
記住我

Trichosporon species have been recognized as emerging opportunistic yeasts. They are commonly found on the skin and in the gastrointestinal flora of humans in temperate and semitropical climates (1). However, Trichosporon spp. can cause invasive and life-threatening fungal disease in immunocompromised hosts (2).
An exceedingly rare representative of this genus, Trichosporon japonicum, was first isolated in 1971 from the air of a microbiological laboratory in Japan and named by Sugita and Nakase in 1998 (3). The first clinical case was published in 2008, describing a T. japonicum related fungemia in a child with acute myeloid leukemia (AML) (4). In this report, we present a case of T. japonicum infection in a pediatric patient with refractory acute B cell lymphoblastic leukemia. Due to the rarity and growing importance of T. japonicum, here, we discuss a case which represents the second complete clinical and mycological resolution of T. japonicum blood infection amongst all case reports in literature to date (5).
Case Description Patient HistoryAn 8-year-old boy was admitted to Bambino Gesù Children's Hospital in October 2020 with a diagnosis of refractory acute B cell lymphoblastic leukemia (ALL) for chimeric antigen receptor (CAR) T-cell therapy in preparation for hematopoietic stem cell transplantation. The diagnosis of ALL had been made in March 2019 in the country of origin of the patient. Subsequently, he had been started on treatment with the first-line chemotherapy protocol (Total XV protocol) which was interrupted due to disease progression. Thereafter, two cycles of Blinatumomab had been tried, however, the second one had been interrupted because of another relapse. Following that, the patient had been given hyperfractionated cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride, and dexamethasone (hyper-CVAD) plus inotuzumab ozogamicin. Finally, he had been transferred to our hospital in Rome.
During his stay in our center treatment was initiated with bridging chemotherapy and bortezomib, followed by two CAR T-cells infusions with poor response. Bone marrow aspirate performed as per protocol 4 weeks after the second infusion of CAR T-cells revealed 90% of CD19-negative blasts. Thus, a therapeutic failure was declared at the end of the fourth month of hospital stay.
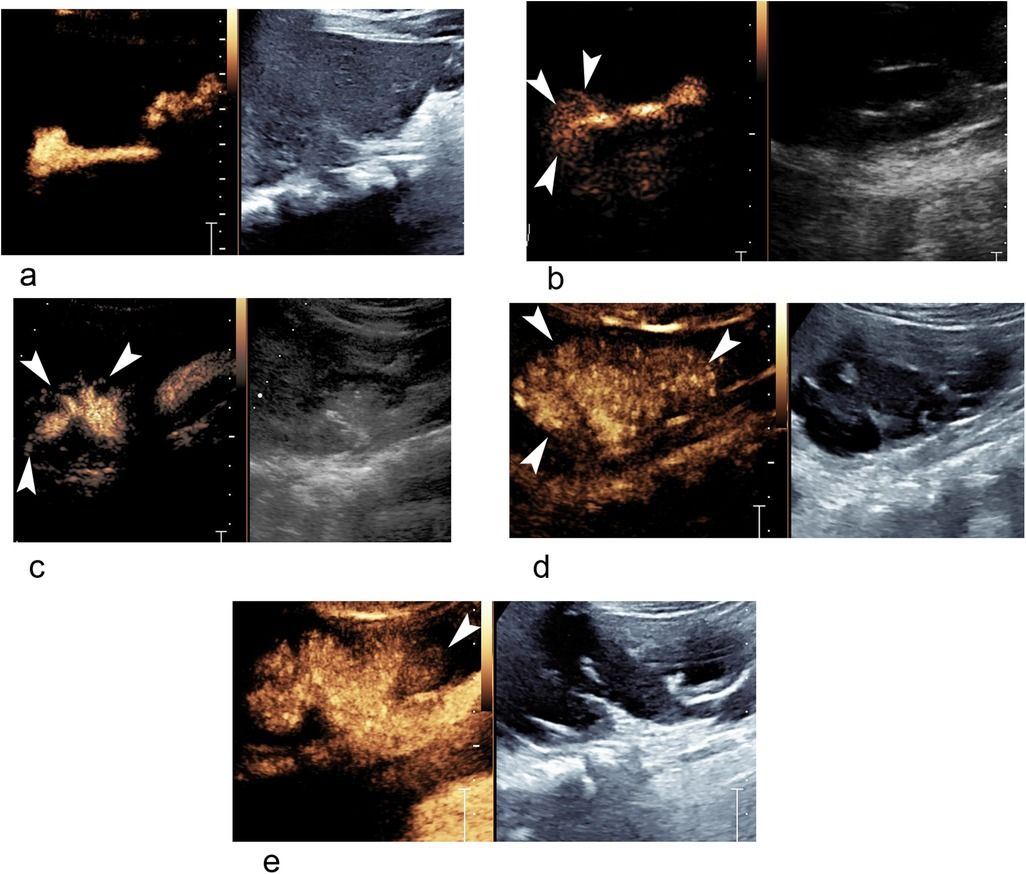
