A three-arm international randomised controlled trial (RCT) is currently being conducted across five countries including Australia, Germany, UK, Norway, and Poland. Recruitment (432 dyads) is complete, the trial is due to end in January 2023, and full analysis of results will be in spring 2023. The trial compares the efficacy of the music intervention outlined in this paper, a reading intervention, and standard care. The full aims and scope of this trial have been outlined in a previous publication [
34]. The current paper outlines the development of the HOMESIDE music intervention and preliminary findings from the following sub-studies: 2.1. The HOMESIDE Music Intervention (MI) 2.1.1. Aims and Mechanisms
The HOMESIDE music intervention (MI) aims to train family carers of people living with dementia (dyads) to use music intentionally to support care and foster shared meaningful experiences among community-dwelling people living in their personal surroundings, rather than in hospitals or care homes. The training program embeds a dyad-centred care model, whereby each dyad is trained and facilitated to use music in ways that support their individual interests, needs, and context. The training, delivered online by a credentialed music therapist, provides caregivers with guidelines, resources, and demonstrations to help them select music activities, intentionally engage their family member, create opportunities for meaningful dialogue, and to notice any positive and negative responses to music. The aims of the music activities taught to dyads are to:
provide caregivers with music resources to meet and support the psychosocial and functional care needs of their family member;
enhance reciprocal verbal, non-verbal, and musical communications and human connection;
reduce behavioural and psychological symptoms of dementia (e.g., agitation, apathy, depression);
promote mental stimulation and meaningful experiences “in the here and now” for both members of the dyad;
promote and maintain the person with dementia’s functional independence and engagement in personally satisfying and meaningful occupations; and
validate both members of the dyad as individuals through recognition of their unique identity and history.
The HOMESIDE music intervention is based on well-established theoretical models of music therapy in dementia care, such as autobiographical musical memory, individual musical preferences, person-centred dementia care, validation, arousal regulation, musical attunement, resource-oriented music therapy, and participatory approaches [
25,
35,
36,
37,
38,
39,
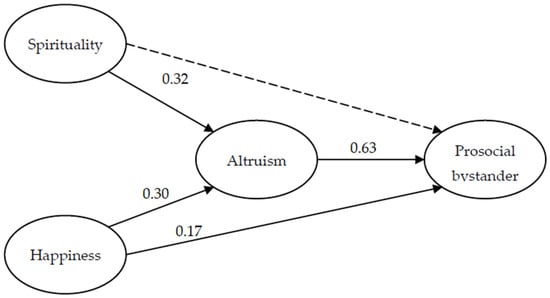
40]. The specific theoretical framework underpinning the effectiveness of HOMESIDE when delivered by the caregiver is illustrated in
Figure 1. Here, the mechanisms underpinning improved wellbeing for the caregiver and person living with dementia occur through a series of experiences that are cultivated through shared music making. Once the caregiver recognises the need for arousal or BPSD regulation, they draw on skills learned during music-therapy training to musically match and attune to the PwD as a means of connecting and regulating them. Through the experience of autobiographical recall and an activation of cognitive reserves, the PwD recognises their family caregiver, thereby creating opportunities for dialogue, connection, sharing meaningful experiences in the here and now, interacting, listening to music, and reminiscing. This experience, in turn, affects the caregiver, who derives pleasure, meaning, and positive emotions from these reciprocal moments of shared musicking, thereby assisting the caregiver to cope better, reinforcing their resilience, and enabling them to sustain their caregiving role (
Figure 1). 2.1.2. Indirect Music-Therapy Training ProgramThe HOMESIDE training program takes place over 12 weeks and includes three bi-weekly training sessions with caregivers in the first six weeks of the program, with phone support provided every other week throughout the 12 weeks. Caregivers are provided with a diary to help them record and reflect on their experiences and determine effective uses of music that work for them. The indirect music-therapy training sessions of HOMESIDE with online COVID-19 adaptations are designed to equip the caregiver to embed music making into everyday life to improve quality of life and reduce dementia symptoms [
34]. During the training sessions, music therapists guide caregivers to select and use music activities to regulate arousal. Caregivers are trained to recognise positive and negative responses and how to adapt the music activities accordingly.The MI demonstrations are informed by those commonly used with people with dementia and their family caregivers and piloted by Baker [
32], Wosch [
41], Odell-Miller [
27,
42] and Tamplin [
43,
44] including: (a) singing familiar/preferred music; (b) movement to music; (c) instrument playing; and (d) listening to familiar/preferred relaxing or activating music as required. After the initial training session, the caregiver is asked to independently implement music sessions with the person with dementia, at least twice per week for approximately 30 min at a time. Additional training sessions are provided at three and six weeks post training to reinforce and further extend caregiver knowledge and skills and monitor adherence to the recommended weekly use. The content of the additional training sessions is tailored to the individual needs and preferences of the participants, so that the sessions are meaningful for each dyad. The music therapist supports the participants by explaining and demonstrating music activities, suggesting and modelling new ideas and providing feedback.
