
記住我
A total of 537 million people live with diabetes globally according to the International Diabetes Federation in 2021. Among them, there are 140.9 million adults (26.2%) were in China, ranking first in the world. In 2021, the prevalence of diabetes in China was 10.6%, slightly lower than in the United States (10.7%) (International Diabetes Federation, 2021). The high prevalence of diabetes in China is, on one hand, due to the increasing aging population; and on the other hand, is related to the lack of physical activities and the refined grain-based diet. Type 2 diabetes mellitus (T2DM), accounting for 90%–95% of all diabetes, is one of the most common chronic metabolic diseases in the world. The main pathophysiological pathogenesis of T2DM is due to Insulin Resistance (IR) and insufficient insulin production of pancreatic ß cells (Cook et al., 2015). Recent research focuses on the human gut microbiota on the intervention of T2DM development. A high-fat, high-sugar diet often leads to a decline in the health of the gut microbiota, which leads to the ecological imbalance in human guts. Gut microbiota imbalance can lead to metabolic dysregulation, including increased IR and elevated levels of inflammation. These are the two key factors in the development of T2DM. Bile acids (BAs) homeostasis is found to be disrupted in T2DM patients, suggesting that BAs interacts with the gut microbiota to regulate carbohydrate, lipid and energy metabolism (Zhang et al., 2018). Meanwhile, BAs regulates the composition of gut microbiota by activating TGR5/FXR receptors, which maintains the stability of intestinal environment, and in turns, improves T2DM (Cipriani et al., 2011; Kakiyama et al., 2013). Furthermore, enzymes synthesized by gut microbiota alter the composition pattern of secondary bile acids (SBAs), which affects the regulation process of carbohydrate and lipid metabolism mediated by various SBAs. This contributes to the improvement of T2DM (Wahlström et al., 2016). Therefore, the dietary intervention of gut microbiota regulating the secretion and metabolism of BAs may help prevent and inhibit inflammatory metabolic disorders, such as T2DM.
Cholesterol is oxidized by enzymes in the liver and becomes the material to produce many different BAs metabolized by gut microbiota. The role of BAs is to facilitate digestion and absorption of fats from food, as well as to activate hormones through different receptors. BAs are the main organic components of bile, which promote the absorption of dietary lipids and maintain cholesterol homeostasis (Jia and Yang, 2019). In addition, BAs act as the significant signaling molecules in the regulation of energy homeostasis to activate different receptors, which play an important role in pathogenesis of T2DM (Perino and Schoonjans, 2022). Recent studies showed that bile acid metabolism altered in T2DM patients, suggesting T2DM was associated with composition and proportion changes of BAs (Sonne et al., 2016; Pandak and Kakiyama, 2019). Alter the bile acid composition may improve blood glucose regulation in T2DM patients. BAs as metabolic regulators participate in the regulation of glucose and lipid metabolism by activating different signaling pathways. Therefore, this article reviewed the findings on the signaling transduction of BAs and their receptors in the improvement of T2DM, the crosstalk with gut microbiota, and their potential therapeutic applications.
2 Synthesis and metabolism of bile acidsBAs are synthesized by cholesterol in the liver and its physiological functions are to participate in the absorption of nutrients and fat-soluble vitamins in the intestine, promote the metabolism of lipids and toxic metabolites, and regulate the glucose metabolism through various mechanisms (Meier and Stieger, 2002). The conversion of cholesterol to BAs is critical for maintaining the cholesterol circulation and preventing the accumulation of cholesterol and triglycerides that cause damage to the liver and other organs. BAs are also signaling molecules and metabolic regulators, which can activate nuclear receptors and G protein coupled receptors (GPCRs) signals, regulate liver lipid and glucose metabolism, and maintain energy homeostasis (Kumar et al., 2016). The enterohepatic cycling of BAs between liver and intestine plays a critical role in nutritional absorption and metabolic regulation. This physiological process is regulated by a complex membrane transport system via nuclear receptors. The disorder of bile acid metabolism can lead to cholestatic liver disease, fatty liver, dyslipidemia, cardiovascular disease, and diabetes (Jia et al., 2021). Several studies have shown the potential value of BAs, BA derivatives and BA sequestrants for the treatment of metabolic liver disease, obesity, and diabetes (Potthoff et al., 2013; Kumar et al., 2016; Guo et al., 2021; Mooranian et al., 2022).
BA synthesis is the main pathway for cholesterol catabolism. The BA production pathways mainly include the classical (or neutral) pathway and the alternative (or acidic) pathway. Cholesterol initiates the neutral (or classical) pathway to synthesize BAs in hepatocytes via cholesterol 7α-hydroxylase (CYP7A1) located on the smooth endoplasmic reticulum. The elevated hepatic cholesterol level induces the formation of oxysterols, which bind to liver X receptor α (LXRα) and activate CYP7A1 transcription. Cholesterol is catalyzed by CYP7A1 to produce 7α-hydroxycholesterol, which is further catalyzed to produce chenodeoxycholic acid (CDCA) and cholic acid (CA). The upregulation of CYP7A1 expression can increase BA synthesis and cholesterol excretion. Subsequently, BAs act as the signaling molecules to activate farnesoid X receptor (FXR) and Takeda G-protein receptor 5 (TGR5) to regulate body metabolism. CYP7A1 is the rate-limiting enzyme of the entire pathway and determines the amounts of BAs. At least 75% of BAs are produced through this pathway under common conditions. In the alternative (or acidic) pathway cholesterol is catalyzed by sterol-27-hydroxylase (CYP27A1) to produce 27-hydroxycholesterol, which is further catalyzed by oxysterol-7α-hydroxylase (CYP7B1) to produce CDCA. Humans and mice produced 9% and 25% of total BAs by alternative pathways, respectively (Wahlström et al., 2016).
BAs synthesized in liver are secreted via the bile, which are mainly reabsorbed in intestine and transported back to liver. After a meal, cholecystokinin secreted by the intestine stimulates the contraction of the gallbladder, and BAs stored in the gallbladder enter the gut. In the enterohepatic cycling, most of BAs (95%) are reabsorbed in the terminal ileum via the apical sodium-dependent bile acid transporter (ASBT) (Jia et al., 2021). The reabsorbed BAs diffuse through the enterocytes to the outside of the basement membrane and circulates through the portal vein to the hepatic sinuses, finally are absorbed by the hepatocytes. Some BAs are reabsorbed in biliary epithelial cells and circulate back to hepatocytes. Small amounts of BAs may leak into the systemic circulation, are reabsorbed as they pass through renal tubules of kidneys, and then return to liver via the systemic circulation (Li and Chiang, 2014). The total amount of BAs and bile salts in the enterohepatic cycling is called the bile acid pool. The bile acid composition in humans is different from that in mice. In humans, the highly hydrophobic bile acid pool consists of approximately 40% CA, CDCA, and 20% DCA. In mice, the highly hydrophilic bile acid pool consists of approximately 50% CA, 50% Tauro-α muricholic acid and Tauro-β muricholic acid (T-αMCA and T-βMCA) (Li and Chiang, 2014). BAs play an important role in glucose and lipid metabolism. Therefore, it may be an effective way to treat T2DM by regulating the composition of BAs via bile acid synthase. The major products of BAs are CDCA and CA. Physiologically, CDCA can dissolve gallstones and ensure smooth enterohepatic cycling of BAs, and CA can promote the digestion and absorption of lipids. CDCA and CA not reabsorbed by ASBT enter the colon, where they bind to glycine or taurine and are stored in the gallbladder. After feeding stimulation, CDCA and CA enter the intestine and are uncoupled and dihydroxylated by gut microbiota to produce SBAs such as ursodeoxycholic acid (UDCA) and lithocholic acid (LCA) (Figure 1) (Wahlström et al., 2016).
