Study design
CPG2-PII and OP-07-001 studies were conducted as phase II multicenter studies that investigated the efficacy, safety, and pharmacokinetics of glucarpidase in patients with delayed MTX clearance after HD-MTX therapy. glucarpidase has demonstrated high efficacy in the United States and Europe in compassionate use. Therefore, those trials were conducted without a comparative group because it is ethically problematic to include patients who are not treated with glucarpidase.
The CPG2-PII study, multicenter, open-label, phase 2 study was conducted to evaluate the potential of glucarpidase to reduce a high blood concentration of MTX in Japanese pediatric and adult patients due to delayed clearance of MTX (jRCT2091220097). Blood samples for measurement of plasma MTX concentration were centrifuged at 4 °C and cryopreserved at − 70 °C or lower. However, it was suggested that the effect of glucarpidase was overestimated because the enzymatic activity of glucarpidase may not be inactivated under these conditions. Therefore, study OP-07-001 (jRCT2080225030) was conducted to confirm the results in CPG2-PII. In OP-07-001, blood collection tubes containing EDTA and citric acid were used to inactivate glucarpidase, which is a zinc-dependent peptidolytic enzyme and functions optimally at a pH near 7.5; thus, the enzyme would be inactivated by chelating zinc and changing the pH to acidic conditions.
These studies were conducted in accordance with the principles of the World Medical Association Declaration of Helsinki, the Good Clinical Practice guidelines, and local regulations. The study protocol was approved by the institutional review board of each institution. Written informed consent was obtained from the patients for participation and enrolment to the clinical trial.
Patients
In the CPG2-PII study, eligible patients were enrolled who had an abnormally high MTX concentration that considerably exceeded the safe concentration range at each time point from 22 to 70 h after starting administration of HD-MTX or those whose MTX concentration exceeded the safe concentration range and whose serum creatinine increased after starting HD-MTX administration. In the case of a patient who had not been treated with glucarpidase, any one of the criteria i) to vii) was met. The criteria were as follows: (i) Blood MTX levels of ≥ 50 µmol/L at least 22 h after the start of MTX administration, (ii) Blood MTX levels of ≥ 5 µmol/L at least 40 h after the start of MTX administration, (iii) Blood MTX levels of ≥ 2 µmol/L at least 46 h after the start of MTX administration, (iv) MTX blood concentration of ≥ 1 µmol/L and signs of acute renal failure at 40 h or later after the start of MTX, (v) MTX blood concentration of ≥ 0.4 µmol/L and signs of acute renal failure at 46 h or later after the start of MTX, (vi) MTX blood concentration of ≥ 0.1 µmol/L (with a dose of MTX 1–3.5 g/m2) at 70 h or later after the start of MTX, (vii) MTX blood concentration of ≥ 0.3 µmol/L (with a dose of MTX > 3.5 g/m2) at 70 h or later after the start of MTX. Additionally, in the patient who had been treated with glucarpidase showed signs of acute renal failure, and MTX blood concentrations of ≥ 50 µmol/L at 22 h or later after the start of MTX. Acute renal failure was defined as (i) the levels of serum creatinine exceeding the upper limits specified in the following table, at no less than 12 h after the start of MTX administration, or a creatinine clearance or glomerular filtration rate (calculated value or actual measurement, for both) of < 70 mL/min or (ii) levels of serum creatinine showing more than twofold increase from before MTX administration or showing more than 1.5-fold increase at the last two sequential blood samplings as well as continuing to increase. In the OP-07-001 study, eligible patients who showed an abnormally high MTX concentration that considerably exceeded the normal concentration range were enrolled at each time point from 22 to 70 h after the onset of HD-MTX administration. Patients who passed at least 15 h after the end of MTX treatment and met any of the following criteria, 1)–4): (1) the blood MTX concentration measured at the site is > 50 µmol/L at 22 h or more after the start of MTX administration. (2) the blood MTX concentration measured at the site is > 5 µmol/L at 40 h or more after MTX administration. (3) the blood MTX concentration measured at the site is > 2 µmol/L at 46 h or more after MTX administration. (4) the blood MTX concentration measured at the site is > 1 µmol/L at 40 h or more after the start of MTX treatment, a sign of AKI was observed. A sign of AKI was defined as meeting any of the following criteria, (i), (ii), and (iii). (i) Serum creatinine level after the MTX administration was higher than upper limit of the site reference value. (ii) At least 1.5-fold increase in the serum creatinine level from baseline after MTX administration. (iii) Increase in the serum creatinine levels by 0.3 mg/dL or higher within 48 h. The inclusion criteria in each study are provided in Supplementary Table S1.
