In the present study, after 12 months’ administration of raloxifene, the BMD, which had increased after at least two doses of denosumab at 6-month intervals, decreased to the baseline level at all measurement sites. A significant increase in the CTx and P1NP levels was also observed. Patients with a low BMI, previous vertebral fractures, or low lumbar spine BMD before denosumab treatment showed a greater reduction in lumbar spine BMD after 12 months of follow-up raloxifene therapy.
Denosumab is a potent antiresorptive agent, but there are concerns about the “rebound phenomenon” that occurs when it is discontinued [26]. Bone density is lost rapidly [27], the suppressed BTMs rebound [28], and multiple vertebral fractures may eventually occur [12]. Therefore, several guidelines and position statements have recommended continuous administration of an antiresorptive agent to prevent the rebound phenomenon if denosumab is discontinued [7, 16,17,18, 29]. Among antiresorptive agents, intravenous infusion of zoledronic acid is primarily recommemded because of its high potency [16, 19,20,21, 30, 31]. The effects of alendronate [22] or risedronate [32] have also been reported. Although raloxifene has a weaker effect on increasing bone density than bisphosphonates, it is an antiresorptive agent-proved vertebral antifracture efficacy [7, 33]. Therapy with other antiresorptive agents is mandatory after discontinuation of denosumab. In such cases, bisphosphonates are generally recommended.
Discontinuation of denosumab may be necessary when compliance, because of potential side effects, is a concern, or if there are insurance reimbursement issues. In Korea, reimbursement is no longer provided if bone density increases to osteopenia levels, confirmed at all measurement sites, regardless of the treatment period. Therefore, when BMD increases with denosumab treatment, it must be discontinued and replaced with cheaper alternatives. However, it is specifically pertinent to Korea’s national health insurance reimbursement system and is not widely accepted by the international guidelines. In our study, 21 (34.4%) patients discontinued denosumab due to loss of reimbursement because their T-scores increased to osteopenia levels.
There is very little evidence on the effects on bone metabolism of follow-up therapy with raloxifene after discontinuation of denosumab. One case report suggested rapid bone loss after switching from denosumab to raloxifene, although the patients had also been exposed to multidisciplinary treatments for breast cancer [34]. Recently, Ebina et al. investigated the effects of raloxifene in patients previously treated with denosumab. The authors observed substantial bone loss after raloxifene treatment and reported that 23.1% of patients developed new vertebral fractures. However, this was a small study in 13 patients. Other study limitations were that vertebral fractures were confirmed only by the patients’subjective complaints, with no radiographic confirmation. In addition, the average age of the patients treated with raloxifene was 77.1 years [23]. The average age of the patients in our study was 65.7 years, and there may have been different responses to raloxifene.
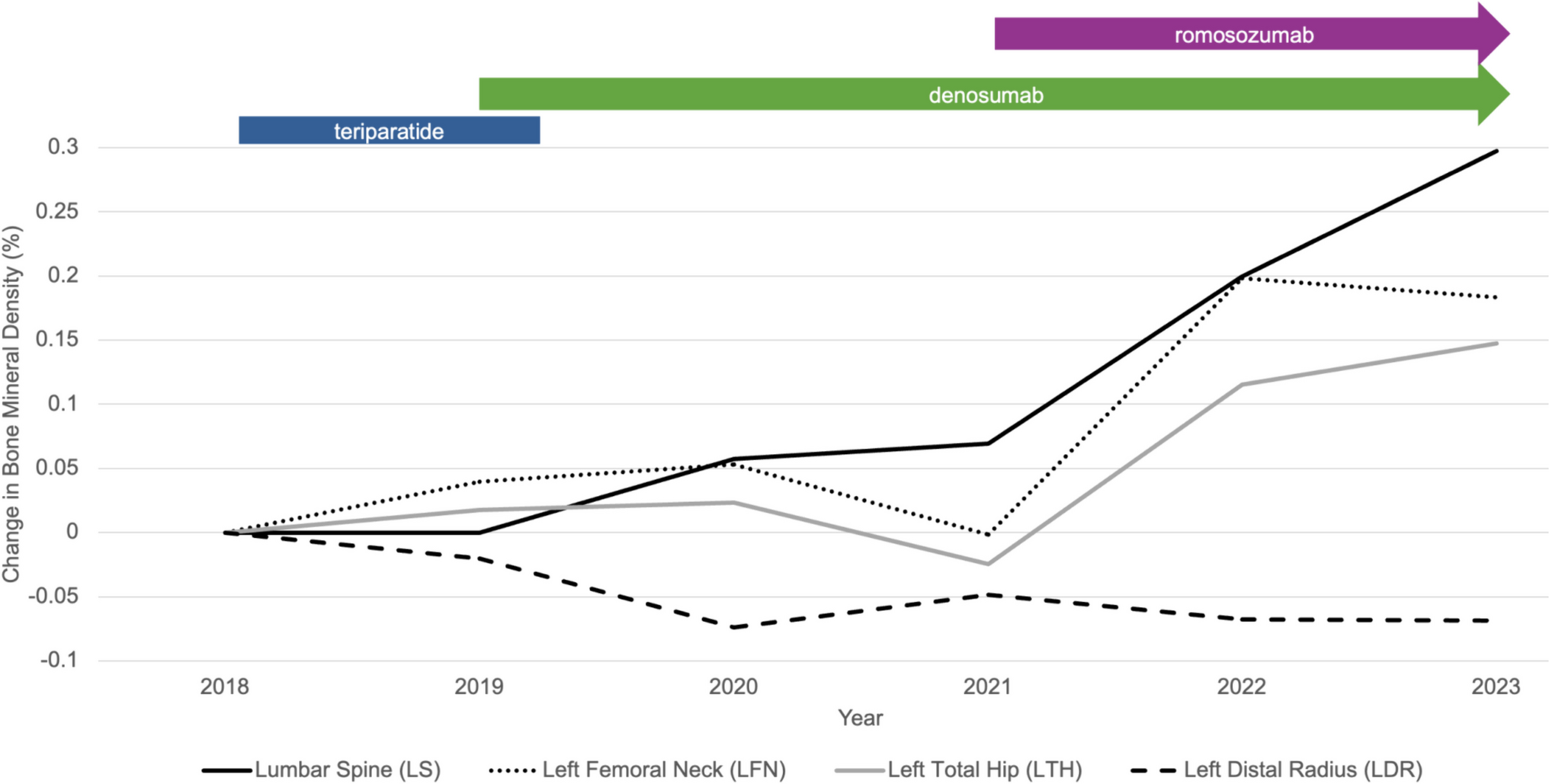
Bone loss was consistently observed after discontinuation of denosumab in our study, in line with the above reports [23, 34]. The lumbar spine had the greatest bone loss after 12 months of raloxifene treatment. In previous literature, the bone mass gained during denosumab treatment was lost, and the baseline value was reached within 12 months of the last denosumab injection if no treatment was given [27, 28]. The CTx level also increased to above the baseline values after denosumab discontinuation [28]. In our study, the administration of raloxifene did not prevent an abrupt increase in BTMs after discontinuation of denosumab. Reports of multiple vertebral fractures at 9–16 months after the last denosumab injection were associated with sudden bone loss and elevation of BTMs [9, 24, 35]. In our study, administration of raloxifene after discontinuation of denosumab did not effectively suppress the decrease in BMD or increase in BTMs. Interestingly, Bone et al. reported that femoral BMD decreased lower than the baseline value with discontinuation of denosumab [3]. In our study, with subsequent administration of raloxifene, the femoral neck BMD remained higher than the baseline value.