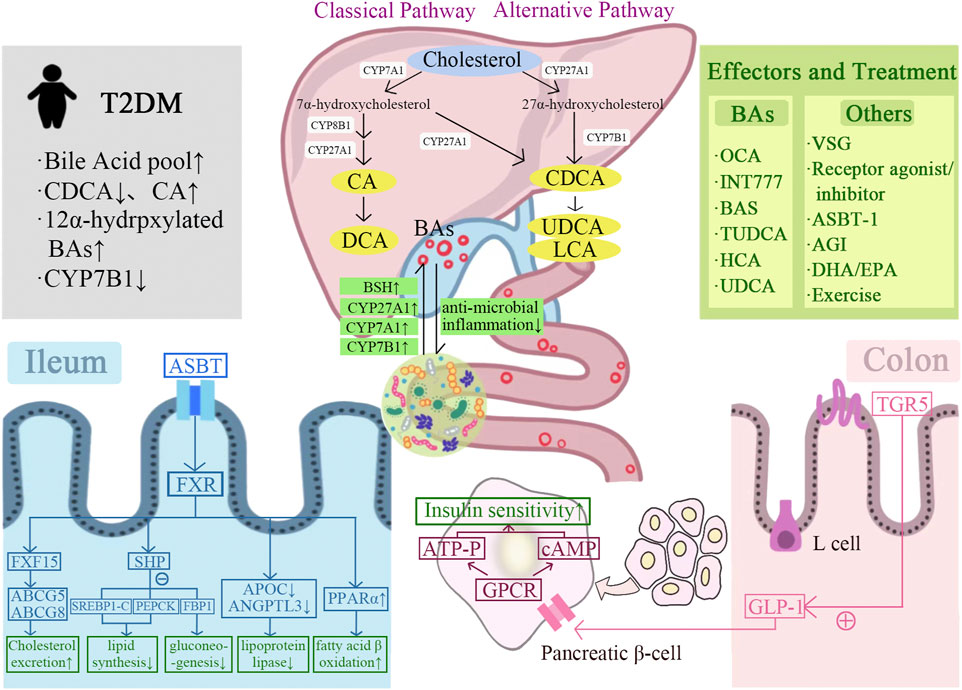
FIGURE 1. Graphical representation of the mechanism of bile acids-gut microbiota crosstalk improves T2DM. BAs are synthesized from cholesterol in the liver via classical and alternative pathways and interact with the gut microbiota. BAs improve insulin sensitivity and T2DM by regulating FXR/TGR5, glucose and lipid metabolism, and GLP-1 secretion. A variety of BAs and their derivatives contribute to the treatment of T2DM, including OCA, INT77, BAS, TUDCA, HCA, and UDCA. In addition, T2DM can also be improved by other treatments, including bariatric surgery, receptor agonists/inhibitors, ASBT-1, AGI, DHA/EPA, and exercise.
3 Bile acids and gut microbiotaThe gut microbiota plays an important role in the regulation of bile acid metabolism. The composition of SBAs can be altered by the enzymes synthesized by gut microbiota, and then affect the regulation of glucose and lipid metabolism mediated by various SBAs (Zhang et al., 2018). The BAs also interact with the gut microbiota, and the composition difference of BAs can explain 37% of the distribution difference of gut microbiota (Chiang and Ferrell, 2019). The physiological functions of BAs are mediated by gut microbiota. The gut microbiota uncouples conjugated BAs to free BAs via bile salt hydrolases, and then dehydrogenates or dehydroxylates the free BAs to SBAs, such as converting CA to deoxycholic acid (DCA) and CDCA to LCA. DCA is reabsorbed in the colon and circulates to the liver with CA and CDCA. A bile acid pool of about 3 g, consisting of about 40% CA, 40% CDCA, 20% DCA, and a trace amount of LCA, was recovered 4–12 times per day. The remaining 5% of BAs that do not enter the enterohepatic cycling, part of which is catabolized by gut microbiota to generate SBAs, which are passively reabsorbed by the small intestine and colon; the other part is excreted through feces (Chiang and Ferrell, 2019; Ticho et al., 2019). The gut microbiota involved in converting primary BAs into SBAs are Bacteroides, Clostridium, Eubacterium, Lactobacillus and Escherichia (Ticho et al., 2019).
3.1 Gut microbiota and their metabolitesThe basic functions of gut microbiota are to participate in the regulation of intestinal metabolites. It is estimated that more than 8,000 non-nutritive compounds exist in the human gut, most of which cannot be digested by human digestive enzymes (Wishart, 2019). The carbohydrates, lipids, proteins, and complex dietary fibers are fermented and catabolized by gut microbiota in the colon to produce functional metabolites, such as short-chain fatty acids (SCFAs), SBAs, and hormones. The colon is the primary site of fermentation, but gut microbiota from other sites, such as Lactobacillus and Streptococcus in small intestine, also participate in the regulation of nutrient metabolism (Liang et al., 2021). The dysbiosis of gut microbiota leads to changes of many metabolites, of which the type and concentration affect the host-sensing receptor responses (Chen et al., 2019).
3.2 Gut microbiota regulates bile acids3.2.1 Deconjugation of gut microbiota regulates the composition of bile acid poolThe deconjugation of BAs by gut microbiota is carried out in the small intestine by bacteria with bile salt hydrolase (BSH) activity, thus maintaining normal levels of deconjugated bile acids and cholesterol in the circulation (Chiang, 2013). Metagenomics studies have shown that all major bacteria and archaea in the human intestine express functional BSH, including Lactobacillus, Bifidobacterium, Clostridium, Bacteroides, etc. (Odermatt et al., 2011). BSH enriched in gut microbiota is related to the increased resistance to bile toxicity. The antibiotic use and the dysbiosis of gut microbiota are associated with long-term changes in gut microbiota composition and bile acid metabolism. BSH activity is necessary to accelerate cholesterol catabolism by increasing the excretion of bile acids (Supplementary Table S1) (Chiang, 2013). The study showed that mice treated with 3 days of oral antibiotics exhibit impaired bile acid metabolism similar to germ-free animals (Miyata et al., 2009). In summary, gut microbiota and its deconjugation function led to changes in the composition of bile acid pool that contribute to the maintenance of cholesterol homeostasis.
3.2.2 Gut microbiota regulates the expression of bile acid synthaseThe gut microbiota regulates bile acid production by regulating the expression of the rate-limiting enzymes cholesterol-7α-hydroxylase (CYP7A1), CYP27A1, and CYP7B1 in the bile acid production pathway (Wahlström et al., 2016). Excessive amount of cholesterol is removed from the peripheral system, including lipid-filled macrophages, via the reverse cholesterol transport (RCT) pathway. During this process, cholesterol is converted to BA by CYP7A1, which is subsequently excreted in the feces (Chambers et al., 2019). By crossing Cyp7A1 and Cyp27A1 gene deficient mice, the total amount of BA in the double-gene knockout mice was reduced more than 85%, demonstrating that the deletion of the rate-limiting enzyme in the BA production pathway caused the decrease of BA synthesis (Rizzolo et al., 2021). It was shown that the number of 7-dehydroxylase-producing bacteria was significantly reduced in the intestine of germ-free or antibiotic-treated mice, and the levels of glycine-conjugated BAs and SBAs were also significantly reduced, while the levels of taurine conjugated bile acid (TBA) were significantly increased (Wahlström et al., 2016). In addition, the antibiotic treatment can upregulate the expression of CYP7A1 and increase the production of CDCA and CA by inhibiting the expression of fibroblast growth factor 15 (FGF15) (Sayin et al., 2013; Chambers et al., 2019). All the above findings indicated gut microbiota played a regulatory role in BAs synthesis (Figure 1).