Patients were excluded if they needed any concomitant treatment with drugs that affect MTX clearance/metabolism (e.g., penicillins, cephalosporins, aminoglycosides, tetracycline, nonsteroidal anti-inflammatory drugs, loop diuretics, thiazides, and probenecid) after high-dose MTX therapy and any episode of hypersensitivity reaction for glucarpidase or its additives (lactose, Tris-HCl buffer solution). No patients who were receiving prohibited concomitant medicines at the enrolment.
Treatments
The safety of administering two doses of 50 U/kg per dose at an interval of 48 h was confirmed in the CPG2-PI study. The dose of glucarpidase that had been used for compassionate use in Europe and the United States had been 50 U/kg in all studies. The pharmacokinetics (PK) and drug interaction with LV studies performed in the United States [27] were also conducted at a dose of 50 U/kg. Taking these data into consideration, 50 U/kg was used subsequently in this trial. The dose of glucarpidase was calculated by rounding off the patient body weight to the nearest integer and multiplying this by 50. The glucarpidase 1000 U/vial was reconstituted with 1 mL of sterile saline for injection to adjust the dose. Patients with a MTX concentration ≥ 1 µmol/L, according to local laboratory results at 48 h after the first dose, could receive a second dose of glucarpidase dose at the same concentration as the initial dose in the CPG2-PII study. The same dose was used in the OP-07-001 study but glucarpidase was only administered once.
Outcomes and assessments
In the CPG2-PII study, the primary endpoint was to evaluate the proportion of patients who achieved clinically important reduction (CIR), defined as < 1 µmol/L of the MTX plasma levels after the initial injection lasting for at least 5 days. The occurrence of adverse events or adverse drug reactions and the pharmacokinetic parameters of glucarpidase, MTX, DAMPA LV, and 5-MeTHF were evaluated as secondary endpoints. Renal impairment, pyrexia, neutropenic fever, mucositis, and infections and parasitosis, whose causality was related to MTX, were specified as MTX-related adverse events and their occurrence or nonoccurrence rate were evaluated. The observation period was defined as the interval between the start of observation and administration of glucarpidase, and the observation will end when the protocol treatment ended, and one of the following conditions (whichever comes first) was met: (i) It was assessed that the next course of administration of an antitumor drug can be started for the treatment of the primary disease. (ii) There were no adverse event of grade 2 (CTCAE) (excluding hair loss and abnormal test values). (iii) Adverse events of grade 3 that existed during the treatment period had all resolved to grade 2, and this state did not change for 3 days or longer. (iv) The patient died.
