The study was approved by the responsible ethics committee (Medical Ethics Committee of the Affiliated Hospital of Qingdao University, No.: QYFYEC 2018–055-01) and was performed at Phase I Clinical Research Center of the Affiliated Hospital of Qingdao University. The study protocol was conducted in accordance with the Declaration of Helsinki, Good Clinical Practice (GCP) and applicable laws and regulations of China National Medical Products Administration (NMPA). Written informed consent was obtained from all subjects before their participation in the study.
Subjects
Sex-related differences have been proved to exist in the extent of CYP3A induction by rifampin [13] and age can also affect the clearance of certain CYP3A substrates [14]. To evaluate the effect of a strong CYP3A inducer on famitinib PK variability without the contribution of gender and age factors, the DDI study was conducted in healthy male adult subjects aged in 18–50 years, with a body mass index (BMI) between 19 and 28 kg/m2 and a minimum of 50 kg weight.
The main exclusion criteria included the following: history or presence of clinically significant systemic diseases or disorders; significant abnormalities in physical examination and essential laboratory tests; hypersensitivity to investigational products; use of any prescription medication or herbal preparations within 1 month, or use of over-the-counter medication or dietary supplements, within previous 2 weeks, especially drugs that induce or inhibit CYA3A enzyme; abuse of alcohol or drugs; smoking more than 5 cigarettes a day or urinalysis cotinine diagnosis being positive; consumption of any beverages or food containing caffeine or products rich in grapefruit, such as coffee, tea and chocolate, etc., within 48 h prior to dosing or during the trial.
The impact of cigarette smoking on famitinib is unclear now. Cigarette smoke exposure induces hepatic CYP enzymes, especially CYP1A1/2. Whereas CYP3A4 is identified as the principle isoform that mediates famitinib bioactivation in the intestine, CYP1A1/2 is found to be the primary enzyme responsible for famitinib bioactivation in the liver, kidney and lung [9]. Thus, the highly expressed CYP1A of smokers may elevate the risk of famitinib-induced hepatotoxicity and subjects enrolled in our study were all non-smokers, due to the high sensitivity of cotinine diagnosis.
Study design
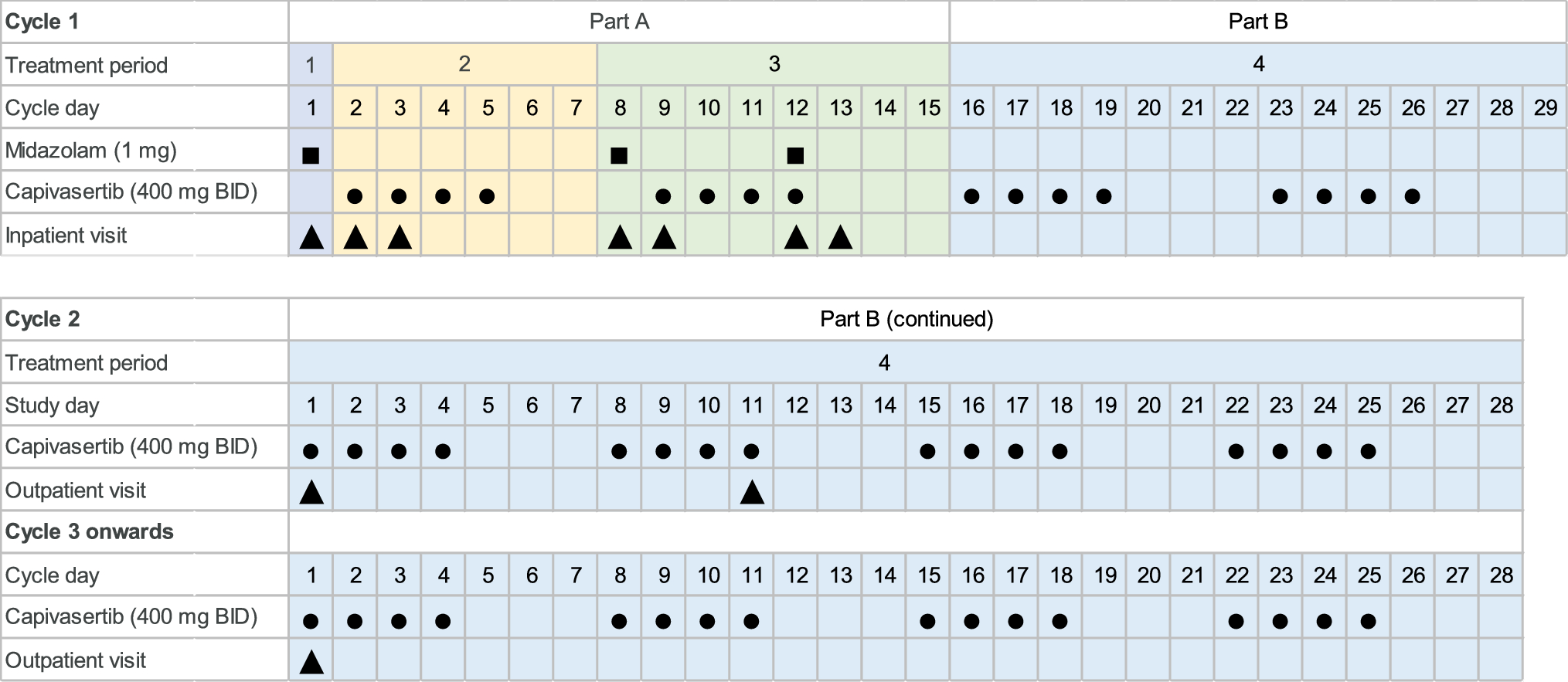
The DDI study was an open-label, self-contrast study comprising the following two periods: period 1 (Days 1–9), administration of a single oral dose of famitinib 25 mg alone in the morning of study day 1; period 2 (Days 10–23), repeated administration of oral rifampin 600 mg once daily for 14 days in the morning of days 10–23, and co-administration of a single dose of famitinib 25 mg on Day 16. The famitinib was supplied as 25 mg capsules (Jiangsu Hengrui Pharmaceuticals Co., Ltd, Jiangsu Province, China; batch no.:200304NU; expiration date: March 2022), while rifampin as 300 mg capsules (Shenyang Hongqi Pharmaceutical Co., Ltd., Liaoning Province, China, batch no.:2001011; expiration date: December 2020). In the two periods, oral doses of famitinib were administered after an overnight fast (at least 10 h) with 240 mL room-temperature water. Subjects were forbidden to drink water within 1 h before and after taking famitinib, and the lunch and dinner were provided at 4 h and 8 h,, respectively, post-drug administration (Day 1, 16). In the second period, subjects received rifampin in the fasting state with 240 mL water and had regular meals 1 h after the dose. Cigarettes, caffeinated drinks and alcoholic products were prohibited during the whole trial period, and when the subjects stayed in the study center (Days 1–4, 10–23), the only food permitted was prepared and provided at predetermined times by the researchers.