Diagnostic Assessment and Therapeutic InterventionIn the fifth month of admission, the patient, who was on amphotericin B (AMB) long-term prophylaxis (3 mg/kg intravenously once a day), developed fever, acute respiratory distress and cutaneous lesions suggestive of septic emboli on day 1 (Table 1). High level of C-reactive protein (CRP) was measured at 34 mg/dL. In parallel, blood culture (BC) samples were taken from central venous catheter (CVC) for identification of a potential bacterial infection, as well as for fungi detection; all were processed on BD BACTEC™ FX. No Candida species were detected on the T2Dx Instrument (T2 Biosystems). Of note, caspofungin (50 mg/m2 intravenously once a day) was added to AMB on the same day. On day 2, a whole body computed tomography (CT) showed multiple bilateral lung nodules and micronodules, mainly in centrilobular distribution with confluence in some areas. Evaluation of CT raised suspicion of mycobacterial infection and led to the analysis of expectorated sputum samples and gastric aspirates, which all resulted negative. There was no evidence of central nervous system (CNS) involvement. BCs were repeated on days 2 and 3; together with the BC taken on day 1, they all became positive for fungi on days 4 and 5, respectively. The first hypothetical identification was done by phenotypical microscopic observation (Figure 1). The isolate was then identified as T. japonicum by matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS, Bruker Biotyper) with a high score value of 2.05. It was further confirmed by molecular typing, using MicroSEQ™ 500 16S rDNA PCR Kit (ThermoFisher SCIENTIFIC) and repeatedly detected on days 4 and 5. Antifungal susceptibility testing was performed according to Clinical and Laboratory Standards Institute (CLSI) guidelines. The isolate of T. japonicum displayed presumed variable susceptibility as evidenced by the following minimum inhibitory concentrations (MIC): anidulafungin (>8 μg/mL), caspofungin (8 μg/mL) and micafungin (>8 μg/mL); AMB (0.25 μg/mL); fluconazole (1 μg/mL), itraconazole (0.12 μg/mL), posaconazole (0.12 μg/mL), isavuconazole (0.06 μg/mL), and voriconazole (0.03 μg/mL). Based on the antimycogram, caspofungin was changed to voriconazole (8 mg/kg intravenously twice a day) on day 5, while AMB was continued at the same dose. It is important to note that the patient remained neutropenic (neutrophils <100/μL) during all the hospital stay, including the episode of fungemia, and did not recover the neutrophil count upon treatment.
