SMILE is a comparatively new method that has only been applied in clinical practice since 2011 [10]. Still, it is recognized for its superiority in achieving better corneal biomechanical stability [3]. In this study, SMILE and FS-LASIK revealed no statistical differences in terms of their efficacy, safety, predictability, or stability for myopic corrections of − 1.00 to − 6.00 D, in agreement with previous studies [7, 11]. Our results also revealed that SMILE and FS-LASIK had the same probability of myopic regression and ascertained predictors affecting myopic regression. To the best of our knowledge, this study is the first to investigate myopic regression in a large number of patients with myopia from − 1.00 to − 6.00 D and the first to discuss the relevant predictors of myopic regression for the SMILE and the FS-LASIK procedures.
Variation in myopic regression
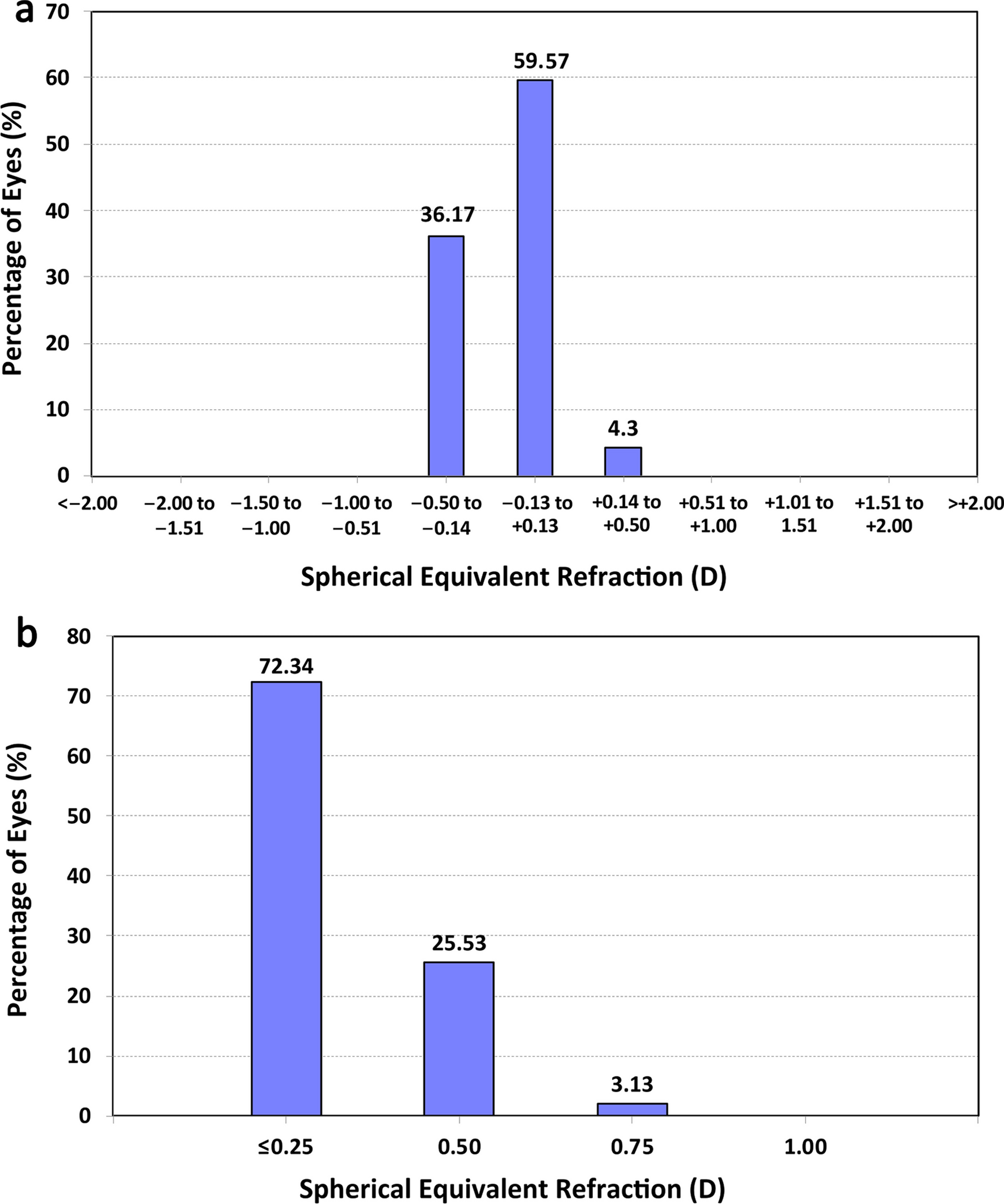
The mean postoperative SEQ was − 0.15 D in the SMILE group and − 0.10 D in the FS-LASIK group at 12 months. This finding was similar to previously published results that indicated a tendency toward a more myopic residual SEQ, at − 0.01 to − 0.33 D in SMILE versus − 0.02 to − 0.17 D in FS-LASIK [12]. Overall, 77.02% of the eyes in the SMILE group and 77.36% in the FS-LASIK had a postoperative SEQ within ± 0.50 D, which is the approximate value published in a previous study [13]. In total, 95% of the eyes in the SMILE group and 96% in the FS-LASIK group were within ± 1.00 D of the targeted SEQ, agreeing with previous reports [13, 14].
We also provide the first evaluation and comparison of the rates of myopic regression for a SMILE and an FS-LASIK group. The incidence of myopic regression was lower in our FS-LASIK group than in a previous study by Lin et al. [9], who showed that 43.6% of eyes that underwent FS-LASIK had myopic regression. The higher myopic regression rate might be attributed to eyes with more severe myopia within − 10.00 D in their study compared with ours (within − 6.00 D). Their preoperation average SEQ (− 6.17 ± 1.86 D) was more elevated than ours (− 4.51 ± 1.29 D). Myopic regression would vary according to myopic diopter if the definition and inclusion criteria were uniform. We paid attention to the myopic diopter, the definition and inclusion criteria, method of surgery, and follow-up time when we compared the percentage of myopic regression [9]. The impact was more evident within − 0.50 D and became insignificant when the definition of myopic regression increased to − 1.00 D, as in the study by Lin et al. [9].