3.2.3 Probiotics regulates bile acid synthesisProbiotics are involved in the regulation of bile acid synthesis and metabolism during the interaction of bile acids and gut microbiota. The currently known mechanisms include: 1) regulation of BSH activity Bifidobacterium and Lactobacillus were identified as probiotics with BSH activity, among which Bifidobacterium breve and Lactobacillus plantarum LA3 strains had the highest BSH activity (Öner et al., 2014). BSH catalyzes the conversion of primary BAs to SBAs, leading to reduced reabsorption of BAs in the enterohepatic circulation and easier excretion of SBAs from the gut, thereby promoting bile acid synthesis and LDL-cholesterol clearance (Costabile et al., 2017; Pushpass et al., 2021). 2) assimilation of cholesterol Probiotics lower cholesterol levels by binding cholesterol to their cell membranes and converting it into coprostanol (Lye et al., 2010). 3) activation/inhibition of FXR DegGirolamo et al. found that the bile acid composition was significantly altered in mice after gavage with the probiotic mixture VSL#3 for 21 days. The high levels of BSH activity inhibited FXR response in the gut-liver axis and resulted in a decrease in the ratio of conjugated BAs/free BAs in feces (Degirolamo et al., 2014). In contrast, Choi et al. found that the addition of Lactobacillus. Curvatus and Lactobacillus. Plantarum to a high-fat diet for 6 weeks increased the intestinal FXR expression in mice (Inagaki et al., 2005). Martoni et al. found that supplementation with Lactobacillus reuteri activated FXR as well as increased circulating bile acid levels (Martoni et al., 2015).
Akkermansia muciniphila (Akk) accounts for 1%–5% of the human gut microbiota and is considered to be a new generation of beneficial microorganisms (Zhang et al., 2019). Akk treatment has been verified to improve symptoms of metabolic disorders, including IR, metabolic endotoxemia, and adipose tissue inflammation (Zhao et al., 2017; Depommier et al., 2019). Several studies revealed how Akk regulated signal transduction and energy expenditure to achieve its metabolic effect mechanisms (Grander et al., 2018; Sheng et al., 2018). Akk supplementation reduced the synthesis and transport of fatty acid in the liver and muscle, and attenuated chronic low-grade inflammation by inhibiting the lipopolysaccharide (LPS)-binding protein (LBP) signaling pathway (Zhao et al., 2017). Another study found that Akk treatment increased hepatic absorption of cholesterol and bile acid metabolism, and improved the enterohepatic cycling of bile acid metabolism. In turn, the enhanced bile acid metabolism facilitated the remodeling of gut microbiota composition and the colonization of Akk (Rao et al., 2021). In addition, the activation of oxidative stress and the induction of intestinal cell apoptosis damage the intestinal barrier, leading to the development of diseases such as inflammatory bowel disease (IBD), obesity and T2DM (Aviello et al., 2019; Franzosa et al., 2019; Ni et al., 2021). Akk treatment effectively increased lipid oxidation, ameliorated lipid accumulation-induced intestinal oxidative stress and cell apoptosis, and maintained them at normal levels (Rao et al., 2021). These findings further confirm the potential of Akk in the treatment of metabolic disorders.
Clearly, we need to provide more details through human experiments to elucidate the mechanisms behind the beneficial effects of specific probiotic-bile acid interactions on glycolipid metabolism.
3.3 Bile acids regulate gut microbiota via farnesoid X receptor/Takeda G-protein receptor 5BAs is an important regulator of gut microbiota balance. Low bile acid levels appeared to reduce the number of Gram-positive bacteria. Reduced bile acid levels in the intestine appear to favor Gram-negative bacteria in the gut microbiota, some of which are potentially pathogenic bacteria that produce strong antigenic lipopolysaccharides. In contrast, elevated bile acid levels in the intestine favored the transformation of Gram-positive bacteria Firmicutes, including bacteria that caused dehydroxylation of primary BAs to harmful SBAs. The complex and significant changes in gut microbiota at the phylum level were observed in rats fed CA-containing diet. Compared with the control group, the proportion of Firmicutes expanded from 54% to 93%–98%, and Clostridium expanded from 39% to about 70% (Islam et al., 2011). The SBAs influenced by gut microbiota activate FXR and TGR5 more strongly than the BAs (Long et al., 2017). The BAs have a direct antibacterial effect on the gut microbiota. The SBAs, DCA, is more effective as an antibacterial agent than CA due to its stronger hydrophobicity and detergency on bacterial membranes (Chiang, 2013). Meanwhile, BAs also regulate host immune response through FXR-induced antibacterial peptides or by acting on FXR/TGR5. TGR5 has been shown to be involved in regulating the stability of the intestinal environment. The deletion of TGR5 is manifested by increased intestinal permeability and susceptibility to intestinal inflammation. The overproduction of pro-inflammatory cytokines in FXR−/− mice caused intestinal inflammation. The activating of FXR can prevent the development of inflammation in mice with colitis (Figure 1) (Cipriani et al., 2011).
4 Bile acids and type 2 diabetes mellitus4.1 The alterations of bile acid metabolism in type 2 diabetes mellitusThe physiopathology of T2DM is characterized by fasting hyperglycaemia, IR, and postprandial hyperglycemia (Grandl and Wolfrum, 2018). Early and recent studies suggested the size and/or composition of bile acid pool changed in patients with T2DM. The size of the bile acid pools in insulin-treated and untreated T2DM patients were different. The content of CDCA is decreased and the synthesis of CA is increased in bile acid pool in T2DM patients. In human studies, the magnitude of change in postprandial plasma BA levels was positively correlated with dietary fat content. Furthermore, compared to normoglycemic subjects matched with age, sex, and BMI, the T2DM patients had increased total plasma BAs, mainly due to the increased glycine-binding BAs, DCA, and UDCA during oral glucose and dietary tolerance experiments (Sonne et al., 2016). The oral glucose tolerance test was performed on 2952 T2DM patients with normal fasting serum total bile acids (S-TBAs). Results showed that the elevated fasting S-TBAs levels within the normal range were significantly associated with reduced fasting and systemic insulin sensitivity, impaired islet β-cell function and increased blood glucose after glucose stimulation in T2DM patients, suggesting that the regulation of fasting S-TBAs may be a therapeutic target for T2DM (Wang et al., 2020). The plasma concentration of 12α-hydroxylated bile acid was higher in obese and T2DM patients than that in healthy individuals. The transcription level of CYP7B1 was decreased in mice model of IR and T2DM, as well as in obese and T2DM patients (Figure 1) (Chen et al., 2016; Pandak and Chiang, 2019). The studies clearly supported the opinion of altered bile acid metabolism in patients with T2DM.
