
記住我









Drawing upon interviews with clinicians and administrators (n = 9) and ethnographic observation of planning meetings (n = 3) we describe the development of a Primary Care-Based Buprenorphine Clinic, which allowed patients to access buprenorphine for OUD outside of a specialty substance use disorder or mental health setting, and an E-Consult Service, which provides virtual consultation regarding OUD diagnosis and treatment to clinicians throughout the health care system, including in remote and rural locations. First, we detail how policy change at the national and local level altered clinicians’ perceptions of the need for expanded access to MOUD. We then describe how a model of care delivery was identified and staffing and resources secured. Finally, we describe how a self-appointed team increased staff investment in the change process by networking across clinical silos and bringing staff into the planning process. Figure 1 provides a visual display of the pathways linking national policy to local change processes. Table 1 maps the local actions and processes described in the text to CFIR constructs and ERIC implementation strategies.
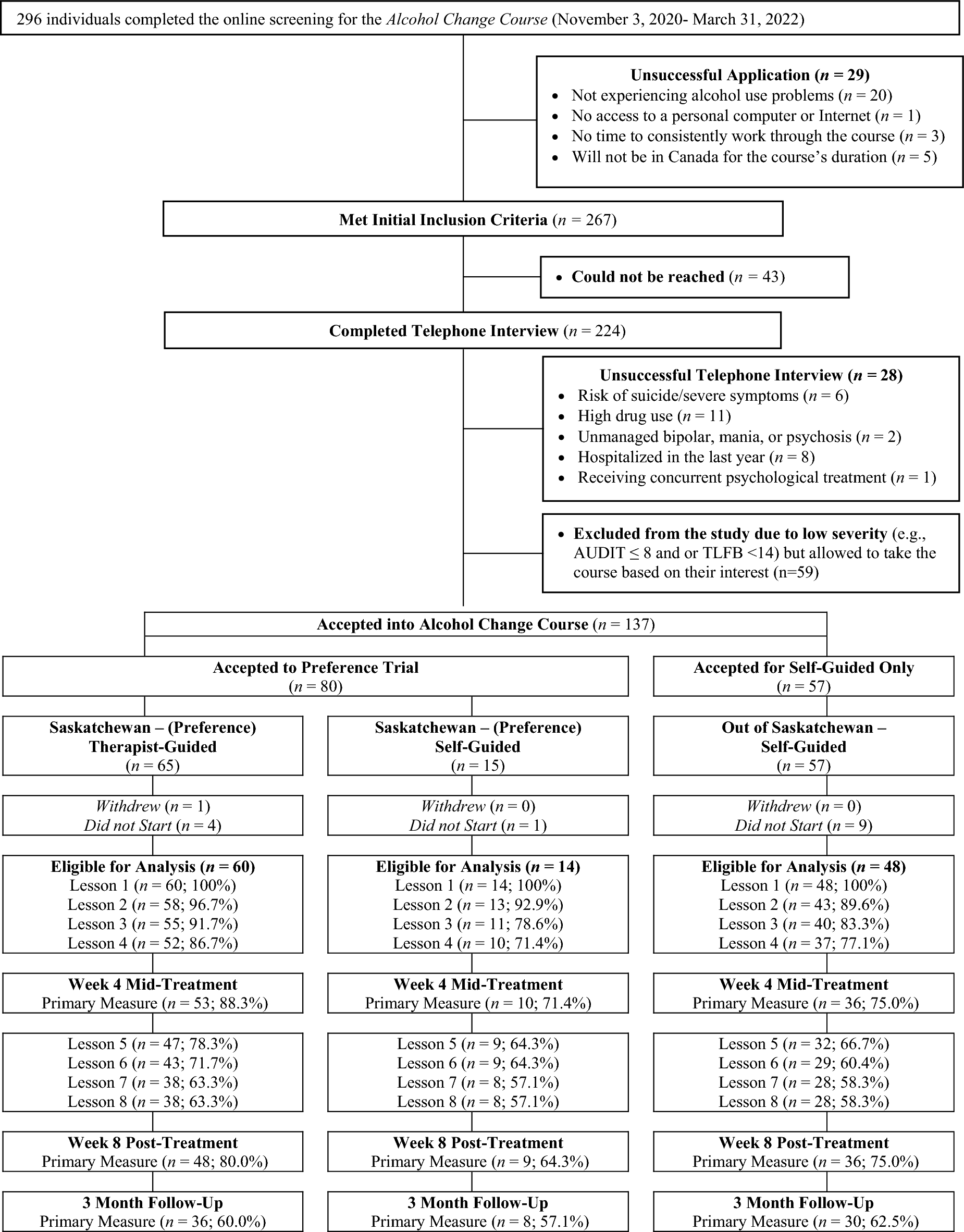
Fig. 1
Pathways linking national to local initiatives to expand access to MOUD.
