From 2019, SARS-CoV-2 was recognized as the etiological agent of COVID-19 [14], making necessary rapid detection of infected patients.
PCR- RT is the gold standard for diagnosing SARS-CoV-2 infection. However, especially in the ED, it is important the use of rapid screening methods to limit viral transmission and prevent COVID-19 spreading in hospital settings [15].
RADTs represent an efficient alternative as a first-line diagnostic method combining both advantages: low price and quick results. As the detected antigens are expressed during viral active replication, RADT accuracy is closely linked to the viral load and it can be used to identify acute infection [16].
The guidance released on 11th September by the World Health Organization (WHO) [17] recommended use of RADTs for diagnosis of COVID-19 when the RT-PCR test is not available underlying that it must have a sensitivity of at least 80%.
Many studies are available in literature about the use of RADTs in the pediatric ED, mainly focused on comparison with the gold standard RT-PCR.
Carbonell- Sahuquillo et al. [3] evaluated the Panbio™ COVID-19 Ag Rapid Test Device as a point-of-care diagnostic tool for COVID-19 at a pediatric ED. The authors underline that, even if the assay did not meet one of the criteria (at least 80% sensitivity) recommended by WHO interim guidance for RADT diagnosis of SARS-CoV-2 infection, its performance in identifying children with high SARS-CoV-2 RiboNucleic Acid loads in the upper respiratory tract, which associate with contagiousness, makes it a valuable tool for the management of children with suspected COVID-19 at the ED.
Ollier et al. [6] found that sensitivity of RADTs increased from 69.6 to 82.9% when performed on symptomatic children suggesting that RADTs sensitivity depends on the entity of nasal viral load at testing time, which is higher in the first few days of infection when patients are most likely to be symptomatic. Their results are in line with what has been observed by Mockel et al. [13]: false negatives obtained with RADTs coincide with low viral load confirmed by RT-PCR.
The Panbio™ rapid antigen test kit for SARS-CoV-2 (Abbott Diagnostic GmbH, Jena, Germany) is a qualitative test using specimens from nasopharyngeal swabs. The manufacturer declared in patients with symptoms a sensitivity of 93.3% overall and 98.2% in those RT-PCR cycle threshold ≤33, and a specificity of 99.4% [18]. These data agree with the findings in our cohort of hospitalized, and therefore symptomatic patients: the Panbio™ rapid antigen test showed a sensitivity of 94% and a specificity of 100%.
Assuming that RADTs reach high sensitivity mainly when patient is contagious, and that in EDs screening for SARS-CoV-2 is aimed precisely at avoiding the viral transmission during visits and procedures that the patient must carry out quickly making it difficult to obtain the result of a test analyzed by RT-PCR, our study wants to provide a description of the epidemiological picture during the “fourth wave” of the Pandemic evaluating the performance of the Panbio™ COVID-19 RADT for detecting SARS-CoV-2 and describe the cohort’s clinical features, considering positive cases observed in the aforementioned period. Moreover, our efforts aim at evaluating the impact of the introduction in Italy of COVID-19 vaccination for children and teens seen at ED during the study period. Regarding the demographic characteristics, we observed an overlapping median age between positive and negative ones. As regards clinical features, the number of patients admitted to the ED for fever and for headache was statistically higher in those who tested positive than negative counterpart (p < 0.05). On the other hand, the number of patients who came to ED for cough was statistically higher in negative patients than in the positive ones. This unexpected finding can be explained by public health measures to tackle Coronavirus spread, such as the obligation of face masks, which did not involve children. We can speculate that this may be attributable to contemporary circulation of other respiratory viruses.