4.2 Bile acids improve insulin sensitivity through receptor-mediated regulation of glucose and lipid metabolismThe BAs can activate a variety of nuclear and membrane receptors. The nuclear receptors mainly include FXR, pregnane X receptor (PXR), steroid and xenobiotic receptor (SXR), constitutional androstane receptor (CAR) and VDR. The membrane receptors mainly include TGR5, sphingosine-1 phosphate receptor 2 (S1PR2) (Ticho et al., 2019). FXR and PXR are abundantly expressed in the liver and intestine. Moreover, they regulate insulin synthesis and glucose-induced secretion in the pancreatic β-cell. VDR is widely distributed in most tissues including pancreas, skin, intestine and liver (Kumar et al., 2016).
4.2.1 Intermediation of nuclear receptorFXR is the major nuclear receptor for BAs to exert the physiological effect. As the first natural endogenous receptor for BAs, its role in the homeostasis of glucose and lipid metabolism in vivo has been confirmed in several studies (Noel et al., 2016). FXR activation improves lipid metabolism and insulin sensitivity in Zucke (fa/fa) obese rats, ob/ob mice, and db/db diabetic mice (Cariou et al., 2006; Cipriani et al., 2010), suggesting that FXR agonists could be used in the treatment of diet-induced T2DM as a pharmaceutical strategy. FXR activation can reduce hepatic lipoprotein synthesis by inducing the gene expression of lipoprotein metabolism or scavenging. At the same time, the expression of triglyceride synthesis genes was inhibited to reduce plasma triglyceride and cholesterol levels (Shapiro et al., 2018). The BAs induce the expression of the target gene SHP by activating hepatic FXR. The SHP reduced hepatic lipid synthesis by inhibiting the expression of the transcription factor sterol regulatory element binding transcription factor-1c (SREBP-1c) and its downstream hepatic lipid synthesis genes (Ahmad and Haeusler, 2019). In addition, the expression of SHP can also reduce hepatic gluconeogenesis by inhibiting phosphoenolpyruvate carboxykinase and fructose bisphosphatase-1 (Mathur et al., 2021). Compared to wild-type mice, the fasting glucose tolerance was significantly impaired in FXR knockout (FXR KO) mice. And the intraperitoneal glucose tolerance and blood glucose fluctuations were significantly improved by injecting the FXR agonist GW4064 in ob/ob and db/db mice (Supplementary Table S1) (Han et al., 2021). The FXR agonist Fexaramine significantly improved the blood glucose levels and reduced the diet-induced weight gain (Fang et al., 2015; Pathak et al., 2018). Furthermore, FXR activation can lead to decreased expression of apolipoprotein C (APOC) and angiopoietin-like protein 3 (ANGPTL3), thereby inhibiting the activity of lipoprotein lipase. In addition, FXR activation induces the expression of peroxisome proliferator-activated receptor α (PPARα), which promotes fatty acid β-oxidation (Li and Li, 2017). FXR was activated by BAs to induce the production of FGF15, which changed the ratio of primary BAs to SBAs, enhanced the hydrophilicity of bile, and then allowed cholesterol to be discharged into the intestinal lumen by ATP-binding cassette transport G5 (ABCG5) and ATP-binding cassette transport G8 (ABCG8), resulting in more than 60% of the absorbed cholesterol to be excreted through the intestinal lumen (de Boer et al., 2017).
Several studies have found that the inhibition of FXR also has a significant effect on body glucose and lipid metabolism. Whole-body FXR KO mice and mice lacking FXR in the intestine showed significantly improved oral glucose tolerance and reduced body weight (Chávez-Talavera et al., 2017; Jiang et al., 2015; Trabelsi et al., 2015; Xie et al., 2017). The mechanisms by which FXR inhibition improves glucose and lipid metabolism include: 1) The intestinal FXR-mediated serum ceramide production affects hepatic phosphoenolpyruvate carboxykinase (PEPCK) activity and hepatic gluconeogenesis, and regulates glucose-6-phosphatase (G6P) expression; 2) FXR-dependent inhibition of glucagon-like peptide 1 (GLP-1) precursor increases, thereby promoting GLP-1 production. GLP-1 enhances the glucose-induced insulin secretion and increases the insulin sensitivity in skeletal muscle, adipose tissue, and liver; 3) FXR-dependent inhibition of hepatic glycolytic gene expression increases; 4) Increase the level of glucose phosphorylation in intestinal epithelial cells and delay intestinal glucose absorption (Figure 1). In conclusion, the FXR-mediated regulatory mechanism of glucose and lipid metabolism deserves further in-depth study.
In addition to FXR, VDR can also be activated by LCA and participate in the regulation of glucose and lipid metabolism by affecting pancreatic islets, macrophages, or endothelial cells (Oh et al., 2015; Ni et al., 2016). However, these BAs are difficult to be absorbed into cells. Compared with the activated type of vitamin D, these BAs have a weaker ability to bind the nuclear receptor VDR. Therefore, higher levels of LCA are required to activate the VDR in the body and most occurs in the presence of vitamin D deficiency. At present, the mechanism of BAs-VDR signaling on the homeostasis of glucose and lipid metabolism still needs to be further studied.
4.2.2 Intermediation of membrane receptorTGR5 is the most intensively studied membrane-bound G protein-coupled receptor, which is expressed in tissues of various metabolic organs, including the intestine, liver, adipose tissue, and muscle. BAs is the only known endogenous ligand for TGR5 (Xiao et al., 2020). The roles of TGR5 in improving glucose and lipid metabolism mainly include: 1) promote hepatic glycogen synthesis and insulin sensitivity; 2) increase insulin secretion from the pancreas; 3) promote energy expenditure, especially in liver, brown adipose tissue, and muscle; 4) facilitate thermogenesis, leading to weight loss; 5) regulate satiety in the brain (Ðanić et al., 2018). After BAs binding, TGR5 activation is related to intracellular accumulation of cyclic adenosine monophosphate (cAMP), adenylate cyclase activation, and calcium mobilization (Duboc et al., 2014). Due to its widespread tissue distribution, BA-activated TGR5 receptors are involved in various regulatory processes, ranging from the activation of macrophage to the regulation of glucose metabolism. BAs reduce the production of inflammatory cytokines through TGR5 activation in immune cells. BAs increase the energy expenditure of skeletal muscle and brown adipose tissue through iodothyronine deiodinase (D2), thereby preventing obesity (Castellanos-Jankiewicz et al., 2021). BAs regulate postprandial insulin release and blood glucose concentration by activating TGR5 in enteroendocrine L cells and stimulating the release of incretin GLP-1 (Kuhre et al., 2016). It has also been shown that TGR5 activation promotes glucose-induced insulin release from pancreatic β-cells in a cAMP- and calcium-dependent manner, meanwhile, avoiding glucagon release from α-cells (Figure 1) (Huang et al., 2019).
4.3 Bile acids promote insulin secretion by regulating GLP-1Although only 1% enteroendocrine cells in the intestinal epithelium, the intestine is the largest endocrine organ due to its length. The enteroendocrine K cells secrete the glucose-dependent insulinotropic polypeptide (IP) to promote insulin release after food intake (Trabelsi et al., 2017). GLP-1 secreted by the enteroendocrine L cells, is a gastrointestinal hormone released in response to feeding that inhibits gastric emptying, appetite (Tomaro-Duchesneau et al., 2020), and glucagon secretion by exerting an incretin effect (Hira et al., 2020). After GLP-1 binds to the GLP-1 receptor on the islet β-cell membrane, it phosphorylates K+−ATPase. Consequently, the cell membrane is depolarized, K+ channels close, Ca2+ channels open, and Ca2+ influx stimulates insulin secretion from β-cells, resulting in the closure of K+ channels, the depolarization of the cell membrane, the opening of Ca2+ channels, and the influx of Ca2+, stimulates insulin secretion from β-cells. Meanwhile, by binding to the receptor, GLP-1 activates adenylate cyclase (AC) on the cell membrane, which converts ATP to cAMP. As a second messenger, cAMP activates protein kinase A (PKA) and cAMP-regulated guanine nucleotide exchange factor II (GEF II) to promote insulin secretion (Gomez et al., 2002).
