
記住我

Approaches based on lipids (e.g., micelles, LNPs, lipoplex, liposomes, and emulsions), polymers (e.g., polymeric nanoparticles, dendrimers, and polymeric nanoemulsions), and microorganisms (e.g., yeasts, bacteria, archaea, viruses, and virosomes) emerge as alternative systems to be explored by presenting chemical components in their external structure that act in different ways as natural adjuvants. Therefore, this review aimed to discuss the influence of these different systems on the response generated by nucleic acid vaccines, evaluating their efficacy, mechanism, routes of administration, advantages, and limitations.
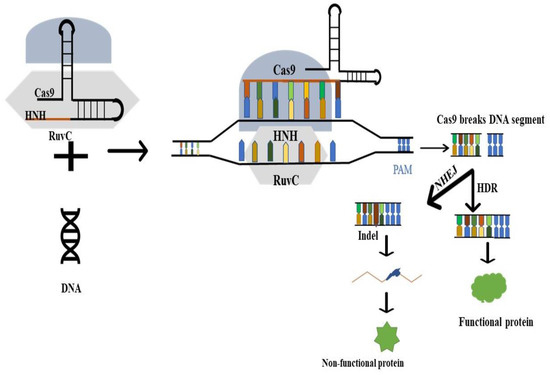
2. Therapeutic Vaccines for HPV-Associated MalignanciesProphylactic vaccines aim to prevent infection by a pathogen, and thus protect the individual from future contact through immunological memory [29]. The application of prophylactic vaccines induces an adaptive immune response primarily focused on the humoral immune response [30]. This immunity is achieved through B cells, but to be successful, it requires the participation of CD4+ T cells, hence depending on effective cellular immunity [31].Capsid proteins from different high-risk HPV strains are used in preventive HPV vaccinations to generate a neutralizing antibody response that prevents recurrent HPV infection [10]. These vaccines are based on viral capsid protein L1 virus-like particles (VLPs) produced and expressed by yeast (such as Saccharomyces cerevisiae) and baculovirus in insect cells [32]. From the spontaneous self-assembly of the L1 protein, a highly immunogenic structure similar to the native conformation of virions is formed, which is then recognized by the immune system cells, inducing the production of neutralizing antibodies [33]. For these vaccines, the significance of the humoral response is evident; nevertheless, studies suggest that B cells may also have an indirect effect in modulating immune responses against HPV-related malignancies [10]. Recent studies show that additional diagnostics and therapies targeting B cells can help predict patients with a better prognosis who would benefit from less invasive treatments [34,35]. In the study by Kim et al. (2020), for example, it was found that in HPV-associated squamous cell carcinomas, B cells improved the overall survival and were activated by radiation and PD-1 blockade. Additionally, Hladíková et al. (2019) found that tumor-infiltrating B cells affect the progression of oropharyngeal squamous cell carcinoma through cell-to-cell interactions with CD8+ T cells.As for therapeutic vaccines, they require the differentiated modulation of the immune system as both chronic infections and cancers are associated with specific immunosuppression and impairment of the immune surveillance system [36]. This vaccine aims to eliminate the disease by increasing, modulating, or redirecting the immune response, thus forcing the immune system to recognize pathogens and abnormal cells [37,38,39]. Since the pathogenic genesis of HPV is linked to the persistent expression of oncogenic viral proteins, most of them are considered as therapeutic targets against HPV-related malignancies [23].It is currently recognized that the oncogenic causative role of high-risk HPV types is fundamentally attributed to the action of the main viral oncoproteins, E6 and E7, which, respectively, inhibit the tumor suppressors p53 and pRB, which are involved in the development of malignancies [40]. These oncoproteins act synergistically, targeting various cellular pathways involved in regulating cell cycle control, promoting cellular immortalization, and facilitating invasion and malignant progression in the host [41]. In addition to these, the HPV E5 protein has been considered an attractive therapeutic target to prevent the progression of precancerous lesions into invasive cervical cancer since it is considered a putative oncogene that acts in the first stage of carcinogenesis, is responsible for regulating the MHC-I, and mediates immune evasion [23,42]. Oncoproteins are constitutively produced at high levels in tumor cells and are not found elsewhere in the human body, which distinguishes HPV-associated cancers [41,43]. This constitutive production makes them an excellent target for the therapeutic vaccines designed to provoke a specific antitumor response, targeting cells that express the antigens and limiting the danger of harming healthy tissue [44].Unlike prophylactic ones, they are primarily focused on cell-mediated immunity and involve the interaction between APCs and naive T cells that will become CD4+ effector cells (via MHC-II) or CD8+ (via MHC-I) [45]. CD4+ cells differentiate into helper T cells that secrete effector molecules, such as cytokines, and may act by increasing the CTL (cytotoxic T lymphocyte) immune response, activating antibody-producing B cells, and modulating regulatory or inflammatory profiles [23]. As with cancer vaccines, CD4+ and CD8+ T cells travel to the tumor site and, upon finding corresponding antigens, kill tumor cells by cytotoxicity and cytokine production [45]. Therapeutic vaccine platforms against HPV-associated cancers in clinical and preclinical stages include bacterial and viral vectors, peptides, proteins, nucleic