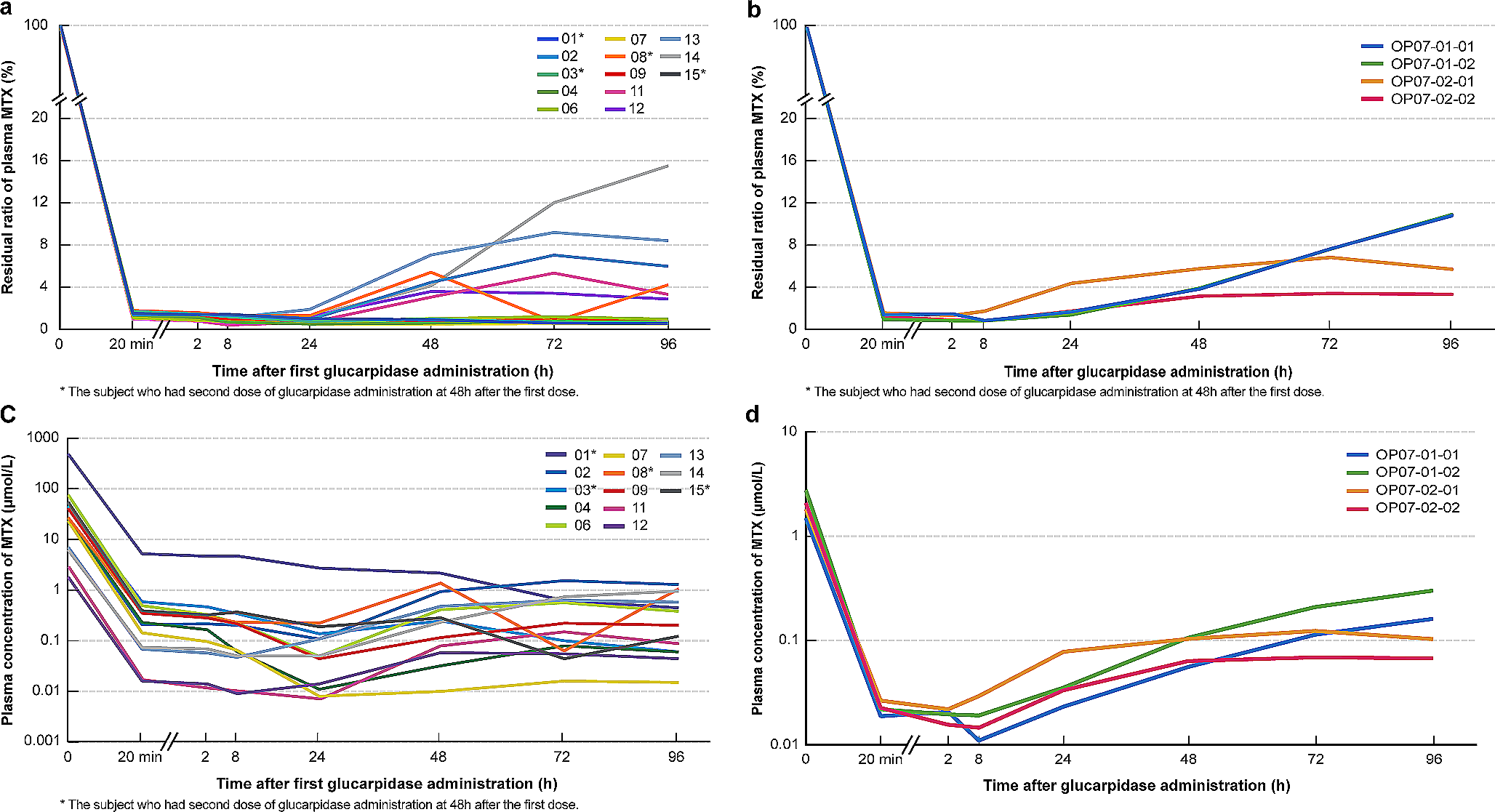
In OP-07-001, the decreasing rate of the plasma MTX concentration (central measurement) at 20 min after glucarpidase administration from the baseline measured immediately before administration was regarded as the primary endpoint. Secondary endpoints included the plasma MTX concentration and achievement of CIR, the occurrence of adverse events, adverse drug reactions, and pharmacokinetic parameters of glucarpidase. The CIR in OP-07-001 study was defined at all the scheduled blood sampling timepoints after the glucarpidase administration whether the plasma MTX concentration via the central measurement was below the threshold (1 µmol/L). The observation period was defined as the interval from enrolment day to 28 days after administration day of glucarpidase unless the patient met either (1) to (6) of the following criteria, (1) When it was judged that treatment for the target disease should be prioritized (chemotherapy was required regardless of the route of administration) when HD-MTX therapy was performed, (2) When the investigator or subinvestigator judges that the study should be discontinued because of occurrence of adverse events, (3) When the subject or his/her legally authorized representative requested to discontinue the study, (4) When the subject was found to be ineligible for the study, (5) When it was found impossible to perform the necessary observations/examinations because of the subject’s convenience or (6) When the investigator or subinvestigator judged that the study should be discontinued.