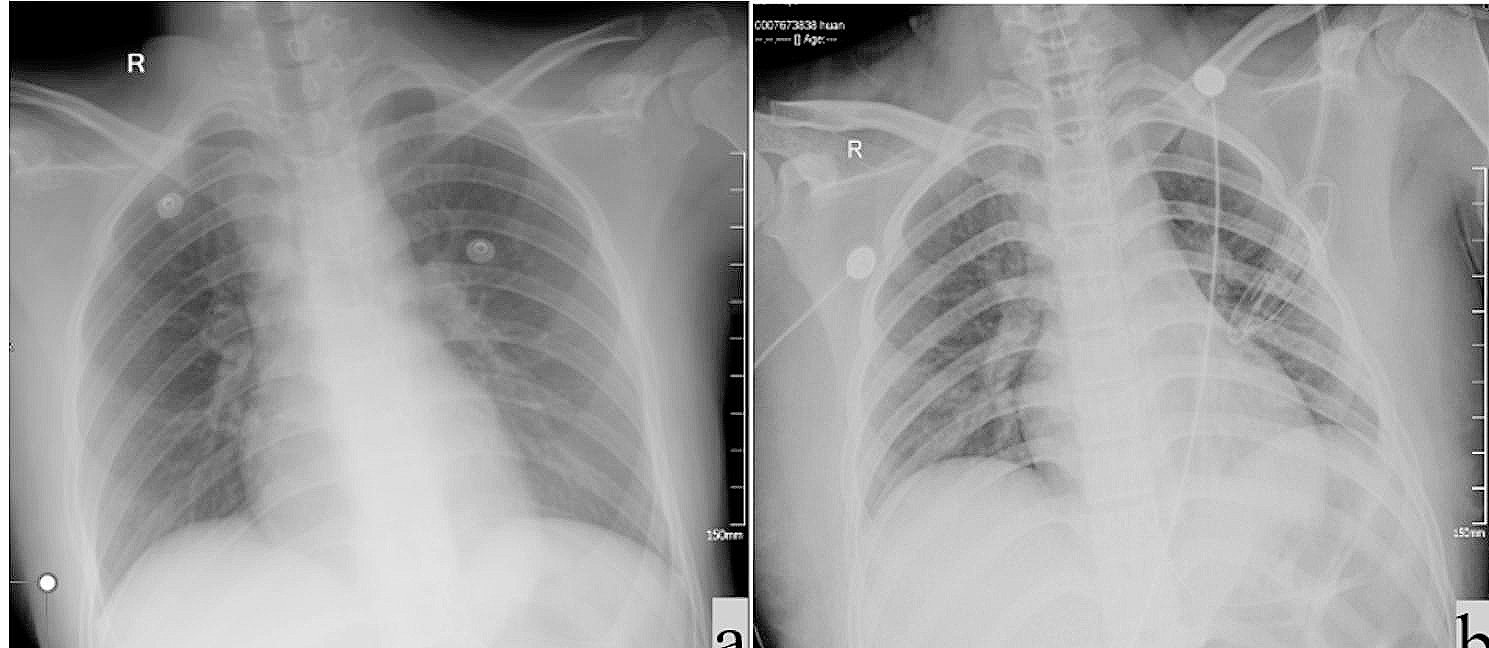
No significant difference was found regarding hospitalization rates between positive and negative groups, but we can trace back this data to the scarcity of pneumonia related to COVID-19 in pediatric patients, since the disease in children runs mildly in the majority of cases. According to triage severity, we did not find a statistically significant difference in patients admitted between positive and negative. On the other hand, the number of positive patients conducted to the ED by ambulance was significantly greater compared to the negative group; in about 70% of cases the reason for accessing ED was fever. This aspect may reflect parents’ fear of having contracted the virus and of having to manage this condition at home in a time when accessing to territorial pediatric care was more difficult and subject to the execution of a COVID swab. Moreover, our subcohorts (A, B, C) according to the different timing to vaccination allowed us to note that the distribution of positivity is not statistically significant in the three groups (p > 0.05).
It is interesting to note that, in the period before vaccine implementation among children, the number of accesses to the ED was significantly higher for groups A and C than in the subsequent period, probably due to the pandemic curve with a peak of the “fourth wave” in January 2022. However, group B did not show this trend. Furthermore, epidemiological context must be considered: by the start of the study period, the 7-day Italian incidence rate was 54 per 100,000 on September 6–12, 2021 and the peak of the fourth wave was reached in the week 10–16 January 2022 with an incidence rate of 2021 per 100,000. At the end of the observational period a 7-day incidence rate of 433 per 100,000 was recorded in Italy [8].
According to our knowledge, this is the first study describing the clinical characteristics of a pediatric cohort afferent to the ED who tested positive for a rapid antigen test also referring to the progress of the vaccination campaign in children and the national trend of the pandemic.
It is not possible to express an absolute opinion about the vaccination campaign’s impact because the effects are to be sought after the observation period of this study.
Our study has some limitations: first, no data about time of onset of symptoms have been collected and all patients were subjected to RADT indifferently; furthermore, the most important limitations of this study are its retrospective design and the lack of RT-PCR data for all patients because this test, as per our protocol, is performed only in children requiring hospitalization. However, we have tried to limit the effects of these by opting to adopt a descriptive rather than an analytical approach, and by making within-group comparisons.





留言 (0)