acids, and, more recently, whole cell-based vaccines [43,46]. Most platforms consisting of attenuated or inactivated pathogens generate a sufficient signal to the immune system to produce memory cells and antibodies [47]. However, they present problems associated with safety, such as virulence reversal, limitations related to efficacy against rapidly evolving pathogens, and demand for production systems with high levels of biosafety [48]. Nucleic acid vaccines, on the other hand, are third-generation vaccines that focus on the synthesis of an antigen of interest and presentation by MHC molecules, allowing the specific induction of cellular responses, which are important in the treatment of cancer, allergies, and autoimmune diseases [49,50]. Furthermore, the production of nucleic acid-based vaccines makes them quick to develop since there is no large-scale growth of highly pathogenic organisms, reducing the cost and the risk of contamination and infection [50]. 3. Nucleic Acid Vaccines against HPV-Related Cancers and Their LimitationsThe DNA vaccine can evoke efficient cellular, and humoral responses compared to conventional and protein-based vaccines and is considered safer, more stable, and easier to manufacture [25].This vaccine is generally produced using recombinant DNA technology and consists of a plasmid containing one or more genes that encode the vaccine antigen (Figure 1A) [51]. Consequently, it is designed to increase the translation and insertion of DNA into cells so that the activation of CD4+ T cells, better induction of CTLs, and antibody production by B cells occurs [51]. After its internalization by the cell and entry into the nucleus, the DNA is transcribed and then translated in the cytoplasm [52]. Then, the encoded antigen is expressed and presented by the MHC to generate CD4+ and CD8+ T cell activation and the indirect activation of humoral immunity [53,54].It is important to note that, although there is still an emphasis on a potential for genotoxicity by chromosomal integration, studies have already shown that it is highly unlikely that the vector will integrate into genomic DNA [55,56,57]. The first DNA-based vaccine for emergency use, in humans, was developed in India for COVID-19. It is known as ZyCoV-D, and it produces the spike protein of the SARS-CoV-2 virus, inducing immune responses aimed at viral elimination. Interim findings from the phase III clinical trial revealed robust immunogenicity, tolerance, and safety profiles [58]. Although this was a milestone for the clinical use of the DNA vaccine, despite veterinary clearance against infectious agents from fish, companion animals, and farms, this platform is still not approved by the FDA for use in humans [59]. One of the main limitations is DNA delivery. These bottlenecks are frequently caused by low-protein expression levels and poor APC uptake, resulting in decreased immunogenicity and low transfection rates [51,60].Examples of clinical trials of therapeutic DNA vaccines against HPV-associated malignancies can be viewed in Table 1. Overall, these vaccines were well tolerated without severe adverse effects and could induce detectable humoral and T-cell responses. However, the percentage of regression or cure was modest, and they are not yet licensed. The phase II vaccine GX-188E, for example, composed of E6/E7 pDNA, was applied to patients positive for HPV 16/18 with CIN3. Among these, 67% of patients 36 weeks after the first injection showed histopathological regression. Although these patients showed increased HPV-specific IFNγ responses, it was impossible to directly correlate with regression [61]. Another vaccine, however, called VGX-3100, developed by INOVIO Pharmaceuticals, reached Phase III of clinical trials (REVEAL 1 and REVEAL 2) and consisted of a mixture of two plasmids containing the optimized E6 and E7 genes of HPV 16/18 delivered by electroporation. This immunotherapy is focused on the treatment of high-grade precancerous cervical dysplasia. Nonetheless, no study results have been published in Clinical Trials (NCT03185013) and are only available as a press release [62].Like the DNA vaccine, the RNA vaccine is a safe and effective platform that encodes antigenic proteins and induces an immune response via antigen presentation [26]. To date, three types of RNA vaccines have been developed, including conventional non-amplifying messenger RNA (mRNA) molecules; self-amplifying mRNA (saRNA) vaccines; and base-modified conventional non-amplifying mRNA (bmRNA) [69]. The basic structure of these vaccines consists of the conventional arrangement of coding molecules present in the body, presenting a 5′ CAP, UTRs regions, open reading frame (ORF), and a PolyA tail (Figure 1B) [70]. Although its application has been previously restricted by RNA instability and inefficient delivery, several studies have investigated this platform for prophylactic and therapeutic applications [71]. Recently, mRNA vaccines developed by Moderna and Pfizer/BioNTech were licensed against COVID-19, reaffirming the potential of this long-studied platform [72]. In mRNA and saRNA vaccines, the property of stimulating adaptive immunity with the induction of B cells and CD4+ and CD8+ T cells was verified [73]. In contrast to the DNA