According to our univariate analysis, the myopic regression rate was higher with FS-LASIK than with SMILE. The cumulative risk for myopic regression was 16.3% for FS-LASIK and 11.9% for SMILE at 12 months (P = 0.010). This result was supported by the findings of Reinstein et al. [15], who reported that the intact anterior lamella remained stronger after SMILE than after LASIK, according to the mathematical model of Randleman et al. [16, 17].
We also rectified the differences between the two groups with the Cox PH model for some variables, including the mean age of 27.49 ± 6.78 years in FS-LASIK and 28.38 ± 6.91 years in SMILE (P = 0.000) and the pre-HOA-RMS3 of 0.26 ± 0.12 μm in FS-LASIK and 0.25 ± 0.13 μm in SMILE (P = 0.005). No significant difference was evident for myopic regression after all covariates were adjusted. This result could be supported by the findings of Agca et al. [13], who reported that corneal hysteresis (CH) and a corneal resistance factor (CRF) did not differ significantly between SMILE and FS-LASIK postoperatively. The similarity of the biomechanical effects after SMILE and FS-LASIK might sustain this parallel occurrence of myopic regression. Kanellopoulos [18] showed that the SMILE procedure reduces the tensile strength in lower myopic corrections while retaining a similar tensile strength in higher myopic correction compared with LASIK. Magallanes et al. [19] proved that the significant loss of corneal strength following large myopic corrections might lead to refractive regression.
Predictors for myopic regression
Factors that predicted myopic regression varied in previous studies. The mechanism of myopic regression might include corneal remodeling [5] and biomechanical changes [20] in the anterior and posterior corneal surfaces [21, 22], axial length elongation, and nuclear sclerosis by age during the long-term follow-up period [23]. The identified predictors that affected myopic regression after LASIK included a higher degree of astigmatism [24], the subjective SEQ [20], age [25], IOP [26, 27], and OZ diameter [28]. The significant factors that affected myopic regression in the present study included pre-HOA-RMS3, pre-subjective sphere, ACD, corneal diameter, OZ, and predicted DA.