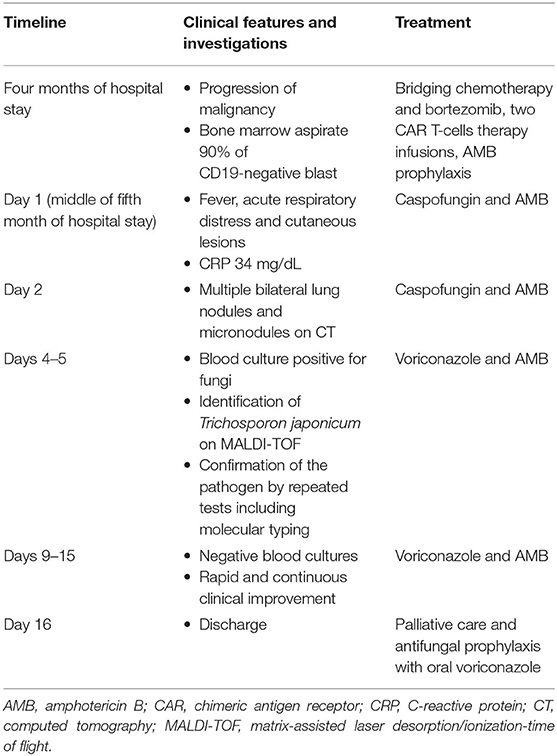
Table 1. Timeline of Trichosporon japonicum fungemia course.
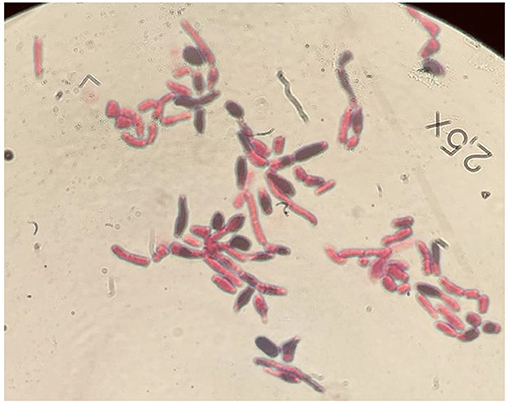
Figure 1. Microscopic appearance of T. japonicum isolates with Gram stain using RAL-stainer, magnified 100 times.
We analyzed all samples in which this yeast was isolated from BCs between days 1 to 15. There was a rapid clinical improvement with a complete resolution of symptoms and the infection was cleared by day 14 as confirmed by repeatedly negative BCs. Nevertheless, due to progression of ALL, it was decided that further treatment should focus only on palliative care. The patient was discharged on antifungal prophylaxis (voriconazole 150 mg by mouth twice a day) and came back to his country of origin where he died 3 weeks later due to the underlying malignancy.
DiscussionThe genus Trichosporon is composed of ~50 species which are widely present in nature (soil, air, seawater); 16 species have been identified as human pathogens of which T. japonicum has been isolated from different sources such as biopsy, skin, sputum, vaginal mucosa, bile, urine, pleural fluid, nails (6, 7). To date, only two clinical cases of T. japonicum isolated from blood samples have been described in the literature (5, 8). One case was reported in an adult with hematological malignancy who had undergone hematopoietic stem cell transplantation. The infection was catheter-related, which was later removed, and it contributed to death; treatment with liposomal AMB was not adequate (8). Additionally, the very first clinical case concerned a child with AML post bone marrow transplantation. Multiple yeasts were isolated from sputum cultures, therefore, she was treated with liposomal AMB and itraconazole. T. japonicum was only identified after her death (4). These cases illustrate the difficulty and delay in accurate diagnosis of T. japonicum infection along with the associated high mortality.
Little is known about factors related to T. japonicum virulence. Thermotolerance is a key feature of pathogenicity in yeasts as it allows them to switch from commensal to a pathogenic lifestyle (2, 7). Our results demonstrated that isolates of T. japonicum grow at 30°C as well as 37°C (Figure 2). Another known virulence factor of Trichosporon spp. is biofilm formation; it has been studied lately in relation to antifungal susceptibility (9). In this regard, Agirbasli et al. described a case of significant biofilm formation in T. japonicum (4).