vaccine, RNA vaccines do not require targeting and entry into the nucleus, as their translation into antigenic proteins occurs in the cytoplasm [74]. After processing, epitopes from these proteins are presented via MCH-I by cross-presentation with APCs, which results in the activation of CD8+ T cells and the induction of the immune response [48]. In the case of exogenous proteins, these can be taken up by APCs, degraded by endosomes and presented via MHC-II, leading to the induction of CD4+ T cells [75]. Recently, Komdeur et al. (2021) published the results of the Phase I clinical trial of the first human RNA vaccine based on the Semliki Forest virus (SFV) encoding HPV 16 E6 and E7 antigens against HPV-related cancers. Immunization was safe and well tolerated, resulting in positive vaccine-induced CD4+ and CD8+ T cell-specific immune responses in all study patients with a history of CIN [68]. In addition, the anti-CD40 RNA vaccine (BNT113) developed by Pfizer/BioNTech is currently recruiting previous and recurrent HPV16+ patients against major HPV-associated cancers in its phase I clinical trial [67].However, mRNA vaccines also have limitations. These are mainly related to low stability due to degradation and delivery optimization problems, since specialized delivery systems are needed that allow the integrity of the genetic material and its entry into cells [76,77]. In addition, although they are also considered easy to manufacture and safe, there are logistical limitations regarding the distribution of these vaccines due to the requirement of a cold chain [78,79]. Once both DNA and RNA vaccines have limitations regarding their therapeutic effects, such as a modest percentage of regression or cure, a low correlation between tumor regression and IFNγ responses, and limited thermostability [61,76,77], some strategies to improve T cell function may be necessary to achieve optimal immune responses [36,39]. Among these optimizations are, for example, constructs containing synthetic antigens with multiple epitopes for TC8+, TCD4+, or both, the optimization of codons in the sequences of DNA and RNA, in addition to the use of fat-soluble delivery systems, and platforms with natural adjuvants in the cell wall [80]. The next topic addresses delivery systems used for nucleic acid vaccines that could be further employed in future HPV vaccine strategies. 4. DNA/RNA Vaccine Delivery Systems: A Path to Improve ImmunogenicityMeasures that aid or optimize vaccine formulation are increasingly being researched in order to overcome the limitations of nucleic acid vaccines [27]. For DNA vaccines, the most common tactics to increase immunogenicity include codon optimization, electroporation as a physical delivery method, and adding CpG motifs [70,81]. In addition, the use of molecules and systems capable of helping to modulate the immune system as well as facilitating the uptake by antigen-presenting cells (APCs) is increasingly necessary to generate a robust and well-targeted response [51].Adjuvants are compounds co-injected with the antigen that improve or shape the immune response, aiming to increase the immunogenicity of vaccines, reduce the number of doses needed, and extend immunological memory [31,82]. This adjuvant action is accomplished through mechanisms associated with the activation of the innate immune system that relates to the uptake, presentation, induction of inflammatory mediators, and adjustment of costimulatory molecules [27,36,83]. These substances should ideally have stability and compatibility with the antigen, safety, low cost, and be susceptible to degradation [84]. Adjuvants currently incorporated into FDA-approved prophylactic vaccines or clinical-phase therapeutics that primarily include aluminum-based substances such as aluminum phosphate and aluminum hydroxide, and AS04 (which combines aluminum hydroxide with the monophosphoryl lipid A-MPL agonist) [85]. However, several other adjuvants have been developed and approved for use in licensed human vaccines. In addition to those formulated with aluminum salts, Imiquimod (R837), RIBI-529, oil-in-water emulsions (AS03, AF03, and MF59), and Toll-like receptor (TLR) agonist substances such as TLR9-based agonists are used in synthetic DNA sequences (CpG 1018), consisting of MPL (TLR4 agonist) and QS-21, as the adjuvant AS01B [70,85,86].In the front line of defense against a pathogen, the innate immune system provides a nonspecific response mediated by cells (phagocytic, dendritic, natural killers (NKs)) and by complement molecules through the recognition of molecular patterns by Pattern recognition receptors (PRRs), such as Toll-like (TLRs), NOD (NLRs), RIG-I (RLRs), and C-type lectins [87,88]. Many adjuvants can directly or indirectly activate these receptors to stimulate different types of innate immune responses that, if bound to antigens, can initiate and potentiate areas of the adaptive immune system (composed of T and B lymphocytes, NKs, and mediate molecules such as cytokines [89]. The activation of this system by antigen recognition through the immune synapse with costimulatory molecules and MHC allows the inactivation of the pathogen and the development of immunological memory [90]. It is able to affect the immune response by balancing