In the present study, the decrease in lumbar spine BMD was substantial after discontinuation of denosumab despite administering raloxifene. Bone loss in the lumbar spine was greater in patients with a low baseline BMI, prior vertebral fracture, or low lumbar BMD measured before denosumab treatment. A history of previous vertebral fractures is likely to be associated with a greater decrease in lumbar spine BMD after administration of raloxifene. Previous fractures were accompanied by overall microarchitectural deterioration as well as reduced bone quality [36]; hence, the discontinuation of denosumab may have more effects in patients with previous fractures. Therefore, caution may be required when switching denosumab to raloxifene in patients with prevalent vertebral fractures.
Moreover, BMD decreased significantly after raloxifene in patients who remained osteoporotic (T-score ≤ − 2.5) after denosumab administration. Therefore, raloxifene should be administered with caution when there is a high risk of fracture. If osteopenia is achieved with denosumab, the BMD decrease will be marginal after subsequent administration of raloxifene. Thus, the use of raloxifene is more appropriate in such cases. However, Kendler et al. reported that the greater the BMD percentage change after denosumab administration, the greater the BMD loss after subsequent alendronate administration [22]. A direct comparison is difficult because the participants in the study, the administered drug, and the administration period of denosumab are different; nevertheless, this result should be confirmed in future studies.
Our study has some limitations. First, this was a retrospective study with a lower level of evidence than that of a prospective study. Second, our study did not include a control group that had no treatment after denosumab was discontinued. However, not taking any follow-up treatment after discontinuing denosumab may raise ethical issues given the known problems. Therefore, we indirectly compared the data after discontinuation of denosumab to data in the existing literature, although the analysis groups were different. A comparison of SERMs with various active comparators after discontinuation of denosumab will also be an interesting research topic. Third, patient compliance was not assessed in this study. All patients included in the analysis had timely follow-up without loss; however, the lack of confirmation of drug compliance is a limitation. Fourth, lumbar spine anteroposterior and lateral radiography were conducted to confirm vertebral fractures, but there were limitations in confirming vertebral fractures in all areas, including the thoracic spine. Lastly, the relatively short study period and the small number of patients with fractures are also limitations. Additionally, it is necessary to consider the rebound phenomenon according to the duration of denosumab administration. These shortcomings can be resolved through future long-term prospective studies.
Administration of raloxifene for 12 months after denosumab discontinuation did not maintain the increased bone mass, and BTMs rebounded. Moreover, the reduction in lumbar spine BMD was greater in the patients who had vertebral fractures before denosumab administration or those who had a lower lumbar spine BMD or lower BMI. In conclusion, raloxifene sequentially administered after denosumab discontinuation is not effective in preventing rebound phenomenon. We believe that this is a novel finding. These findings need to be validated by a prospective study to draw clear conclusions regarding the sequential treatment with denosumab-SERMs.




留言 (0)