BAs can regulate GLP-1 secretion and proglucagon gene expression. It was showed that both TGR5 and FXR were expressed in L cells. TGR5 is located on the basolateral of L cells, which mediated the BAs-induced GLP-1 secretion (Harach et al., 2012). The high-fat-fed TGR5 transgenic mice (TGR5-tg mice) exhibited improved glucose tolerance, whereas TGR5-KO mice fed with high fat diet had worse glycemic status. After oral glucose tolerance test (OGTT), TGR5-tg mice fed with high fat diet showed higher GLP-1 and insulin levels than TGR5-WT mice. It suggests that the improvement in glucose metabolism is achieved by GLP-1-mediated incretin action. TGR5/GLP-1 pathway is important in the improvement of blood glucose by BAs. Through TGR5 activation, BAs also initiate cAMP and its downstream related signaling pathways, type 2 iodothyronine deiodinase (D2), Ca2+/calcineurin-activated nuclear factor of activated T cell 3 (NFAT 3), proprotein convertases 1/3 (PC 1/3) (Morimoto et al., 2016), or mammalian target of rapamycin (mTOR) (Zhai et al., 2018), which stimulate the secretion of GLP-1 from intestinal L cells, promote insulin secretion (Cao et al., 2016; Lasalle et al., 2017), and improve the pancreatic β-cell function and blood glucose homeostasis, thereby improving T2DM. In addition, the activation of intestinal TGR5 also promotes the release of peptide tyrosine tyrosine (PYY), which reduces appetite (Bala et al., 2014).
Conversely, the activation of FXR inhibits the ileal proglucagon gene expression and GLP-1 secretion by inhibiting glycolysis and carbohydrate response element binding protein (ChREBP) activity in L cells (Trabelsi et al., 2015). The deletion of FXR gene improved glucose metabolism by enhancing peripheral glucose handling and increasing adipose tissue insulin sensitivity in hyperphagic ob/ob mice. Nevertheless, this effect was not observed in hepatocytes from ob/ob mice lacking the FXR gene (Prawitt et al., 2011), thus demonstrating the beneficial effect of FXR gene deletion in extrahepatic tissues on glucose homeostasis.
In conclusion, BAs have beneficial effects on T2DM by regulating GLP-1 to activate GPCRs, reducing food intake, improving insulin sensitivity, inhibiting fat accumulation, and reducing systemic inflammation. The reduction of BAs may reduce these beneficial effects and promote the development of IR and T2DM (Figure 1).
4.4 Bile acids improve insulin sensitivity by activating FGF15/19 and FGF21 pathwaysThe feeding-induced fibroblast growth factor 19 (FGF19) and the fasting-induced fibroblast growth factor 21 (FGF21) are metabolic regulatory hormones with different physiological functions, but both have similar effects in improving energy metabolism and insulin sensitivity (Kuro-O, 2019). The fibroblast growth factor 15 (FGF15) in rodents and the FGF19 in humans are highly expressed in ileal epithelial cells and can be secreted by BAs-activated FXR or TGR5, which is an important endocrine hormone that regulates hepatic bile acid synthesis and host glucose and lipid metabolic homeostasis (Somm and Jornayvaz, 2018). FGF15 can affect the peroxisome proliferator-activated receptor γ (PPARγ) pathway through hepatic fibroblast growth factor receptor 4 (FGFR4), reducing fat accumulation and cholesterol, triglyceride synthesis. FGF15 and FGF19 can reduce hepatic gluconeogenesis by regulating the dephosphorylation of the gluconeogenic transcription factor cAMP responsive element binding protein 6 (CREB6) (Potthoff et al., 2011). On the other hand, they activate the phosphorylation cascade of extracellular signal-regulated kinase (ERK)-glycogen synthase kinase a/p (GSK a/p) to promote hepatic glycogen synthesis (Kir et al., 2011). In hypothalamic neurons, FGF15 or FGF19 activates the ERK signaling pathway to reduce insulin-independent glucose levels (Lan et al., 2017; Liu et al., 2018). In addition, they can increase metabolic rate and reduce body weight by increasing β⁃Klotho-dependent sympathetic activity in brown adipose tissue (Lan et al., 2017). The plasma levels of FGF19 were significantly decreased in T2DM and obese patients, while injection of recombinant FGF19 protein significantly improved metabolic disorders in db/db mice and DIO mice (Guo et al., 2022). FGF21 is a nutrient-sensitive hormone produced in hepatocytes, which can be induced by BAs. FGF21 improves insulin sensitivity through several mechanisms. In the liver, FGF21 inhibits the mammalian target of rapamycin complex 1 (Mtorc1) signaling pathway and increases hepatic insulin sensitivity (Pathak and Chiang, 2019). In adipose tissue, FGF21 promotes fatty acid oxidation by activating PPARγ, thereby improving insulin sensitivity (Wu et al., 2020). FGF21 also stimulates adiponectin (APN) secretion in adipose tissue, thereby reducing ceramide and blood glucose, and enhancing insulin sensitivity in DIO mice (Figure 2A) (Holland et al., 2013).
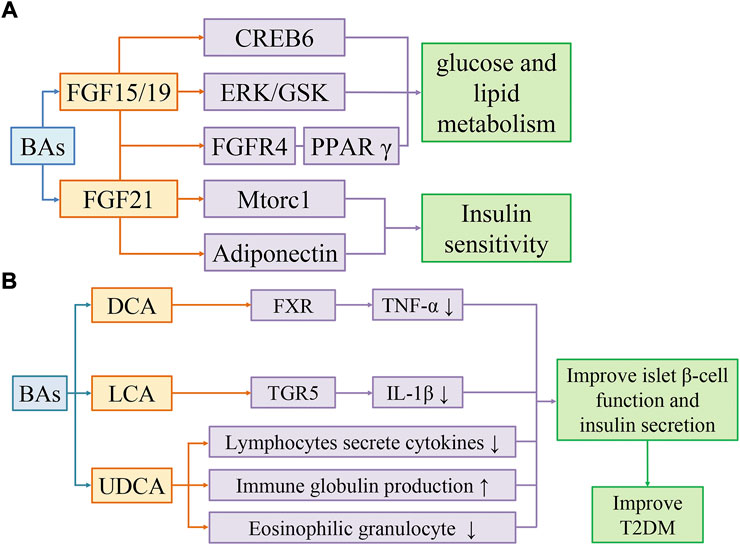
FIGURE 2. Bile acids activate FGF15/19 and FGF21 pathways to improve insulin sensitivity (A). Bile acids improve T2DM by reducing inflammation (B). (A) BAs improve glucose and lipid metabolism through FGF19/CREB6, FGF19/EPK/GSK, and FGF19/FGFR4/PPARγ pathways, and improve insulin sensitivity through FGF21/Mtorc1 and FGF21/Adiponectin pathways. (B) DCA activates FXR to reduce TNF-α levels. LCA activates TGR5 to reduce IL-1β levels. UDCA regulates the immune system by reducing cytokine secretion by lymphocytes, producing immunoglobulins, and inhibiting eosinophil activation and degranulation. Secondary bile acids can improve T2DM by restoring islet β-cell function and insulin secretion affected by inflammation.