the induction of humoral and cellular responses. This is made possible by the way in which CD4+ T cells are activated and the types of cytokines released, which results in the expansion of subsets of helper cells (such as Th1, Th2, Th17 and Treg) [91].By secreting antibodies and activating granulocytes (such as neutrophils and eosinophils), Th2 cells mediate the activation and maintenance of the humoral immune response, necessary to remove extracellular infections such as parasites and allergens [92]. The Th1 response, on the other hand, is involved in establishing cellular immunity against intracellular pathogens and cancer cells. Interestingly, individuals with cervical cancer tend to have a Th2 response rather than a Th1 response, and changes in cytokines that drive a Th2 response have also been discovered in cervical tumors, but this has not been fully investigated in HNSCC HPV positive [10,93]. A Th1 response, on the other hand, has been linked to better outcomes in oropharyngeal squamous cell cancer [94,95]. In addition to these, an anti-inflammatory subset of CD4+ T cells, called regulatory T cells (Tregs), is linked to immune homeostasis, promoting self-tolerance [96]. Tregs help prevent autoimmune diseases, allergies, and some types of cancers by ensuring that the immune system’s reaction to self and foreign antigens is balanced [97]. Moreover, Tregs were found in significant numbers in cervical intraepithelial neoplasia (CIN) and cervical cancer, and their frequency corresponded to disease severity, indicating that Tregs may be involved in interfering with anti-HPV immunity [10,98,99]. Furthermore, FoxP3+ regulatory T cell infiltration is a strong and independent prognostic factor in head and neck squamous cell carcinoma [100]. Therefore, to produce a vaccine with the potential to increase the immune response, in addition to considering the parameters that affect its potency and efficacy, it is also necessary to add appropriate adjuvants to its composition and amplify the stimulation of the immune system [101].Adjuvants are generally classified according to the mechanism of action as immunomodulatory molecules, delivery systems, or integrated compositions [88,102]. Immunomodulatory adjuvants, mainly represented by cytokines, chemokines, Toll-like receptor agonists and antimicrobial peptides, act by increasing the host’s immune response [82]. In nucleic acid vaccines, there is a certain limitation in the number of clinical and preclinical studies using immunomodulators in their formulation, especially in mRNA vaccines. This may be reflected by the auto-adjuvanticity of the genetic material that leads to specific humoral and cellular immune responses due to the inherent ability of PRRs to activate the innate immune system as well as the nature of the vaccine [103].In the DNA vaccine, plasmid DNA is intrinsically adjuvanted by the recognition of receptors such as TLR9, NALP3, and cGAS [104]. Although its general use as an adjuvant has limitations, DNA vaccination induces a more Th1-biased immune response and activates MHC antigen presentation pathways for inducing CD8+ and CD4+ T cell immune responses. The strategies of the co-formulation of adjuvants on DNA plasmids encoding the gene of interest, or co-immunization, have been tested in a few studies, but have been used to improve and increase vaccine potency [51]. Among the interleukins, IL-12 has been the most used in therapeutic vaccines against HPV-related cancers, and in general, it appears to improve the efficacy aspects of the DNA vaccine by helping to produce specific humoral and T-cell responses [63]. This pro-inflammatory cytokine has several effects, including the regulation of NK cells and activation of T cells, resulting in a protective Th1 response that stimulates IFN production by T lymphocytes [105]. As for mRNA, it can be recognized by Toll-like receptors such as TLR3, TLR7, TLR8, TLR13, and gene-like receptors I (RIG-I), and is associated with MDA-5 melanoma differentiation [106].However, because RNA is highly immunogenic and prone to degradation, modifications were made that ultimately extended its lifespan but also reduced its modulation of immune responses via cytoplasmic receptors [107]. Although there have not been any clinical and preclinical trials in the literature to date using immunomodulatory molecules for this vaccine, current research aims to increase stability and modulate the immune response to achieve different levels of immunogenicity and antigen expression through modifications of nucleosides and mRNA components (such as 5′ CAP) [106,108]. One such modification was the switch from uridine to pseudouridine, which increased mRNA stability and base methylation to reduce recognition by TLRs, which facilitated its use as a vaccine platform [109,110]. However, depending on the desired vaccine outcomes, it is crucial to balance the resulting adjuvant effects and translation activity to achieve optimal immune responses [111].The incorporation of immunoadjuvants into nucleic acid vaccines represents a promising approach to enable the controlled induction of the innate immune system [111]. However, in addition to knowing the profile of these immunomodulators, it is important to take into consideration how the