Table 1 Processes mapped to established implementation constructs and strategies Setting the stage for practice changeIn 2017, the VA and Department of Defense (DoD) jointly published clinical practice guidelines addressing the use of long-term opioid therapy for chronic pain [32]. Similar to 2016 Centers for Disease Control and Prevention guidelines on opioid prescribing, VA/DoD guidelines recommended routinely evaluating the need to continue long-term opioids for chronic pain with guidance to reduce or discontinue opioids when risks exceeded benefits [33]. While not addressing OUD treatment specifically, this guidance from the outer setting had significant implications for primary care clinicians’ perception of the need to offer MOUD in primary care. As one clinician noted, implementing the new guidelines necessarily meant that, “…we’re going to unearth more people with opiate use disorder and [there would]…be a need to offer them options for a treatment.” At the time, no providers in this health system were prescribing buprenorphine within primary care, although several had completed the DEA waiver training. While patients could access specialty care according to the VA’s Stepped Care Model for Opioid Use Disorder [4], establishing care with specialty OUD services required patients to self-schedule a lengthy intake visit limited to certain time slots during the week. This requirement presented barriers for some patients. Moreover, primary care providers lacked a venue to communicate or consult with specialists in OUD treatment outside of the electronic health record (EHR). These gaps meant that, despite pressures to taper long-term opioids, clinicians had limited options to treat patients who began to exhibit symptoms of OUD during the taper process. As one clinician remarked, “we were consistently running into this situation of these patients that we were kind of on the treadmill with and getting nowhere.”
A second outer setting change, initiated by local primary care leadership and implemented by the Clinic Practice Manager, further heightened clinicians’ awareness of the lack of OUD treatment capacity within primary care. The new initiative linked opioid metrics (e.g., percent of completed urine drug screens, reviews of the state prescription drug monitoring program database, and naloxone prescriptions) with physicians’ performance pay. In response, one primary care clinician described a group email thread he had sent to local leadership asking what would be done to address a patient with OUD identified through such processes, “I…raised the question… ‘should we really…[be] putting effort into identifying more people if we don’t put parallel effort into making more treatment accessible to them?… I kind of felt that it wasn’t ethical to… identify people without having treatment options available.” The change in national guidance and local performance pay incentives regarding opioid prescribing highlighted gaps in MOUD treatment availabilty and helped to alter clinicians’ perceptions of the need for a change.
Starting a primary care-based Buprenorphine ClinicBelief in the need for change was a necessary but not sufficient pre-condition for practice change to take place. What was crucial in this context, as has been identified in others, was the willingness of a Champion to take on the heavy lifting of moving the clinic from idea to reality [19, 34, 35]. At first, no one stepped forward to lead change efforts despite a general consensus that increased access to MOUD was needed and that the best next step would be to increase MOUD availability in the primary care setting. As one clinician described, “I think if everybody was lukewarm and there wasn’t somebody that was [really pushing]… I mean, everybody’s busy, there’s a billion other things to do. If you have many lukewarm folks about a particular topic, there’s no way for people to overcome the activation energy it’d take to…do something new.” Another clinician, who eventually took on the role of Champion, concurred, while also acknowledging that committing to the role had not happened immediately, “It was one of those things where it’s like a good idea, but no one really has… the time or capacity to really take it on. And, I put myself in that category also, for a while…” Yet as time went on, she became increasingly enthusiastic, in part due to fortuitous participation in a federally-funded systematic review addressing barriers to OUD treatment [20]. As she described, “[of] everything I’m doing, I now feel the most passionate about this one thing… From a public health and…social justice standpoint… it’s very clear to me that this is…a service [primary care buprenorphine] that we should be providing.” Her research coupled with the work of planning and soliciting support for expanded access to MOUD activated this clinician to take on the role of Champion.