4.5 Bile acids improve T2DM by reducing the levels of inflammatory cytokinesIn individuals with obesity, T2DM and MAFLD, the chronic low-grade inflammation is usually accompanied by metabolic changes in tissues and organs, which is characterized by recruitment of immune cells, abnormal production of cellular inflammatory cytokines and acute phase reactants, and activation of inflammasome (Weichhart et al., 2015). In inflammatory states, gut microbiota converts bile salts to BAs and SBAs inefficiently (Lloyd-Price et al., 2019). Compared with healthy subjects, patients with IBD have an imbalance of gut microbiota, lower concentrations of SBAs and higher concentrations of conjugated bile acids in feces and blood circulation (Duboc et al., 2013).
BAs inhibits the induction of pro-inflammatory genes by inhibiting the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway (de Aguiar Vallim et al., 2013). SBAs such as DCA and LCA can inhibit TNF-α production in macrophages through FXR. FXR−/− mice showed an increased risk of colitis and cancer compared to wild-type mice (Renga et al., 2013). SBAs, especially LCA, inhibited IL-1β production in macrophages via TGR5 (Guo et al., 2016). The clinical trials have shown that the elevated IL-1β in circulating system is a risk factor for T2DM, so the inhibition of IL-1β may be a promising therapeutic strategy (Zhao et al., 2014). Furthermore, SBAs can block the hyperactivation of the inflammasome in T2DM (Guo et al., 2016). Gut microbiota such as Ruminococcus can synthesize UDCA. As a SBA, UDCA can regulate the immune system by reducing cytokine secretion by lymphocytes, producing immunoglobulin, and inhibiting eosinophil activation and degranulation (Hosseinkhani et al., 2021).
TGR5 and FXR are expressed in a variety of immune cells as two major receptors for BA. TGR5 has anti-inflammatory effects and reduces the production of inflammatory cytokines in monocytes, macrophages, and dendritic cells (Hu et al., 2022). Activated TGR5 inhibits NLRP3 inflammasome activation via the TGR5-cAMP-PKA axis, thereby attenuating high-fat diet-induced elevated glucose tolerance, IR, and inflammatory responses (Hu et al., 2021). Secondly, the activation of TGR5 by BA can reduces the CCAAT/enhancer binding protein ß (C/EBPβ)-mediated inflammatory infiltration of macrophages in white adipose tissue and increase energy expenditure (Velazquez-Villegas et al., 2018). On the other hand, FXR deficiency impairs intestinal barrier function, which may enhance hepatic LPS secretion and inflammatory responses.
Overall, BAs have multiple signaling regulatory roles in regulating the immune system and inflammation. And the low-grade inflammation has been considered as a potential cause of IR. Adipose tissue itself releases many cytokines. Therefore, as the increase of adipose tissue is accompanied by the accumulation of various metabolic stresses, the cytokines released from adipose tissue will “overflow”, resulting in an imbalance between insulin-sensitive cytokines (adiponectin, leptin) and pro-inflammatory cytokines (RBP4, resistin, IL-6, TNF). However, it is worth noting that IR can also occur without an inflammatory response. The studies found that rats and humans exhibited IR before an inflammatory response (Roden and Shulman, 2019). Following the intervention of dietary palm oil (PO) composed of saturated fatty acids, the hepatic γATP and HCL concentrations were increased in mice, which simultaneously induced lipid oxidation and IR, and the human subjects developed systemic IR. The plasma free fatty acid (FFA) concentrations were significantly increased in humans and mice after PO intake, but there were no changes in circulating inflammatory markers or adipokines, such as TNF-α, IL-6, and fetuin-A (Figure 2B) (Hernández et al., 2017).
4.6 Effects of 12α-hydroxylated bile acids and non-12α-hydroxylated bile acids on insulin sensitivityInsulin is the only hormone in the body that reduces blood glucose and promotes the synthesis of glycogen, fat, and protein simultaneously, which plays a crucial role in glucose and lipid metabolism. Abnormal insulin sensitivity is one of the important reasons for the disorder of glucose and lipid metabolism in vivo. Several studies analyzed the relationship between bile acid concentrations and insulin sensitivity. The results showed that IR was associated with the concentrations of primary bile acids and 12α-hydroxylated bile acids (Haeusler et al., 2013; Legry et al., 2017).
12α hydroxylated bile acids are mainly catalyzed by cytochrome P450 family 8 subfamily B member 1 (Cyp8b1). The plasma concentrations of 12α-hydroxylated bile acids were higher in obese and T2DM patients than in healthy people (Kaur et al., 2015). In DIO mice, knockdown of the Cyp8b1 gene reduced body weight, decreased postprandial insulin levels, and improved glucose tolerance, despite no changes in thermogenesis and oxygen consumption. The fecal lipid content was higher in Cyp8b1 KO mice indicated that the lipid absorption capacity was reduced in the intestine. The number of ileal L cells was increased and the contents of GLP-1 and PYY were increased in the ileal epithelium in Cyp8b1 KO mice, which may be due to impaired lipid absorption and lipid receptors activation. The lipidomic results showed that knockdown of Cyp8b1 increased the excretion of fecal lipids such as monoacylglycerol, which is an activator of the lipid receptor G protein coupled receptor 119 (GPR119). GPR119 is mostly distributed on the surface of enteroendocrine cells, especially L cells, and mediates lipid-induced GLP-1 secretion. Cyp8b1 KO mice had higher levels of ileal GLP-1 and PYY contents, slowed gastric emptying, and decreased feed intake and body weight, which could be relieved by knocking out GPR119. The inefficient hydrolysis of triglyceride in Cyp8b1 KO mice results in the entry of unabsorbed lipids into the small intestine and colon, which activates GPR119 to induce the release of GLP-1 and PYY, slow gastric emptying, and reduce food intake (Higuchi et al., 2020). Thus, changes in the content of 12α-hydroxylated bile acids can affect lipid absorption, intestinal hormone secretion, and lipid receptor activation, thereby affecting insulin sensitivity, and glucose and lipid metabolism. In addition, 12α-hydroxylated bile acids also inhibit hepatic PPARα-FGF21 signaling pathway by activating intestinal FXR to generate ceramide and FGF15, thus leading to IR (Chiang and Ferrell, 2019; Pathak and Kakiyama, 2019).
BAs can regulate intestinal lipid receptors in multiple ways. It has been proved that BAs promotes the hydrolysis and absorption of dietary fat, which is an endogenous mechanism to prevent satiety induction by enteroendocrine cells (Higuchi et al., 2020). The bile acid composition of Cyp8b1 KO mice is altered with a decrease in 12α-hydroxylated bile acids and an increase in non-12α-hydroxylated bile acids, which induces impaired jejunal oleoylethanolamide production, slow gastric emptying, and increased satiety after feeding (Haeusler et al., 2013). The non-12 hydroxylated bile acids resist the obesity phenotype in mice through TGR5-mediated activation of brown adipose tissue (BAT) and upregulation of uncoupling protein 1 (UCP1) expression (Wei et al., 2020). Dieting significantly reduced the proportion of non-12α-hydroxylated secondary bile acids such as UDCA and LCA in mice. Calorie restriction (CR) diets have been recognized as a factor in promoting health, prolonging lifespan, and preventing the development of metabolic diseases (Kökten et al., 2021). However, long-term weight loss is challenging due to the complex interaction between hormones and behavior (Liu et al., 2022), which often results in gradual or rapid weight regain after CR intervention (Marlatt et al., 2017). Recently, study by Mengci Li showed that the beneficial bacteria Parabacteroides distasonis in mice was significantly reduced during fasting or CR. The supplementation of non-12α hydroxylated bile acids UDCA and Parabacteroides distasonis to high-fat diets prevented weight gain and improved glucose and energy metabolism. Mice can reduce weight rebound by supplementation with non-12α hydroxylated bile acids or Parabacteroides distasonis (Li et al., 2022).