The further training sessions provided at Week 3 and Week 6 aim to consolidate the caregiver’s knowledge and understanding of the programme. In these sessions, the music therapist asks the caregiver to demonstrate the music activities they have been facilitating with the dyad, based on the four activities introduced in the first session. The music therapist then provides feedback and supports the dyad to continue these activities, suggesting alterations as needed. Even if a dyad reports they are not using a certain activity, the therapist can model this again and explore any barriers around implementing the activity. Some activities may not be interesting or right for all dyads, but the therapist can ensure that the dyad has had sufficient training to implement the activity at a later stage should they choose to.
The music therapist carries out phone calls (15–30 min) with the caregiver every other week throughout the intervention. During the phone call, the therapist checks in about the dyad’s wellbeing and how they are progressing with the music intervention. The calls can help to clarify any questions the dyad may have about implementing the intervention, including discussing any problems or negative responses that have occurred. The therapist may aid in choosing music or provide additional resources for accessing personalized music. The phone calls can also provide an opportunity to check in on the caregiver’s wellbeing and support them as needed.
During the initial session, the music therapist introduces the aims of the training session, assesses the needs of the dyad, and assesses the dyad’s music preferences to ensure the training is dyad-centred. This collaborative process may focus on cognitive, behavioural, sensory or mobility challenges, as well as problems arising from medication side effects. An in-depth view of considerations for this needs assessment is based on an established assessment for this population [
45].
Dyads are provided with a music-intervention guideline, which outlines the theory underpinning the use of music, detailed descriptions about the activities and clear strategies for using them. At the end of the training, the carer is encouraged to practice some of the methods while the music therapist is still present. The music therapist provides immediate feedback and additional guidance, thereby enabling participants to experience the activities in action, gain immediate support, and refine their approaches to maximise outcomes.
2.2. The HOMESIDE Music Activities
The music activities should be used with flexibility to respond to individual dyad needs and do not need to be introduced or implemented in any specific order.
Singing
The first activity demonstrated to the dyad is the use of intentional singing to support care and foster meaningful interactions. The dyad is encouraged to sit close, ideally face to face, and then to choose a song familiar to one or both of them. They are then encouraged to sing it together with or without a pre-recorded accompaniment. To assist the caregivers in initiating useful dialogue, they are provided with a list of prompts/questions in the music-intervention guideline to help them engage their family member in memory recall and a shared dialogue. For example, “Do you remember when (e.g., we danced to that song at the church hall?)”; “I loved hearing you sing this song to (child’s name)”; “Does this remind you of the time we…?”
Movement to Music
Dyads are guided to incorporate movement/dance into their daily routines and incorporate it with song singing if appropriate. Instructions about how to recognise what type of familiar and preferred music is suitable for movement/dance are provided. Dancing is encouraged, when safe, to increase engagement.
The music therapist demonstrates creating a safe environment, ensuring there are no objects on the ground that could be tripping hazards, and there is sufficient space to move freely. Explanations of the choice of music appropriate for movement is offered—for example, music that has a strong and steady beat but with simple rhythms. The music should not be too fast as that will mean the movements may be too difficult to execute, but also not too slow, as the beat helps structure the timing of movements. Movement to music may be conducted in sitting, standing, or lying positions. It can be as simple as tapping along to music in bed, or seated reaching movements, or more complex movements to music standing up, including dancing.