antigens will be delivered and presented to the cells of the immune system. Thus, another strategy for such a vaccine is the use of carrier or integrated adjuvant delivery systems to increase transfection efficiency, ensure the integrity of the genetic material, and provide a better recognition of immune system cells [112]. Many human vaccines, whether in in vitro or preclinical and clinical research phases, use materials such as liposomes, lipid nanoparticles, aluminum salts, emulsions, and virosomes as delivery platforms for the vaccine antigens [113]. In addition to these, other systems based on microorganisms, lipids, polymers, inorganic molecules, and nucleic acids are investigated as carrier particles [114]. Once injected and containing the antigen of interest, these systems can damage or kill the host cells at the injection site, thus triggering responses against the compounds released by the cells [115].Vaccine delivery systems can function as antigen-associated carriers with adjustable release as well as immune cell recruiters owing to the production of a pro-inflammatory reaction at the injection site, facilitating antigen-specific uptake [116,117,118]. Given the vast diversity of systems, each with its unique properties, factors such as hydrophobicity, size, charge, surface modifications, and material type can influence the interaction with nucleic acids and how they will be perceived by immune cells after vaccine inoculation [119]. Thus, considering the physical and immunological differences of the different carriers for nucleic acid vaccines, the main lipid, polymer, and microorganism-based systems used in nucleic acid vaccines are addressed below (Table 2). 4.1. Lipid-Based Delivery SystemsLipid nanoparticles (LNPs) are an intensively researched non-viral vector for the in vivo delivery of nucleic acid vaccines [142]. NPs refer to all nanoparticles composed of lipids, including various classes such as liposomes, lipoplexes, nanostructured lipid carriers, and cationic nanoemulsions [143]. LNPs are increasingly being used in immunotherapy against cancers and infectious diseases and require specific types and ratios of lipid components when used in nucleic acid vaccines [119]. 4.1.1. LiposomesLiposomes were the first nucleic acid carrier particles to be FDA-approved (with the Doxil Liposome) and the first nanomedicine delivery platform to advance from proof-of-concept to clinical application [144]. They consist of amphiphilic spherical particles composed of one or more phospholipid bilayers surrounded by an aqueous core in which the materials of choice can be encapsulated [119]. In their composition, there is an interaction between the hydrophilic (polar head) and hydrophobic (apolar tail) parts, forming vesicles [145]. They are biodegradable compounds that are versatile, easy to formulate, have substantial efficacy, and may exhibit minimal toxicity depending on the nature of their components [119,146].Although in vivo studies still evaluate the transport efficiency of nucleic acids in pure form, the most common liposomal forms today are hybridized with adjuvant molecules, targeting ligands and polymers [147]. More recent studies of nucleic acid vaccines with conjugated liposomes have shown promise against infectious diseases and cancer immunotherapy and point to aiding in the induction of cellular and humoral responses (Table 2). In addition, the size of liposomes is known to affect the induction of the vaccine response. In general, small liposomes induce a more polarized Th2 response and are therefore more targeted in prophylactic vaccines [148]. On the other hand, larger liposomes help in Th1 bias, being targeted in therapeutic vaccines for cellular response formation [101].Because nucleic acids are anionic, liposomes containing cationic lipids such as DOTMA (N-[1-(2,3-dioleoyloxy) propyl chloride]-N,N,N-trimethylammonium), DOTAP (1,2-dioleoyloxy-3-trimethylammonium), and DDA (dimethyldioctadecylammonium) are preferred [120,122,149]. These lipids, by possessing a positive charge, interact electrostatically with the negative charge of nucleic acids, allowing stability in the encapsulation of the genetic material in the aqueous core [149]. Additionally, they possess adjuvant effects that can be modulated by the nature of the cationic molecule, stimulating the innate immune response, pro-inflammatory mediators, and cytokines [150]. On the other hand, DOPE (1,2-dioleoyl-sn-glycero-3-phosphoethanolamine), which is also widely used, is a neutrally charged auxiliary lipid used to favor cell membrane destabilization and aid the endosomal escape of nucleic acids into the cytoplasm [121,146]. However, destabilization by serum proteins when delivered intravenously, charge-dependent, cytotoxicity and rapid elimination from the body make the transition of liposomes to clinical research problematic [123]. 