Sample size
In the CPG2-PII study, considering that the number of patients with the target disease is rare, 18 patients were set to study the effectiveness and safety of the glucarpidase and the pharmacokinetic analysis of each analyte in a single dose, open-label design.
In the OP-07-001 study, in reference to the results of Study CPG2-PII, when the expected mean decreasing rate of the plasma MTX concentration (central measurement) was set to 99% and the standard deviation to 0.25, at least 3 patients were required to confirm that the mean decreasing rate exceeds 98.5% by one side t-test with a significance level set to 10% and power of 80%.
Measurements
In the CPG2-PII study, blood samples for glucarpidase, MTX, and DAMPA analysis were collected on day 1 (before glucarpidase dosing, 20 min and 2 h after glucarpidase dosing, and before a second LV administration) and were collected on day 2 to 5 continuously. Blood samples for LV and 5-MeTHF analysis were collected on days 1 (2 and 3 h after glucarpidase dosing and before a second LV administration) and 2 (14–20 h after glucarpidase dosing, 1 h after LV dosing, and before next LV administration). glucarpidase levels were measured via immunoassay at a central testing laboratory. The concentrations of MTX, DAMPA, 5-MeTHF, and LV in plasma were measured using LC/MS/MS at the central laboratory while the MTX concentration was measured at a local laboratory, with an MTX assay kit. The sampling times are listed in Supplementary Table S2. Antibody tests for glucarpidase were performed on day 1 (before glucarpidase dosing) and 1, 3, and 6 months after glucarpidase dosing. Measurement of vital signs and body weight, and laboratory tests were performed.
In the OP-07-001 study, blood samples for glucarpidase analysis were collected on day 1 and 2 (before glucarpidase dosing and 20 min and 2, 24, and 48 h after glucarpidase dosing). Blood samples for MTX and DAMPA analysis were collected on day 1 to 5 (before glucarpidase dosing and 20 min and 2, 8, 24, 48, 72, and 96 h after glucarpidase dosing). glucarpidase was measured by immunoassay at the central laboratory, and MTX was measured by MTX assay kit at the local laboratory. MTX and DAMPA were measured via LC/MS/MS at the central laboratory. Vital signs and body weight were measured, and laboratory tests and 12-lead electrocardiogram were performed.
Statistical analysis
In the CPG2-PII study, the primary endpoint was achievement of CIR that was the highest MTX concentration after administration of glucarpidase was below 1 µmol/L. A proportion of patients who achieved CIR was calculated as the primary analysis. A two-sided 95% confidence interval (CI) for the proportion of CIR was calculated using the exact method based on a binomial distribution. As secondary analysis, the number and proportion of patients with MTX-related adverse events, pharmacokinetic parameters of glucarpidase, MTX, DAMPA, LV, and 5-MeTHF, and incidence of the adverse events and adverse reactions were calculated.
In the OP-07-001 study, for the primary analysis, the decreasing rate of the plasma MTX concentration at 20 min after the start of glucarpidase administration from baseline and mean of the decreasing rate with one-sided 90% CI [lower limit] were calculated in the full analysis set. The datasets analyzed in this study are available from Ohara Pharmaceutical Co., Ltd.

留言 (0)