Playing instruments
Musical instruments or body percussion can engage dyads in a mutual activity, creating a common space for meaningful connection. Music therapists demonstrate the use of simple percussion instruments and how this can enhance and motivate dyadic interactions. This non-verbal connection might be important, especially in situations where verbal dialogue is limited. Body percussion or instrument playing can be utilised as a separate task to overcome agitation, interrupt stereotypical movements by providing sensory input, or support activities of daily living through task-oriented training.
Music for relaxation
Dyads are trained to identify music that is stimulative and sedative and how to use these musical properties for managing different scenarios. Brief descriptions of relaxing music (sedative) are offered to ensure they understand the components include music with a slow regular rhythm, repetitive melody, few (if any) vocals or lyrics, and an absence of sudden changes in volume, tempo, or complexity to limit the cognitive load. It is helpful to explain and illustrate with concrete examples, that listening to music may trigger sadness that can be experienced as cathartic. Conversely, it is highlighted to dyads that they should avoid music choices that evoke uncomfortable negative emotions for either of them.
To use music intentionally for relaxation, the PwD is encouraged to sit or lie down in a relaxed position, close their eyes, take slow deep breaths, and to become aware of their surroundings. If appropriate, the caregiver can also sit and join in the relaxation experience. The music therapist guides the carer to sit with the PwD and take their hand, and gently stroke it to encourage a deeper relaxation response. This helps both the caregiver and PwD to feel connected to one another and for them to feel safe. The dyad is encouraged to listen to the music together in this relaxed state. If the PwD has difficulty settling, the caregiver could suggest imagery to accompany the relaxation, such as imagining a scene from a holiday that they have had. If the PwD falls asleep during the relaxation, the caregiver is instructed to make them comfortable using pillows, or covering them with a blanket to keep them warm, etc. If they are really enjoying the imagery, the caregiver can encourage them to discuss their imagery or memories stimulated by the experience after the music has finished.
The music used by dyads within the intervention is flexible, based on familiarity and preferences for the participants themselves. The music therapists support the dyads to use a range of music based on both the caregiver and care-recipient’s previous musical experiences and preferences. Due to this flexibility, in our current study, there was a wide range of artists and genres used both within and between dyads. Some examples of the music used includes: “Dancing Queen” by Abba, “We Will Rock You” by Queen, “The Blue Danube” by Johann Strauss, “Memory” by Andrew Lloyd Webber, “Norwegian Wood” by The Beatles, “Ring of Fire” by Johnny Cash, “Hebrides Overture (Fingal’s Cave)” by Felix Mendelssohn, and many more. This is the protocol for the intervention, and further analysis of the musical elements and their meaning will be presented at a later date.
Supportive Tips
Caregivers should be encouraged to be flexible and responsive to the wishes and changing status of the PwD at any given moment.
Table 1 outlines examples of supportive tips provided by the music therapist. 2.3. Data Collection
In addition to measuring quantitative wellbeing outcomes for the PwD and their informal caregivers, data pertaining to dyads’ adherence, experiences, and appraisals of the music intervention are also collected as part of the HOMESIDE trial.
Participant diaries
Dyads participating in the HOMESIDE music intervention complete diaries throughout their 12-week participation. The diaries record which of the four activities the dyads are using at home, their joint responses to the activities and any lasting effects. Caregivers complete a diary page after each music activity they facilitated with the care recipient. Diaries are used to monitor adherence and learn about dyads’ responses to the activities and their experiences. Diaries are mailed to participants at the beginning of their study participation and returned to interventionists after 12 weeks.
Phone-call and training-session records
Qualified music therapists (also termed ‘music interventionists’) complete a record of every phone call and training session conducted with dyads. These records serve to monitor adherence to the intervention and to tailor the content of the training to the dyads’ needs over time.
Participant semi-structured interviews
Participants take part in a semi-structured interview after the 12-week intervention. Interviews consist of 13 primary questions and aim to explore experiences and appraisals of the music intervention and participation in the research study.









留言 (0)