4.7 Probiotic treatment improve T2DM by regulating Cyp8b1 geneProbiotic metabolites regulate the expression and activity of intestinal nuclear receptors (NRs), including VDR, FXR, and PPARs, whose activity extends to the cerebral cortex (Distrutti et al., 2014). Regulation of gut microbiota by administration of the probiotic cocktail VSL#3 increased fecal bile acid excretion in mice, as well as de novo hepatic bile acid synthesis, associated with increased BSH transcription and fecal enzyme activity. VSL#3 is a probiotic formulation consisting of Lactobacillus acidophilus, Lactobacillus paracasei, Lactobacillus bulgaricus, Lactobacillus plantarum, Bifidobacterium breve, Bifidobacterium infantis, Bifidobacterium longum, and Streptococcus thermophilus. VSL#3 significantly altered the composition of fecal microbiota in mice administered by gavage at a dose of 50 × 109 CFU/d for 21 days, increasing the number of Firmicutes and Actinomycetes, while decreasing Bacteroides, and Bacillus Proteus. VSL#3 increases the expression of Cyp7a1 gene by down-regulating the expression of FGF15 in the ileum, activates GPCR, promotes the secretion of GLP-1, and increases insulin sensitivity (Supplementary Table S1) (Jena et al., 2020).
4.8 Future directions and therapeutic approaches for T2DM based on the bile acids signalingThe incidence of T2DM is increasing worldwide. T2DM patients required long-term drug treatment with the high risk of cardiovascular disease and other complications. T2DM caused a huge medical burden to individuals and society. Therefore, there is an urgent need to explore effective approaches to prevent and improve blood glucose and blood lipid levels in T2DM patients. At present, the improvement of T2DM based on the interaction of BAs and gut microbiota shows the prospect of effective intervention through bile acid signaling in the future (Massey and Brown, 2021). The potential targeting signaling pathways and targets of BAs and their derivatives in improving T2DM include: FGF15/19 regulates hepatic glucose and lipid metabolism by PPARγ, ERK signaling pathways and CREB6 dephosphorylation (Potthoff et al., 2011); FGF21 enhances insulin sensitivity by Mtorc1 signaling pathway (Pandak and Chiang, 2019) and stimulating APN secretion (Holland et al., 2013). The results suggest that fibroblast growth factor and its related pathways contribute to glycemic control and reduce lipid synthesis and accumulation, which may become a worthy intervention on T2DM. In addition, BAs also reduce the secretion of inflammatory cytokines such as TNF-α (Renga et al., 2013) and IL-1β (Guo et al., 2016), improve the function of islet β-cells, and increase insulin secretion by regulating TGR5 and FXR in the liver and intestine (Cao et al., 2016; Lasalle et al., 2017). Studies have shown that FXR antagonists and TGR5 agonists in the intestine can improve glycemic control in rodents with T2DM (Zheng et al., 2021). TGR5 and FXR become potential targets for reducing insulin resistance and improving T2DM. Therefore, the development of gut-specific FXR antagonists and TGR5 agonists may be a promising approach for the treatment of hyperglycemia, but the long-term impact of this approach needs to be evaluated (Shapiro et al., 2018).
5 Therapeutic effects of bile acids and their derivatives on type 2 diabetes mellitus5.1 Obeticholic acidObeticholic acid (OCA) is a derivative of the primary bile acid CDCA and a selective FXR agonist with anti-cholestatic activity and inhibit intestinal inflammation (Fiorucci et al., 2011). In animal studies, OCA was able to increase insulin sensitivity, inhibit gluconeogenesis and adipogenesis, and have anti-inflammatory and anti-fibrotic effects. OCA also ameliorated high-fat diet-induced obesity and IR in mice, and fatty liver and IR in Zucker (fa/fa) rats. OCA can antagonize NF-κB-stimulated liver inflammation, regulate innate immunity in animal models of colitis, inhibit IBD, and protect intestinal barrier (Guo et al., 2021). OCA has entered phase II clinical trials in patients with type 2 diabetic metabolic fatty liver disease, with improvements in insulin sensitivity, hepatic gamma-glutamyl transferase levels, and weight loss (Mudaliar et al., 2013).
5.2 6α-ethyl-23(S)-methyl cholic acid, INT777The TGR5 specific agonist 6α-ethyl-23(S)-methyl-CA (EMCA or INT-777) is a CA derivative. In animal model, EMCA improved glucose tolerance, stimulated GLP-1 secretion from enteroendocrine L cells, improved insulin sensitivity, and increased the intracellular ATP/ADP ratio in obese mice. TGR5 agonists can reduce intestinal inflammation and prevent liver inflammation (Wu et al., 2019). Activation of TGR5 also reduced macrophage inflammation and lipid load to reduce atherosclerotic lesions (Li et al., 2018).
5.3 Bile acid sequestrantBile acid sequestrant (BAS) is an anion exchange resin originally used to reduce hypercholesterolemia. BAS increased HDL-cholesterol levels by 3%–5% and reduced LDL-cholesterol levels by 15%–30%, while serum triacylglycerol (TAG) levels were unchanged or increased slightly. BAS reduces intestinal FXR activity by trapping BA in the intestinal lumen and increasing BA excretion in the feces. Cholesterol continues to be converted by hepatocytes into bile acids, lowering plasma cholesterol levels (Hao et al., 2017).
BAS stimulates GLP-1 secretion by inhibiting ileal reabsorption of BAs. BAS drives BAs to the colon where L-cell density is highest. L-cell density is greatest in the colon, where BAs are driven by the BAS. BAs bind and activate TGR5 on L-cell, reducing intestinal glucose absorption, and promoting hepatic glycolysis and lipogenesis (Harach et al., 2012). Further study showed that BAS improved blood glucose by reducing glycogenolysis in the liver via TGR5/GLP-1 (Potthoff et al., 2013). The effects of colsevelam hydrochloride on blood glucose homeostasis were observed only in FXR ob/ob WT mice, but not in FXR KO ob/ob mice, suggesting that FXR may be responsible for the effects of Colesevelam hydrochloride (Supplementary Table S1) (Hartmann et al., 2022). It is consistent with these results that BAS treatment improves glucose clearance and insulin sensitivity in T2DM patients. After taking Colesevelam hydrochloride, insulin secretion increased. Long-term treatment of T2DM obese ZSF1 rats with another BAS, SAR442357, increased plasma insulin levels and decreased HbA1c, cholesterol, and triglyceride levels (Supplementary Table S1). Unlike Colesevelam hydrochloride, SAR442357 also slows the progression of diabetic kidney disease (DKD) (Castañeda et al., 2021).