Beginning in 2017 and through 2018, the Champion began meeting with specialists and administrators to understand where and how MOUD was already being offered within the larger health care system and what steps would be needed to start prescribing buprenorphine within the medical center’s primary care clinic. These meetings helped generate momentum for the idea of creating a Primary Care-Based Buprenorphine Clinic and obtain buy-in from stakeholders in the substance use disorder, pain management and mental health clinics, the other locations offering OUD treatment with buprenorphine. Seeing that some momentum was building encouraged other primary clinicians who were interested, but did not have time to do this groundwork themselves, to lend their support for change. The Champion, a small number of other interested primary care clinicians, the Clinic Practice Manager, a specialist from the substance use disorder clinic, and a pharmacist began meeting monthly to discuss how to overcome logistical barriers to implementing a new Clinic. Barriers discussed in these meetings included limited clinic space, staffing issues, and determining the future clinic’s patient capacity and scope, “There was a lot of, like…we want to do this, but who’s going to do it and how’s it going to be done?” The Champion was hesitant to lead the clinic on her own, “[It]…felt a little daunting just to say, like I’m going to do it all!” A turning point came when the pharmacist suggested that a second year Pharmacy Resident rotate in the clinic to gain OUD treatment experience (under the supervision of a Pharmacy Preceptor) and a second primary care clinician committed to co-directing the clinic with the Champion (hereafter referred to as the Clinic Co-Director). With this staffing in place, the team finalized the model to be implemented for buprenorphine care delivery: a clinician-pharmacy collaborative care model.
This model had precedent in the VA system, in which clinical pharmacists and primary care providers often collaborate on treatment plans for patients with chronic diseases such as diabetes, high blood pressure or chronic pain [36, 37]. In order to preserve the clinic’s capacity for new patients, the Champion or Clinic Co-Director would meet with patients initially to outline the care plan, and follow-up visits would be conducted by the Pharmacy Resident (with oversight from Champion or Clinic Co-Director and the Pharmacy Preceptor). Although the Pharmacy Resident could not prescribe buprenorphine, it was in the resident’s scope to ask patients about medication effectiveness, adherence, and side effects as well as order urine drug screens for treatment monitoring. The model was consistent with the primary care clinic’s established function as a teaching clinic and provided learners with substance use disorder treatment experience, “this gives the residents a leg up…when they graduate…they already have that little bit of experience with the SUD clinic that could be transcribable into the full practice.” Although the learners in this case would be pharmacy residents (rather than medical residents), the fact that the proposed clinic would meet an educational need helped garner support for the model from local primary care leadership. Concretely, support from the Clinic Practice Manager consisted of dedicating physical space for the clinic one morning/week and allowing for a reduction of about 100 patients in their usual primary care panel for both the Champion and Clinic Co-Director (without additional compensation or protected time). Nursing staff also agreed to support the clinic with patient check-ins and rooming, although the Champion and Co-Director pledged to provide some of this support themselves to avoid over-burdening nursing staff.
