
記住我
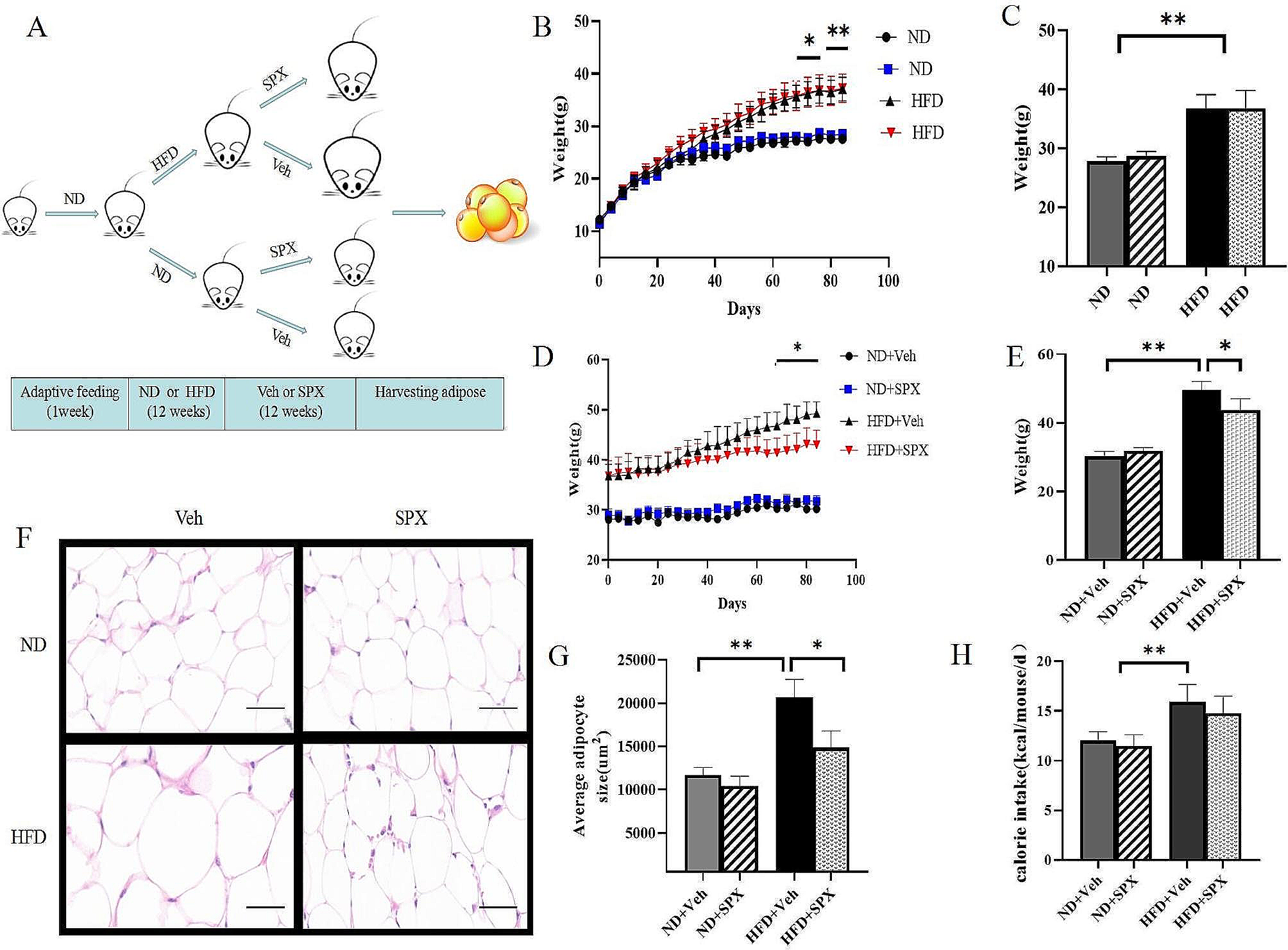
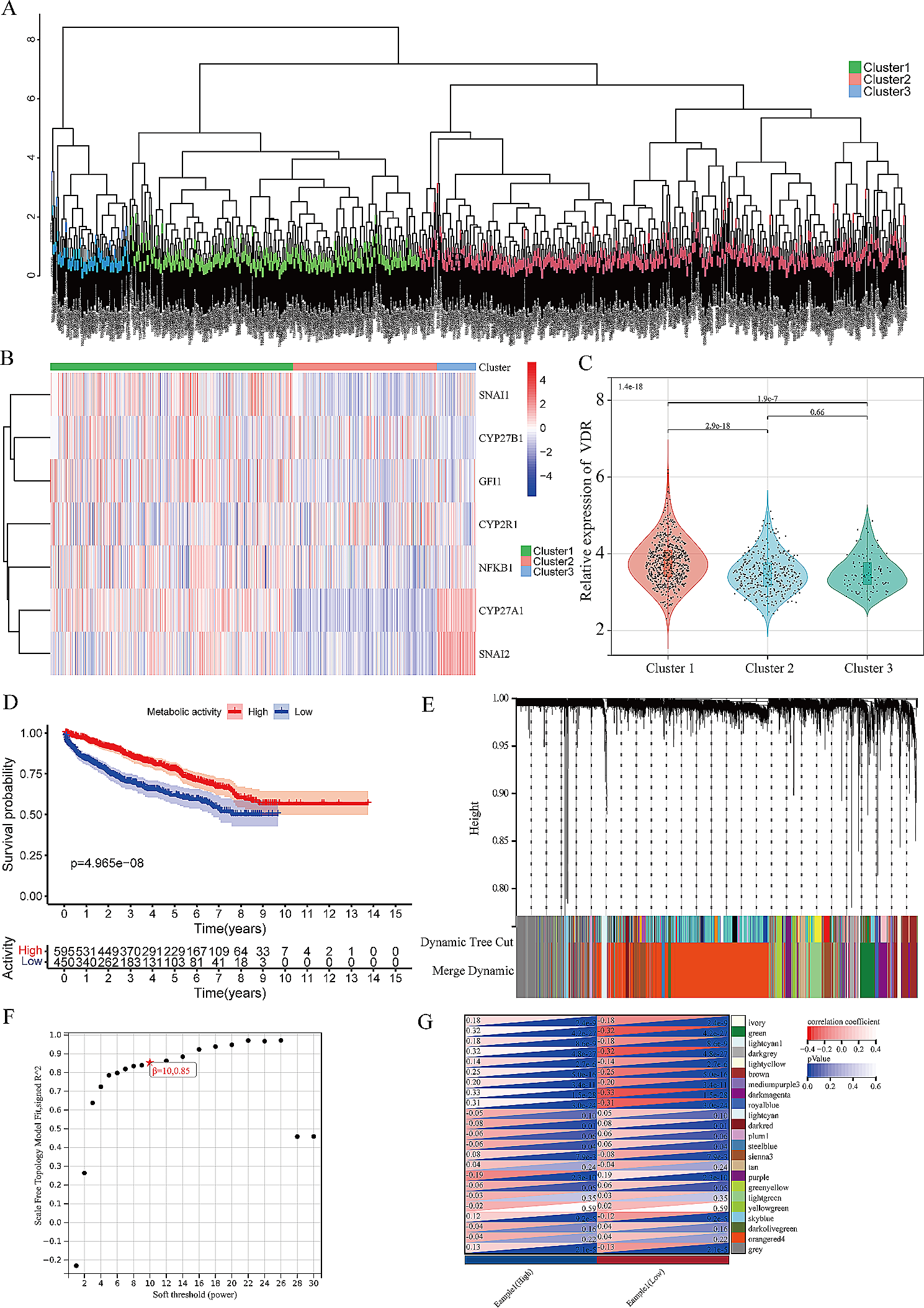


We used data from the Ansan–Ansung Cohort of the Korean Genome and Epidemiology Study (KoGES), which is an ongoing prospective community-based cohort study investigating the environmental and genetic factors affecting prevalent chronic diseases. The study design is described in detail elsewhere [21]. In brief, the Ansan–Ansung cohort study recruited 10,030 individuals aged 40–69 years in a rural (Ansung) and an urban (Ansan) area from 2001 to 2002. Participants were followed up biennially, and we used the follow-up data until 2016 for this study. The final analytical sample of the present study consisted of 9294 participants (4458 men and 4836 women) after excluding those without HbA1c data (n = 3), those with missing covariates (n = 224), those having a history of CVD or cancer (n = 367) at baseline, and those without linked mortality data (n = 142) (Fig. 1). All participants provided written informed consent, and the study protocol was approved by the Institutional Review Board of National Institute of Health, Korea.
Fig. 1
Flow chart of the cohort study
MeasurementsDuring each examination, information on socio-demographic and lifestyle characteristics, personal medical histories and medication usage were collected by trained interviewers using structured questionnaires.