5.4 Tauroursodeoxycholic acidTauroursodeoxycholic acid (TUDCA) can activate FXR in mouse pancreatic β-cells, inhibit the activity of sulphonylurea receptor 1 (SUR1, a subunit of ATP-sensitive potassium channel), reduce K+ efflux, increase cytoplasmic Ca2+ concentration, and promote insulin secretion. And the activation of TGR5 in islet α-cells can induce the expression of glucagon proconvertase-1 (PC1), which catalyzes the production of GLP-1 from glucagon. Then GLP-1 migrates to β-cells and binds to the GLP-1 receptor on its membrane to enhance the insulin secretion function of β-cells (Kumar et al., 2016). Recent studies have found that TUDCA affects blood glucose homeostasis and insulin signaling by activating insulin receptors. TUDCA intervention improves glucose homeostasis in DIO mice, which is eliminated by injection of the insulin receptor antagonist S961. Molecular docking showed that TUDCA exhibited high affinity for TGR5 and insulin receptor and interacted strongly with insulin binding sites one and two of insulin receptor (Supplementary Table S1) (da Silva et al., 2021; Zangerolamo et al., 2021).
5.5 Hyodeoxycholic acidHyodeoxycholic acid (HCA) accounts for 80% of porcine bile. The trace amounts of HCA and its derivatives have been found in human blood (Spinelli et al., 2016). Pigs are unique model animal with a diabetic lifestyle but are resistant to developing T2DM. In vitro HCA upregulates GLP-1 secretion and preproglucagon gene (Gcg) transcription. HCA is found to act as both a TGR5 agonist and an FXR antagonist to promote GLP-1 secretion and Gcg gene transcription in mice, which is a unique mechanism not found in other bile acid producing species. The effects of HCA on serum GLP-1 and insulin levels, glucose tolerance, and insulin tolerance in TGR5+/+ mice were significantly eliminated in TGR5−/− mice, suggesting that HCA upregulates GLP-1 secretion via TGR5 in vivo. In a clinical cohort study, it was confirmed that lower concentrations of serum HCA were associated with diabetes and closely correlated with glycemic markers, suggesting a protective effect of HCA on the development of diabetes in mammals and may be used for T2DM treatment (Zheng et al., 2021).
5.6 Ursodeoxycholic acidAs the drug of choice for the treatment of primary biliary cirrhosis and the dissolution of cholesterol stones, UDCA mainly regulates the physiological function of cholesterol by reducing the intestinal absorption speed of cholesterol and breaking down cholesterol-containing micelles (Bellentani, 2005). In liver disease, UDCA provides clinical benefits by mediating hepatocyte protection, bile secretion and immunomodulation. The hepatocyte-protective effect of UDCA is partly derived from the inhibition of apoptosis (Lukivskaya et al., 2007). UDCA also reduces the permeability of mitochondrial membranes and the release of hydrolases from damaged hepatocytes (Quintero et al., 2014). UDCA was found to improve hepatic steatosis and insulin sensitivity by inducing hepatic lipid excretion and inhibiting hepatic long-chain free fatty acid uptake in obese mice (Nie et al., 2012; Castro et al., 2013; Oh et al., 2016). The effect of UDCA on age-related body fat accumulation and the anti-obesity mechanisms of UDCA in the liver and white adipose tissue was investigated in humans. The results showed that long-term administration of UDCA reduced hepatic lipogenesis and inflammatory responses, which supported the beneficial role of UDCA in the prevention and treatment of T2DM (Al-Salami et al., 2017).
UDCA has anti-inflammatory effects on the ileal mucosa and increases the survival rate of pancreatic β-cells (Mooranian et al., 2016), which suggests its potential application value in T2DM. Three weeks after UDCA intervention was conducted in diabetic Balb/c mice, the blood, tissue, urine, and feces were collected for blood glucose, inflammation, and bile acid analysis. The results showed that UDCA had a regulatory effect on bile acid composition, but did not affect blood glucose levels. The concentrations of blood glucose, HbA1c, HOMA-IR, IFN-γ, IL-6, and IL-10 in T2DM mice remained similar to those in control group, suggesting that UDCA lacked significant hypoglycemic or anti-inflammatory effects in T2DM mice. The levels of CDCA, LCA and UDCA in plasma, brain, and skeletal muscle of T2DM mice were significantly increased after UDCA intervention, suggesting that UDCA regulates bile acid composition and enterohepatic cycling, and may treat T2DM by changing the concentrations of other BAs such as LCA and UDCA (Supplementary Table S1) (Mooranian et al., 2022).
5.7 Lithocholic acidLCA is a second endogenous agonist of the vitamin D receptor (VDR) (Sasaki et al., 2021). LCA can prevent apoptosis of mouse colonic epithelial cells to maintain intestinal barrier function. LCA was found to be more effective than UDCA in preventing the release of TNF-α from colonic epithelial cells in vitro. LCA was also found to be more efficient than UDCA in reducing dextran sodium sulfate-induced inflammation in mice with colitis in animal experiments. In animal experiments, LCA was also more effective than UDCA in preventing dextran sulfate sodium (DSS)—induced inflammation in mice with colitis. The body weight was significantly reduced by LCA treatment, which may be due to the reduced food intake in LCA-treated mice or the effects of BAs on energy expenditure and fat metabolism (Schoeler and Caesar, 2019).
6 Other treatments for Type 2 diabetes mellitus6.1 Vertical sleeve gastrectomyBariatric surgery is one of the most effective and long-lasting treatments for pathologic obesity, T2DM and fatty liver disease (Mingrone et al., 2015). Vertical Sleeve Gastrectomy (VSG) is the most common procedure in bariatric surgery (Angrisani et al., 2015; Buwen et al., 2015). Elevated GLP-1 in circulatory system and changes in systemic BAs level were continuously observed after surgery (Chambers et al., 2014). VSG significantly alters the production, secretion, and redistribution of BAs. A study analyzed the factors that led to the decrease of intestinal BAs levels in obese mice after VSG surgery: on the one hand, the mRNA and protein expression levels of the bile salt export pump were significantly reduced, which reduced the size of the intestinal bile acid pool; on the other hand, VSG-induced increase in intestinal permeability or loss of FXR activity may also lead to decreased BAs levels by promoting paracellular absorption in the proximal intestine. VSG reduces intestinal BAs levels, which leads to impaired intestinal lipid absorption. This mechanism of caloric intake reduction may contribute to the metabolic improvement (Ding et al., 2021a). Another study indicated an increase in endogenous cholic acid-7-sulfate (CA7S) in the gastrointestinal tract of mice and humans after VSG (Supplementary Table S1). As a TGR5 agonist, CA7S regulates blood glucose by increasing TGR5 activation and GLP-1 secretion (Chaudhari et al., 2021).
6.2 Takeda G-protein receptor 5 agonists and farnesoid X receptor inhibitorsIt has been shown that HCA can promote GLP-1 secretion and improve blood glucose homeostasis by activating TGR5 and inhibiting FXR (Zheng et al., 2021), suggesting that the development of TGR5 agonists and FXR antagonists is an effective way to treat T2DM. As a promising drug target, TGR5 can be used to screen new therapeutic agents for T2DM (Velazquez-Villegas et al., 2018), but the application of TGR5 agonists has been limited in recent years due to systemic side effects, such as gallbladder emptying (Stepanov et al., 2013). Recent studies have shown that it is possible to develop a more selective TGR5 agonist. A TGR5 agonist, RDX8940, improved hepatic steatosis and insulin sensitivity without systemic side effects in mice model of MAFLD (Supplementary Table S1) (Finn et al., 2019).
Because that TGR5 agonists absorbed into the circulation would cause significantly off-target effects, intestinal-restricted TGR5 agonists have been proposed as a potential improved therapy for T2DM (Cao et al., 2016). CA7S is an intestinal-restricted TGR5
留言 (0)