Initially the clinic planned to exclusively treat patients who were in sustained remission from OUD transferring from specialty care. OUD specialists viewed this as a beneficial expansion of “step-down” services and an appropriate starting point for primary care clinicians who lacked buprenorphine prescribing experience. As one pharmacy resident described, “…for us starting out… you want patients who have proven to be very stable and not had issues…” Such patients were thought to require fewer supportive services and less frequent touch-points, a treatment approach that was seen as more compatible with primary care practice, which lacked the ability to provide intensive case management. Further, it was decided that patients’ OUD care would be maintained by clinicians in the buprenorphine clinic, rather than transferred back to patients’ primary care clinician. In the clinic planning process, primary care clinicians and specialists in OUD agreed to maintain open lines of communication and discuss patient transfers back to a higher level of care—specialty substance use disorder treatment—when appropriate. In January of 2019 the Primary Care-Based Buprenorphine clinic was launched.
Expanding capacity and scopeAbout a year after the Primary Care-Based Buprenorphine Clinic had been initiated, the core team comprised of the Champion, Clinic Co-Director, other interested clinicians and pharmacists turned to the question of how to further expand access to OUD treatment for patients seen elsewhere in the health care system (e.g., for hospitalized patients, those seen in rural clinical settings). Such settings lacked a consistent process for providing MOUD and engaging patients in ongoing treatment, and some clinics lacked buprenorphine prescribing capacity. One clinician proposed, and received support from leadership to host, a half-day “Buprenorphine Summit” in January of 2020, which was intended to engage clinicians throughout the system in discussion of gaps in treatment availability, and strategies to overcome them. Fortuitously, just before the Summit was scheduled to convene, national VA leadership disseminated a directive mandating that all VA sites begin prescribing buprenorphine within 60 days of receipt of the notice [38]. While in the past local leadership had been hesitant to integrate buprenorphine treatment into clinical settings beyond specialty SUD, mental health, and the nascent Primary Care-Based Buprenorphine Clinic, “leadership was concerned that if we open up care for buprenorphine that…will gobble up appointments and we won’t be able to provide care for other veterans who want to get into the VA…,” with the publication of the notice, “there was impetus to move forward.” The national directive also had implications for local funding decisions, as one clinician described, “If this is a priority for the VA, you can justify the resources for that.” Support from local leadership was evident at the Summit. Not only were leaders from primary care, mental health, emergency medicine, pain management, and pharmacy in attendance, but as the Summit convened, the health system chief of staff provided introductory remarks emphasizing her strong support for the Summit’s goals.
A key component of the Summit was discussion of a series of hypothetical cases, designed to highlight existing gaps in MOUD availability, and the barriers to connecting patients to treatment. For instance, one case presented a patient with OUD receiving care in a rural clinical setting who lacked a clinician certified to prescribe buprenorphine. Another case discussed how to continue buprenorphine for a patient who started buprenorphine while hospitalized but lacked an outpatient provider. The case discussion provided a forum for clinicians to consider the appropriate clinical home for patients with diverse needs and come to agreement on responsibilities across primary care and specialty clinics, which had been somewhat poorly defined in the past. The public nature of the forum also placed a subtle group pressure on clinicians to step up to fill these gaps as they were able; at one point the Champion asked whether anyone would be willing to volunteer to fill a particular role and waited through silence until someone came forward.
Finally, participants reviewed and discussed a variety of possible approaches to expanding access to buprenorphine to satellite primary care clinics and other clinical settings. Prior to the Summit, the organizers had distributed an informal survey via email to clinicians to inquire about their interest in and current use of buprenorphine for OUD. The email also asked what kinds of supports would increase clinicians’ willingness to prescribe buprenorphine. During the Summit, results of the survey were used as a starting point for the discussion. The Champion presented several possibilities (e.g., an E-Consult service, a hub and spoke model, visiting experts to assist outlying or rural clinics), and other attendees generated additional ideas (e.g., a buprenorphine road show, a mock drug enforcement agency audit). The E-Consult generated the most enthusiasm from attendees and the decision was made to move forward with planning. By providing space for participants to brainstorm solutions, the Summit encouraged collaborative problem solving and spurred investment in the proposed initiatives by bringing participants into the planning and development process.