4.1.2. LipoplexesLipoplexes are liposome-based formulations that are formed upon the electrostatic interaction between the liposome cation and the anionic part of the genetic material [151]. These formulations are characterized by their poor encapsulation, low tolerability, and tendency to aggregate and not completely release the nucleic acid into the target cell [152]. Although the existence of lipoplexes in the drug Patisiran has provided a milestone in the development of siRNA-based drugs, due to these impediments, there are few preclinical and clinical studies employing this system [153]. As with liposomes, some researchers create hybrid formulations with polymeric particles, forming lipopoliplexes (LPPs) and varying their loading to improve the safety and retention in the desired organs after injection [125]. On the other hand, Peletta et al. (2021) developed a DNA vaccine delivered by cationic lipoplexes against SARS-CoV-2. In this study, it was found that lipoplexes amplified in promoting antibody induction and the generation of balanced Th1/Th2 responses in mice against SARS-CoV-2, comparable to those obtained by electroporation with naked DNA. Already in the field of immunotherapy, small-interference RNAs (siRNA) and their interaction with pH-sensitive lipoplexes, peptides, and cell-penetrating polymers are being studied for better uptake by tumor cells [152]. 4.1.3. Emulsions and Cationic NanoemulsionsOil-in-water adjuvant emulsions contain MF59, AS03, and AF03. However, they are utilized prevalently with protein and subunit vaccines and are infrequently employed in nucleic acid vaccines. In the literature, it is reported that MF59 has inclinations towards Th2 immune responses, the stimulation of the humoral and cellular responses, and low toxicity [154]. However, because it was not directly employed as a delivery method for the DNA vaccine, it was not feasible to see a direct association with the reaction created by the vaccination. As for cationic nanoemulsions, they are colloidal particles consisting of an oily core in an aqueous phase stabilized by a cationic lipid or a combination of PEGylated lipids or phospholipids [155]. These nanoemulsions have the potential to inhibit particle aggregation, produce stability, and enhance endosomal escape [156]. However, due to the existence of positive charges and their potential toxicity, the inclusion of non-ionic surfactants such as those employed in the formulation of MF59 (Tween and Span) is advised [156]. In addition, they are examined as carriers for gene-editing treatment and in delivery for protein expression by nucleic acids in immunotherapy of mucosal disorders [127,157]. In the study of Schuh et al. [127], for example, a nasal injection of nanoemulsions carrying a DNA plasmid targeting IDUA protein expression (pIDUA) was undertaken as an attempt to target the brain aiming at gene therapy of Mucopolysaccharidosis Type I. 4.1.4. Lipid NanoparticlesLipid nanoparticles are the most widely used lipid-based systems in nucleic acid vaccines. Although LNPs also encompass other types of lipid systems and have similar composition, they are in themselves a type of system as they exhibit a different organization [158]. Unlike liposomes that contain an aqueous core surrounded by a bilayer, lipid nanoparticles can contain lipids in the core as well as other particles such as ionizable lipids and PEGylates [147]. LNPs have gained even more prominence recently due to their use in Moderna and Pfizer’s mRNA vaccines against COVID-19 [128,129]. Furthermore, in the DNA vaccine field, a study developed by Mucker et al. (2020) showed that LNPs, commonly used in RNA vaccines, also provided improved stability to DNA and the induction of cellular responses for immunoprophylaxis in animals. In approved COVID-19 vaccines, LNPs consist of an ionizable cationic lipid to facilitate internalization, a PEG-lipid to prevent aggregation, cholesterol, and a neutral phospholipid that contributes structurally [159]. Both vaccine types generate significant neutralizing antibody titers and robust antigen-specific CD8+ and Th1-like CD4+ T-cell responses [120,160]. In these vaccines, LNPs provide delivery and protection against degradation by ribonucleases and generate the activation of the innate immune response by generating transient local inflammation at the injection site [161]. However, they need to be stored at low temperatures, requiring a cold chain along the distribution [162]. Moreover, because they contain a certain amount of water in the core, there is the possibility of decreased efficacy and instability due to the possible hydrolysis of the mRNA [161]. An alternative is the use of solid lipid nanoparticles, which can be lyophilized, improving the large-scale distribution of the vaccine, and promoting lower chances of hydrolysis [163]. 4.2. Polymer-Based Delivery SystemsLike lipidic nanoparticles, polymeric systems present a great diversity of molecules and are widely used in drug formulation and gene therapy [164]. The polymer-based systems can be divided in terms of origin as: natural and synthetic polymers, and in terms of type: polyamino acids, polysaccharides, polyamines, polyamidoamines, and polyesters [114]. In recent years, great progress has been made in the employment of polymeric materials as protein carriers and third-generation vaccines [115]. Although they have fewer clinical studies than other systems—especially for mRNA vaccines—these polymers have similar benefits, including stability, diversity, targeting, immunomodulatory activity, and personalization [114]. Cationic polymeric nanoparticles, polyplexes, micelles, lipopolyplexes, copolymers, and