Anthropometric measurements were obtained by trained research staff using standardized protocols and all measuring instruments were calibrated everyday before examination. Standing height was measured using a stadiometer (SECA 225; SECA, Germany) and body weight was measured using a digital scale (GL-60000-20; CAS Korea, Korea). Waist circumference was measured at the midpoint between the lower rib margin and the top of the iliac crest in the standing position. Blood pressure was measured by nurses in both arms in a sitting position with the arms supported at heart level after 5 min of rest using mercury sphygmomanometers (Baumanometer-Standby; W.A. Baum Co. Inc., USA). We used means of measurements from both arms for systolic blood pressure (SBP) and diastolic blood pressure (DBP).
Blood samples of all participants were collected from the antecubital vein after at least 8 h of fasting. HbA1c levels were measured using high performance liquid chromatography (Bio-Rad Variant II; Bio-Rad Laboratories, Inc., Japan) according to the National Glycohemoglobin Standardization Program. The total cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, fasting blood glucose, total bilirubin, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) levels were measured using enzymatic methods (HITACHI Automatic Analyzer 7600; Hitachi, Japan and ADVIA 1650 Auto Analyzer; Siemens, USA). The red blood cell (RBC), hemoglobin, and hematocrit levels were measured using optical methods by laser beam (ADVIA 120 Hematology System; BAYER, USA).