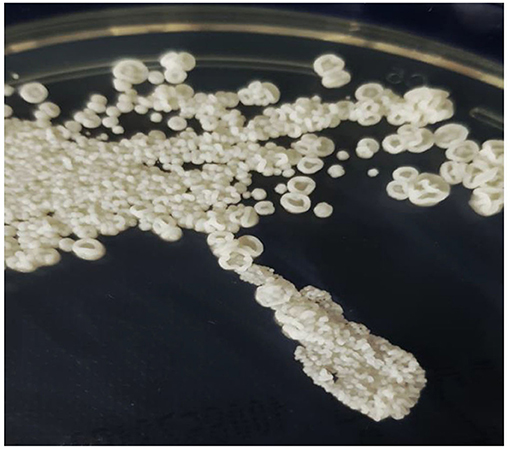
Figure 2. Trichosporon japonicum colony morphology, grown on Sabouraud-gentamicin-chloramphenicol-2-agar (SGC2) at 30◦C for 4 days (bioMérieux).
Invasive Trichosporon infections often cause breakthrough fungemia with high mortality rate particularly in patients with hematological malignancies. These bloodstream infections are primarily associated with the presence of a CVC (10). However, it is somehow tricky to determine the source or portal of entry of the yeast in our case since the symptoms resolved and fungal BCs were repeatedly negative while the CVC was preserved until the end of the patient's hospital stay. In addition, no data suggested that the country of origin could be the reservoir of T. japonicum.
There is an increased resistance of Trichosporon spp. to antifungals as commonly reported in literature (11). Data obtained by Francisco et al. revealed that Trichosporon genus exhibits high resistance to AMB which seems to be species specific (12). In our case, the isolates of T. japonicum showed high MIC for echinocandins and fluconazole, medium for AMB and multiple azoles while the most effective drugs were isavuconazole and voriconazole. The infection occurred despite the use of AMB prophylaxis; however, it was successfully treated with voriconazole given in combination with AMB. Even though the most recent global guidelines give only marginal recommendation for adding AMB to voriconazole (13), the clinical decision to use such combination treatment was supported by the profound aplasia and impracticability of CVC removal.
In this study, despite the conservation of the CVC and the underlying disease progression, a clearance of the fungal infection was obtained with the combination AMB-voriconazole regimen. We therefore demonstrate the important role of voriconazole as a valuable therapeutic tool against Trichosporon infections. In conclusion, regardless of the disease stage and presence or absence of clinical manifestations, we recommend a regular focused investigation for fungi and yeasts in neutropenic patients, expanding it beyond the species and genera subject to most common diagnostic procedures.
Patient PerspectiveThe parents of the patient gave their consent to all the treatment and the publication of the case report. Unfortunately, the perspective of the patient and their parents were not explored due to their return to the country of origin and terminal condition of the patient.
Data Availability StatementThe original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics StatementThe studies involving human participants were reviewed and approved by Ethics Committee of the Bambino Gesù Children's Hospital. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author ContributionsSA-N, MA, AK, LM, MO, BL, and GM contributed to study design, data collection, analysis and interpretation, and drafting and writing the manuscript. FQ, MC, and PM supported the study with their role and clinical expertise. FL followed the patient outcome and critically revised the manuscript. CP and PB were responsible for funding acquisition and supervised the project. All authors approved the final version to be submitted for publication.
Conflict of InterestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer RH declared a past co-authorship with the authors FL and PM and the absence of any ongoing collaboration with any of the authors to the handling editor.
Publisher's NoteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AcknowledgmentsThe authors thank Drs. Marta Argentieri, Laura Pansani, and Annamaria Sisto for their valuable comments on this manuscript. The authors are grateful for the technical staff, Anna Angelaccio, Vittoria Cetra, Francesca Di Leva, Maria Teresa D'Urbano, Giulia Ferri, Gianluca Foglietta, Carmela Parlavecchio, Silvia Tredici, and Ilaria Zullino of the Unit of Microbiology and Diagnostic Immunology, IRCCS Bambino Gesù Children's Hospital, for their outstanding support in collecting, processing samples, and performing laboratory analyses.