The E-Consult serviceIn follow-up planning meetings, the core team discussed E-Consult staffing, scope, design and implementation. Fundamentally, it was decided that the E-Consult would be created within the EHR, made available to all clinicians within the health system and encourage questions regarding how to establish an OUD diagnosis, initiate buprenorphine and approach care transitions, thereby providing, “immediate access mentoring.” The Champion and Clinic Co-Director took ownership of the E-Consult process including the responsibility to respond to consults within the EHR. Because the Primary Care-Based Buprenorphine Clinic was not yet at capacity, the Champion and Clinic Co-Director did not receive additional protected time to manage the E-Consults and instead wrapped this work into their other clinical responsibilities. As a compliment to the E-Consult process, the core group established a twice weekly 30-minute meeting to address questions such as, “what’s the appropriate avenue for this patient, I’m considering buprenorphine therapy,” or, “they’re on buprenorphine therapy and I’m not sure what to do with them.” Attended on a voluntary basis by other clinicians from primary care, mental health, the substance use disorder clinic, and the pain management clinic, this ad hoc interdisciplinary team worked together to determine the appropriate clinical care setting for each patient:
“There’s fluidity in that, so if it doesn’t seem to work in one setting maybe we can move into another…we have…buy in from [the specialty substance use disorder treatment program], from primary care, from inpatient service, we’re trying to get ED involved… the pain clinic… the patient could fit into any of those situations and…we have a mechanism to talk it over and try and make a fit for the patient.”
The E-Consult Service facilitated care coordination by creating a centralized hub for case discussions, thereby addressing multiple systemic issues from lack of communication among clinicians to a lack of treatment capacity in some clinical settings. As one clinician described, “we’ve kind of broken the barriers and silos around care for these patients.” While the resolution for some E-consults might be to schedule a visit in the Primary Care-Based Buprenorphine Clinic, the E-consult process also facilitated patient hand-offs to the substance use disorder and pain management clinics. In some cases, the group might also provide recommendations for ongoing treatment in primary care.
Taking stockThe Primary Care-Based Buprenorphine Clinic saw its first patients in early 2019 and the E-Consult process was finalized just over 1 year later, in February of 2020. Since that time, the landscape of MOUD treatment availability across the health care system has transformed. The Primary Care-Based Buprenorphine Clinic has become well-established, continuing to operate one morning/week, with plans to expand to another half-day. With increased experience, the clinic no longer only serves as a step-down clinic for “stable” patients with OUD, but rather functions as a bridge clinic for patients seen in the hospital or emergency department who need a higher level of care (e.g., in the substance use disorder clinic) but are awaiting appointment availability. In the 3-years the clinic has existed, it has served 65 unique patients and provided training opportunities for seven clinical pharmacy residents, 24 psychiatry residents, and other learners including addiction medicine and palliative care fellows. While Internal Medicine residents do not rotate with the clinic on regular basis, they often refer patients to the clinic and attend the twice-weekly team meetings. This form of collaboration has provided additional opportunities for teaching. The E-Consult Service continues to meet twice weekly and has consulted on 225 patient cases, helping to facilitate initiation or continuation of buprenorphine treatment and linking patients to the most appropriate sites of care. Moreover, with a shift to telework following the onset of COVID-19, the twice weekly case discussions shifted from in-person to virtual meetings, which allows participation from staff at remote clinic sites, thereby furthering the overall educational impact. Over the 3-year period in which these new clinical processes were developed and implemented, the health system has increased the percentage of patients with OUD on medication from approximately 35% to more than 50%. While this improvement cannot be attributed to the Primary Care-Based Buprenorphine Clinic and E-Consult alone, these services are now an integral part of the health system’s efforts to expand MOUD access.
For one member of the team, the intentionally slow, collaborative approach to practice change had been essential to the ultimate success of these efforts:
I think [the Champion’s] appropriately, taught me something about…building the community of providers that you need… hearing all the different sides of this and making sure everybody’s on board and taking…a patient approach... That’s the way to…have a longer standing…program in place that’ll fit in well with the rest of the organization.
While this particular clinician had initially advocated for a more “rabble-rousing” approach to system change, he later reflected that such an approach may not have yielded the institutional buy-in and program sustainability of the more cautious, methodical approach ultimately taken.
留言 (0)