dendrimers are examples of representative polymeric formulations used for nucleic acid vaccine delivery (Table 2). However, as with LNPs, problems such as charge-induced cytotoxicity can lead to unwanted side effects, and so the PEGylation of the material is performed to increase stability and decrease overall charge, or the use of neutral polymers [165]. The problem is that this PEGylated material may go on to generate antibodies specific to the delivery system after administration, as occurs with microorganism-based delivery systems [166]. Neutral polymers, on the other hand, are less stable and offer the less efficient transfection of the nucleic acid [164]. In addition, factors such as biodegradability, molecular weight, loading, aggregation, hemolysis, and suboptimal endosomal escape need to be considered and optimized for assembling a successful polymer delivery system [167]. 4.2.1. PolyplexesWhen polymers are complexed with nucleic acids, polyplexes are formed, mainly posed of cationic polymers such as PEI, PLL, PLO, PAMAM, and PLGA, aiming to achieve loading stability via electrostatic interaction with the genetic material [168]. An example of polyplexes can be observed in the work of Soler Besumbes et al. (2019). In this in vitro study, it was found that cationic PLGA nanoparticles prepared using nanoemulsions (NEs) as a template can be used as delivery systems for DNA vaccines. Thanks to the FDA clearance of its use for medical applications, poly(lactic-co-glycolic acid) (PLGA) is one of the most commonly used synthetic polymers for creating polymeric nanocarriers [169]. Interestingly, macrophages and other antigen-presenting cells readily take up polyplexes, including PLGA nanoparticles (APCs), which are known to generate a more significant and longer-lasting immune response [131]. Another example in the preclinical field is the DNA vaccine against Hepatitis B, which uses the polyplexes of the synthetic polymers poly(-amino ester) (PAE) and poly [2-(dimethylamino) ethyl methacrylate] (PDMAEMA) conjugated with the naturally occurring polysaccharide β-glucan [132]. Although no specific cell-based immune response against the antigen has been developed via subcutaneous vaccination, the bioeffects of vaccine formulations regarding hemocompatibility and cytotoxicity are dose-dependent. 4.2.2. CopolymersUnlike other formulations, copolymers contain more than one monomer in their composition [170]. They are easy to administer, relatively simple to manufacture, and are known to provide increased adaptive responses [171]. These features can be seen in the study by Hraber et al. (2018), who produced a DNA vaccine containing ZIKV antigens carried by tetrafunctional amphiphilic block copolymers (ABCs). Although ABC has no adjuvant activity [133], this vaccine applied to mice generated a significant increase in uptake by APCs and a consequent elevation in target protein production by the activation of molecular sensors. 4.2.3. DendrimersDendrimers are synthetic macromolecules that are extremely branched, symmetrical, globular, usually cationic, and dendrite-like [134]. They are mainly used as nanocarriers for targeted drug release and the solubilization of poorly water-soluble drugs [164]. Dendrimers are smaller in size than some of the usual nanocarriers, so they can be easily encapsulated to form a nanohybrid and can be surface absorbed or chemically bound [172]. The characteristic three-dimensional structures of dendrimers allow them to pass through cell membranes without generating disruption like conventional polymers [134]. Polymers such as polyamidoamine PAMAM form positively charged dendrimers and easily interact with nucleic acids [173]. However, it has the disadvantage of not being biodegradable and presenting a high molecular weight, which reflects some toxicity besides being recognized by the innate immune system and activating complement [114]. In contrast, Zhao et al. (2020) developed a veterinary DNA vaccine with a poly-L-lysine dendrigraft delivery that enhanced cellular and humoral responses against chickens’ H9N2 avian influenza virus. This generated dendrimer is biodegradable, less toxic, soluble, and non-immunogenic, representing an alternative to commonly used synthetic dendrimers known for their adverse effects. 4.2.4. Polymeric MicellesPolymeric micelles, made by combining aqueous solution nucleic acids and copolymers (whose properties can be modulated), are often used as mRNA carriers [174]. As such, a novel polymeric micelle based on polyethyleneimine copolymer (PEI) modified with vitamin E succinate (PVES) for mRNA delivery was developed by Ren et al. (2021) for construct evaluation and prophylaxis against SARS-CoV-2. In terms of complement induction and inherent toxicity due to molecular weight and loading, PEI has the same disadvantages as PAMAM [114]. In this construct, however, PEI was modified and, together with vitamin E, which is hydrophobic, formed self-contained amphiphilic copolymers in the micelles, reducing toxicity and inducing T cells, Th1-type immune response, and the amplification of humoral responses against the RBD antigen of SARS-CoV-2. 