The pre-HOA-RMS3 (HR = 3.79, P = 0.004) was a risk factor for myopic regression. In this study, pre-HOA-RMS3 was a 3 mm pupil diameter root mean square of high-order aberration. Previous studies found that higher HOA-RMS facilitates myopia progression [29]. High-order aberrations induced by imperfections in the cornea and lens might be inherited from the patients’ parents, and genetic contributions to myopia have been recognized in previous studies [30]. Higher HOA-RMS3, which degrades the retinal image, may accelerate the eye's axial elongation, and increase myopia [31]. Another reason may be that HOA-RMS3 increases with accommodation [32], and the refractions in the postoperative period were recorded using an automatic refractometer with accommodation. An accommodated status would be inclined to having more severe myopia. Further prospective studies are needed on the effects of HOA-RMS3 on myopic regression.
ACD (HR = 0.54, P = 0.015) was a protective factor against myopic regression. One reason might be that ACD with non-accommodation was deeper than the accommodation process [33]. The ACD became 1.5% shallower per diopter of accommodative demand, with a median of about 0.99% at − 1 D, 2.63% at − 2 D, and 4.47% at − 3 D for ACD with accommodation. Chen et al. reported that eyes with cycloplegics, non-accommodation, would increase ACD depth and decrease SEQ in low to moderate myopic eyes [34]. Therefore, the eye with accommodation tended toward greater myopia [35]. The other eyes with similar axis length would have deeper ACD and lower SEQ, according to Nakao et al. [36], and less myopic regression.
In our study, the corneal diameter (HR = 1.51, P = 0.016) was a risk factor for myopic regression. The corneal diameter might reflect the eyeball’s size [36], and the eyeball extension from back to front was hypothesized to be a more significant factor than equatorial ocular expansion in axial myopia, based on the mechanical tension theory [37, 38]. A more prominent cornea diameter resulted in a higher myopia SEQ. In our study, the higher pre-sphere led to more significant myopic regression.
As in previous studies, a higher pre-subjective sphere (HR = 0.78, P = 0.016) increased myopic regression [28, 39]. A larger OZ (HR = 0.49, P = 0.020) was a protective factor against myopic regression but only had a minor effect, in agreement with previous reports [28, 39]. The predicted DA (HR = 0.99, P = 0.003) correlated with the spherical equivalent, OZ, and ablation method (aspherical and spherical). A deeper DA decreased the myopic regression, consistent with previous study findings that aspherical ablation could conserve the DA in cases of higher myopia or a thinner cornea, and yet it might increase myopic regression more than spherical ablation [39].
Multivariate analysis with the Cox PH model, conducted to ascertain the impact factors for myopic regression, revealed the HR of myopic regression in 12 months. Using the Cox PH model, the HR of each covariate was obtained to determine the impact of each factor on the risk of myopic regression. Thus, when patients asked for a preoperative consultation, the clinicians could inform them of the possibility of myopic regression according to each patient’s situation.
Our study is not without limitations. It was more convenient to obtain postoperative refraction by autorefraction rather than subjective and cycloplegic refraction at each follow-up visit. However, considering the age of our study participants (adults), the accommodation should not have markedly affected the results. In support of this, Pesudovs [40] showed excellent agreement using subjective refraction, and this was shown to be unaffected by refractive surgery. A second limitation of this retrospective study and selecting the right eyes was the probability of selection bias that could not be excluded. Therefore, some covariates are confounding variables for estimating the myopic regression between the FS-LASIK and SMILE groups. We adjusted all the covariate differences by multivariate analyses with a Cox PH model to minimize their influence on myopic regression. We have also chosen the right eyes as previous studies show high interocular symmetry in bilateral eyes such as refraction [41], corneal biometrics [42, 43], ACD, and IOP [44]. In the future, we plan to devise a prospective and randomizing study to investigate predictors of myopic regression after laser refractive surgery.


留言 (0)