References2. Duarte-Oliveira C, Rodrigues F, Gonçalves SM, Goldman GH, Carvalho A, Cunha C. The cell biology of the trichosporon-host interaction. Front Cell Infect Microbiol. (2017) 7:118. doi: 10.3389/fcimb.2017.00118
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Agirbasli H, Bilgen H, Ozcan SK, Otlu B, Sinik G, Cerikçioglu N, et al. Two possible cases of Trichosporon infections in bone-marrow-transplanted children: the first case of T. japonicum isolated from clinical specimens. Jpn J Infect Dis. (2008) 61:130–2.
PubMed Abstract | Google Scholar
5. Bongomin F, Otu A, Calisti G, Richardson MD, Barnard J, Venkateswaran R, et al. Trichosporon japonicum fungemia and ventricular assist device infection in an immunocompetent patient. Open Forum Infect Dis. (2019) 6:ofz343. doi: 10.1093/ofid/ofz343
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Kalkanci A, Sugita T, Arikan S, Yucesoy M, Ener B, Otag F, et al. Molecular identification, genotyping, and drug susceptibility of the basidiomycetous yeast pathogen Trichosporon isolated from Turkish patients. Med Mycol. (2010) 48:141–6. doi: 10.3109/13693780902977984
PubMed Abstract | CrossRef Full Text | Google Scholar
7. do Espírito Santo EPT, Monteiro RC, da Costa ARF, Marques-da-Silva SH. Molecular identification, genotyping, phenotyping, and antifungal susceptibilities of medically important trichosporon, apiotrichum, and cutaneotrichosporon species. Mycopathologia. (2020) 185:307–17. doi: 10.1007/s11046-019-00407-x
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Álvarez-Uría A, Muñoz P, Vena A, Guinea J, Marcos-Zambrano LJ, Escribano P, et al. Fungaemia caused by rare yeasts: incidence, clinical characteristics and outcome over 10 years. J Antimicrob Chemother. (2018) 73:823–5. doi: 10.1093/jac/dkx436
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Cordeiro R de A, Aguiar ALR, da Silva BN, Pereira LMG, Portela FVM, de Camargo ZP, et al. Trichosporon asahii and Trichosporon inkin biofilms produce antifungal-tolerant persister cells. Front Cell Infect Microbiol. (2021) 11:645812. doi: 10.3389/fcimb.2021.645812
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Ramírez I, Moncada D. Fatal disseminated infection by trichosporon asahii under voriconazole therapy in a patient with acute myeloid leukemia: a review of breakthrough infections by Trichosporon spp. Mycopathologia. (2020) 185:377–88. doi: 10.1007/s11046-019-00416-w
PubMed Abstract | CrossRef Full Text | Google Scholar
11. de Almeida Júnior JN, Hennequin C. Invasive trichosporon infection: a systematic review on a re-emerging fungal pathogen. Front Microbiol. (2016) 7:1629. doi: 10.3389/fmicb.2016.01629
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Francisco EC, de Almeida Junior JN, de Queiroz Telles F, Aquino VR, Mendes AVA, de Andrade Barberino MGM, et al. Species distribution and antifungal susceptibility of 358 Trichosporon clinical isolates collected in 24 medical centres. Clin Microbiol Infect. (2019) 25:909.e1-909.e5. doi: 10.1016/j.cmi.2019.03.026
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Chen SC-A, Perfect J, Colombo AL, Cornely OA, Groll AH, Seidel D, et al. Global guideline for the diagnosis and management of rare yeast infections: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis. (2021) 21:e375–86. doi: 10.1016/S1473-3099(21)00203-6
留言 (0)