moreover, in patients with liver cirrhosis carrying the IL-1β risk haplotype, the likelihood of HCC was two times higher than in carriers of the CT haplotype.It is well known that HCC incidence varies between the different phases of chronic HBV infection. The lowest annual risk of HCC development shows patients with chronic HB infection (
1,
2,
3]. In our study, we also detected the fewest number of HCCs in the IC group and no significant differences in HCC diagnosis between HBeAg-negative and HBeAg-positive CHB. The presence of liver cirrhosis was the main risk factor. However, the impact of the IL-1β polymorphisms was independent of the phases of chronic HBV infection, and the presence of liver cirrhosis enhanced the effect. In all subgroups, patients with HCC showed a higher prevalence of the IL-1β variants compared to non-HCC patients.IL-1β regulates various immune [
8,
9] and inflammatory responses [
27] and promotes hepatocarcinogenesis [
10]. Thus, the IL-1β pathway is known to be part of the NLRP3 inflammasome, which in its active form is involved in the upregulation of fibrotic markers in the liver [
28]. Indeed, significant evidence points towards IL-1β as an important mediator of the transition from liver injury to the onset of liver fibrogenesis [
29]. Functional studies supported the association of the IL1-β TC haplotype with more severe stages of chronic liver diseases. Hence, rs1143627 SNP alters the TATA sequence in the promotor region. The T allele was associated with a five-fold higher binding activity to the transcription factors compared to the C allele [
30], resulting in an elevated IL-1β gene expression in human monocytes [
31,
32], A549 cells [
33] and lung tissue [
34]. In an ex vivo blood stimulation assay, the IL-1β TC haplotype was linked to a 2–3-fold increase in the secretion levels of IL-1β after stimulation with lipopolysaccharide [
35]. Furthermore, Su et al. reported that circulating IL-1β negatively affected spontaneous HBV clearance [
36]. Additionally, the IL-1β rs1143623 C allele was demonstrated to have a higher binding to nuclear extract factors in electrophoretic mobility shift assay, suggesting a stronger promotor activity compared to the major G allele [
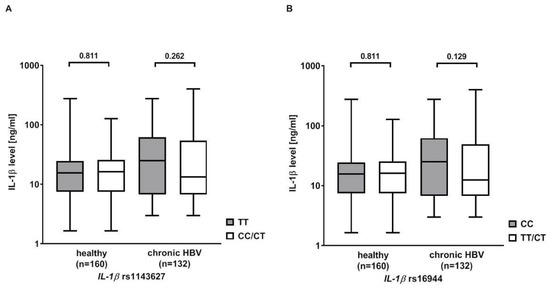
37]. Interestingly, we only found slightly higher IL-1β serum levels in chronically infected patients carrying the rs1143627 TT or rs16944 CC genotypes compared to carriers of the other variants. However, it has been proposed that gene expression is regulated differently in blood cells and liver tissue resulting in divergent protein levels [
38]. Thus, the measurement of cytokine levels in liver tissue might be more reliable.It is still an unanswered question whether polymorphisms in the IL-1ß gene support HCC development via fibrogenesis alone or whether they have an intrinsic hepatocarcinogenic effect. The IL-1ß rs1143627 TT genotype has been shown to be associated with an increased risk for HCC in Japanese patients with hepatitis C virus infection [
39]. The rs16944 SNP was also shown to be associated with a progression towards chronic hepatitis B in patients with acute HBV infection [
5]. Furthermore, in Japanese patients with chronic hepatitis B, an association between IL-1ß polymorphisms and HBV-related histologic hepatic fibrosis could be demonstrated [
40]. In contrast to Migita et al. [
39], we were unable to detect any association between the IL-1β risk variants and ultrasound signs of liver cirrhosis. However, liver histology was available only in a small set (n = 87) of our retrospective population. Furthermore, the measurement of liver stiffness by FibroScan for diagnosing liver fibrosis was only performed in 178 patients [
18]. Nonetheless, the FIB-4 score, which allows an approximate estimation of the presence of liver fibrosis, was associated with the IL-1ß rs16944 risk variant. In fact, apart from increasing the HCC risk by increased fibrogenesis, IL-1β was shown to promote hepatocarcinogenesis independently from the presence of significant fibrosis [
10]. Accordingly, increased levels of IL-1β were measured in the microenvironment of tumour tissues [
41] and serum samples [
42]. Moreover, genetic variants in the IL-1ß locus were also shown to contribute to individual susceptibility in developing metabolic syndrome [
43]. Metabolic factors such as obesity and diabetes and host genetic variants are reported to have a synergistic effect on HCC development in chronic hepatitis B [
44].We have studied the influence of IL-1ß polymorphisms in a population of HBV-infected individuals with similar HCC incidences as reported in other studies. Thus, in Caucasian individuals with chronic hepatitis B, the annual incidence of HCC is 0.3%, and 2.2% in cirrhotic patients [
1,
2]. The corresponding 5-year HCC cumulative incidences are 1% and 10%, respectively [
45,
46]. In our population, the 5-year HCC cumulative incidence was 1.3% in chronic hepatitis B and 3.8% in cirrhotic patients. We, therefore, believe that our results can be extrapolated to other populations with chronic HBV infections. However, this needs to be studied in independent cohorts.One important limitation of our study is the lack of information on HBsAg levels, which are a major risk factor for HCC development in chronic HBV infection [
3]. In our study, HBsAg levels were only available for 258 (40.8%) patients of the total cohort (n = 632) and only in 15 (2.3%) patients with HCC. The patients’ data were retrospectively obtained from medical records dating back to 1996 when the quantitative determination of HBsAg levels had not yet been implemented in the daily practice and had not been routinely conducted. Thus, in upcoming studies focusing on the association of host genetics with hepatocarcinogenesis in CHB, HBsAg levels have to be included in the analysis, especially since it has been shown that HBsAg levels correlate with the phases of HBV infection [
47]. Furthermore, alpha-fetoprotein measurement, a tumour marker supporting diagnosis of liver cancer, was performed in only 115 (18.2%) patients.


留言 (0)