4.3. Microorganism-Based Delivery SystemsInterestingly, although the main activity of delivery systems is to facilitate the specific antigen uptake by immune system cells, some have integrated composition, showing potent immunomodulatory activities [175]. As seen previously, systems that have cationic materials and synthetic polymers such as PEI and PAMAM can be recognized by immune system cells, potentiating the immune response [164]. Besides these, another carrier platform already known since the early days for immunization against infectious agents is currently gaining more visibility for compound delivery. This platform consists of microorganism-based systems, especially those targeting bacteria and yeast [141,176]. Viruses and archaea also present themselves as carrier platforms, mainly in the form of virosomes and archaeosomes, respectively, or through adjunctive carrier proteins [101,177]. Although studies focus more on subunit vaccines, they have been shown to be potentially useful for nucleic acid delivery [177].As natural adjuvants, they can efficiently activate signaling pathways in immune cells and mobilize the immune system while carrying nucleic acids anchored on the surface or internally [88]. Given their size and complex composition, they are naturally recognized by the defense system and can act as adjuvants by activating pathogen-associated receptors, inducing specific APC uptake [138]. In addition, they amplify the range of administration methods for intranasal, oral, and intravaginal mucosal routes [176]. Some of these organisms are used as immunological adjuvants and food additives and have certification and recognition as safe (GRAS) by the FDA [178,179]. They can be heat-inactivated or modified to ensure host safety to delete their pathogenic components [176,178].However, although these vectors can induce robust immune responses, some of them, especially viruses and bacteria, can be neutralized by components of the host hu-moral immunity after repeated administration and exhibit some cytotoxicity [80]. 4.3.1. Viral Vectors, Virosomes, and Plant Virus ProteinsViral vector-based technologies are generally considered an effective means of delivering genetic material to cells, but current research uses non-viral systems for nucleic acid vaccine delivery [180]. This preference is because their application is sometimes limited by the development of neutralizing antibodies against the vector, safety concerns, and manufacturing limitations [181]. Although article screening did not retrieve clinical and preclinical trials of viral delivery systems for nucleic acid delivery, virosomes and plant viral nanoparticles have already been employed as carriers [177,182]. Virosomes are nanocarriers that mimic the structure of an enveloped virus whose nucleocapsid has been eliminated [177]. Similarly to liposomes, virosomes are an emerging lipid nanomaterial as an FDA-approved nanocarrier consisting of 60–200 nm unilamellar spherical vesicles [183]. Its preparation techniques are simple, economical, and follow similar major steps [177]. This system interacts with host-cell receptors by transporting nucleic acids, inducing humoral and cellular responses via B cells, and endocytosis by other APCs [184]. On the other hand, plant virus nanoparticles (PVNPs) possess the inherent immunostimulatory capacity and have been investigated as immune adjuvants to stimulate an antitumor immune response [185]. Plant viruses such as CPMV (Cowpea mosaic virus) in the form of viral nanoparticles are advantageous for their non-infectivity and lack of toxicity in humans. They have successfully delivered nucleic acid materials by entering cells through alternative pathways or escaping from endosomal vesicles [186]. 4.3.2. Archaea, Bacteria, and Their By-ProductsAs live vectors, bacteria are promising agents for nucleic acid vaccine delivery [176]. The bacterial vector induces a robust immune response due to its natural components, including lipopolysaccharides (LPSs), peptidoglycan, and flagellin, which are recognized by the immune system [187]. Bacteria have specific features called pathogen-associated molecular patterns (PAMPs), recognized by Toll and Nod-like receptors [188]. This introduction induces the native immune response and enhances the adaptive immune response [136]. However, for some species, the precise mechanisms by which bacterial vectors make nucleic acids available in host cells are not yet fully understood [176]. Notably, recombinant and attenuated strains, such as some species of Salmonella, Mycobacterium, Yersinia, Listeria, and Shigella, and non-pathogenic bacteria, such as lactic acid bacteria (LAB), are considered carriers of nucleic acid vaccines [136,176].These organisms also benefit the administration route via the mucosal route that beneficially induces mucosal and systemic immune responses [176]. LABs, for example, are even more suitable because, in addition to being non-pathogenic, withstanding acidic conditions in the gastrointestinal (GI) system, and protecting nucleic acids, they also exhibit probiotic effects [189]. In addition to these, bacterial derivatives can be used as potentially useful nanocarriers for antigen delivery, some as “bacterial ghosts” that possess the ability to stimulate immune responses as potent as those of live bacteria [190]. Other components s
留言 (0)