Blood sampling and analytical methods
3 mL venous blood samples were collected in lithium-heparin tubes pre-dose and at 1, 2, 3, 4, 5, 6, 8, 12, 24, 48, 72, 96,144 and 192 h after each famitinib dose on the pharmacokinetic profiling days. Samples were centrifuged within 1 h at 1500xg for 10 min at 4℃ to separate the plasma, which was divided into two aliquots (drug monitoring at least 800ul and backup) and stored at – 80 °Cuntil analysis. The whole process was operated in yellow light and avoided being exposed to light because the famitinib metabolite concentrations decreased significantly after light exposure [15], which is similar to sunitinib [16].
Plasma concentrations of famitinib were analysed using a validated liquid chromatography-tandem mass spectrometry (LC–MS/MS) method [9, 15] at Frontage Laboratories Co., Ltd (Shanghai, China). The calibration curve for famitinib covered ranges of 0.050-100 ng/ml. The low limit of qualification (LLOQ) was 0.050 ng/ml. The accuracy, expressed as relative error (RE), was within ± 4.2% and the precision, expressed as coefficient of variation (CV), was < 7.6%, which were conducted on quality control samples with low (0.15 ng/ml), medium (4 ng/ml) and high (75 ng/ml) concentration levels.
Pharmacokinetic calculations
Pharmacokinetic (PK) parameters for famitinib in plasma were estimated by noncompartmental analysis using Phoenix WinNonlin (version 7.0, Pharsight Corporation, St Louis, MO, USA). The primary endpoints were the maximum plasma famitinib concentration (Cmax), the area under the plasma concentration–time curve from time 0 to the last measured time point (AUC0–t), and the area under the plasma concentration–time curve from time 0 to infinity (AUC0–∞). The secondary PK parameters included time to Cmax (Tmax) and the elimination half-life (T1/2), the terminal exponential rate constant (λz), the apparent total body clearance (CL/F). Cmax and Tmax were observed directly from the original concentration–time data. AUC0–t was determined up to the last observed quantifiable concentration using the trapezoidal rule, and AUC0–∞ was the sum of AUC0–t and the extrapolated AUC (AUCextrap), which was calculated based on the last measurable concentration dividing by λz. λz is the slope determined by a linear regression analysis of the terminal phase of the concentration–time profile and T1/2 was obtained as 0.693/λz.
Safety and tolerability
Safety and tolerability were evaluated by monitoring vital signs, physical examination, laboratory tests, electrocardiogram (ECG) and adverse events (AEs). Vital signs, including body temperature, blood pressure (BP) and heart rate, were measured and ECG were performed during baseline period, before drug administration and at 4, 24, 48, 192 h after famitinib administration. Clinical laboratory tests were conducted at screening, day 9, 15, and prior to discharge. AEs, including all subjective symptoms reported by subjects and objective signs observed by clinical investigators, were collected after dosing throughout the study.
Statistical analysis
All subjects who received the study drug and for whom at least one PK parameter data was available were included in the PK analysis sets. The safety analysis sets included subjects who received at least one dose of famitinib or rifampin. Statistical analysis was performed using SAS 9.4 (SAS Inc., Cary, NC, USA). Assuming an intrasubject standard deviation of log-transformed Cmax of 0.3, the tolerance of 80%, and geometric mean ratio (GMR) of 0.2 for AUC of famitinib co-administrated with rifampin versus famitinib only, the 90% confidence intervals (CI) was estimated 0.164–0.244 based on a sample of 18 completing subjects. Considering a drop-off of 15%, 21 subjects were enrolled. The measurement data were expressed as mean ± standard deviation (SD), and categorical variables were described by the percentage. A liner mixed-effects model with log-transformed PK parameters as response was used to calculate the GMR and associated two-sided 90%CI for AUC and Cmax, after eliminating the data with AUC_%Extrap (AUCextrap/AUC) greater than 20%. If the 90%CI was contained within the bounds 0.80–1.25, it was inferred that there was no drug interaction [17].
Safety parameters of the safety analysis sets were summarized using descriptive statistics. AEs were graded according to Common Terminology Criteria for Adverse Events (CTCAE, version 5.0) and coded using Medical Dictionary for Regulatory Activities (MedDRA, version 19.0) System Organ Class (SOC) and Preferred Terms (PT).

留言 (0)