Known diabetes was defined as having a history of physician-diagnosed diabetes or under treatment with oral antidiabetic agents or insulin at each wave of examination. Hypertension was defined as SBP ≥ 140 mmHg or DBP ≥ 90 mmHg, having a history of physician-diagnosed hypertension, or under treatment for hypertension. Dyslipidemia was defined as total cholesterol ≥ 230 mg/dL, HDL cholesterol < 40 mg/dL, or triglycerides ≥ 200 mg/dL, having a history of physician-diagnosed dyslipidemia, or under treatment for dyslipidemia. Liver disease was defined as having a history of physician-diagnosed hepatitis or liver cirrhosis. Anaemia was defined as haemoglobin < 13 g/dL for men and haemoglobin < 12 g/dL for women.
Mortality outcomesThe cohort data were linked to death records (until 31 December 2017) provided by Statistics Korea using resident registration numbers, a unique identifier assigned to all citizens in the Republic of Korea. All death certificates in Koreans are registered to the government, and cause-of-death are ascertained by medical certificates supplemented by linkage to 21 administrative datasets (e.g. National Health Insurance data, National Cancer Registry, and Police Report) to enhance acccuracy of identifying the underlying causes by Statistic Korea (Statistics Korea, Annual report on the causes of death statistics, 2021). The present study investigated the all-cause mortality and cause-specific mortality from CVD (I00 to I99) and cancer (C00 to C97) as classified by the Korean Classification of Diseases, 6th Revision (the Korean version of the International Classification of Diseases, 10th Revision). We also examined mortality from all external causes (S00 toT98) as a negative control.
Statistical analysesParticipants were divided into a known diabetes group and five groups categorized by HbA1c levels (< 5.0%, 5.0–5.4%, 5.5–5.9%, 6.0–6.4%, and ≥ 6.5%) as previously described [9, 12, 22]. The baseline characteristics of participants across HbA1c groups are presented as means and standard deviations for normally distributed continuous variables and as medians and interquartile ranges for skewed continuous variables. Categorical variables are presented as numbers with percentages. Linear trends across HbA1c groups were tested using linear regression for continuous variables and the Cochran–Armitage test or the Mantel–Haenszel test for categorical variables. The Cox proportional hazards model was used to calculate hazard ratios (HRs) for all-cause and cause-specific mortality according to HbA1c category. The proportional hazards assumption was assessed by using log–log survival plots, and no violations were detected. The 5.5–5.9% HbA1c category was set as the reference group. Covariates consisted of factors affecting HbA1c levels and factors reported in the literature to be related to both HbA1c levels and mortality: age (years), sex, residential area (Ansung or Ansan), BMI (kg/m2), smoking (current, past, or never), alcohol use (current, past, or never), regular exercise (yes or no), education (above or below university), hypertension (yes or no), and dyslipidaemia (yes or no).
Models were constructed in the following two ways: (1) a standard Cox proportional hazards model using the baseline HbA1c levels and covariates and (2) a time-dependent Cox propotional hazards model considering HbA1c levels, age, BMI, smoking, alcohol use, regular exercise, hypertension, and dyslipidemia that change over time as time-dependent variables using information from follow-up examination. Missing data were replaced with the values measured in the previous examination. When estimating the risk of cause-specific mortality from CVD, cancer, and external causes, mortality from the other causes was considered competing risk using the Fine–Grey model. Person-years for each participant were calculated as the duration from the baseline examination date to the date of death or 31 December 2017 depending on which came first. Mortality rates per 1000 person-years were calculated for each HbA1c category.
To assess whether the association between HbA1c levels and the risk of mortality differed according to the characteristics of study participants, subgroup analyses were performed for age, sex, smoking status, hypertension, liver diseases, and RBC count. We also tested the interaction effect between HbA1c levels and the characteristics of study participants on mortality using interaction terms.
For sensitivity analysis, we additionally adjusted for RBC count, haemoglobin level, anaemia, and liver diseases which are known to affect HbA1c in our analytical models. We also adjusted for waist circumference instead of BMI. Furthermore, to rule out the effects of possible subclinical disease or underlying poor health condition, we excluded 77 people who died within the first 2 years of follow-up.
After excluding participants with known diabetes, restricted cubic spline regression analyses were performed to model the shape of the association between continuous HbA1c levels at baseline and mortality. Knots were set at the 5th, 25th, 75th, and 95th percentiles and reference was set at the median HbA1c level of 5.6%. The plot was truncated at the 1st and 99th percentiles.
Additionally, we compared the receiver-operating characteristic (ROC) curves and the area under the curve (AUC) for mortality of a conventional model and the model plus baseline HbA1c. The conventional model included age, sex, residential area, BMI, smoking, alcohol use, regular exercise, education, hypertension, and dyslipidemia.
SAS version 9.4 (SAS Institute, Cary, NC, USA) was used for all statistical analyses, and statistical significance was defined as two-tailed p values < 0.05.
留言 (0)