
記住我

Diffuse pulmonary ossification is an uncommon condition characterized by bone formation in the lung parenchyma. It is rarely diagnosed while the patient is still alive. Diffuse pulmonary ossification can be classified into dendriform (dendriform pulmonary ossification: DPO) or nodular types. It can be idiopathic or secondary to lung diseases and heart failure. Many DPO cases identified while the patient is still alive are pathologically diagnosed by surgical lung biopsy (SLB). It is difficult to diagnose DPO using transbronchial lung biopsy (TBLB) because we can collect only small tissues by TBLB. Transbronchial lung cryobiopsy (TBLC) is a new diagnostic procedure and is reported to have a high diagnostic accuracy for interstitial lung diseases. However, major complications associated with TBLC include pneumothorax and pulmonary haemorrhage. Although the incidence of these complications in TBLC is higher than that in TBLB, TBLC is considered less invasive compared to SLB. Here, we report the case of a patient who was diagnosed with idiopathic DPO by TBLC.
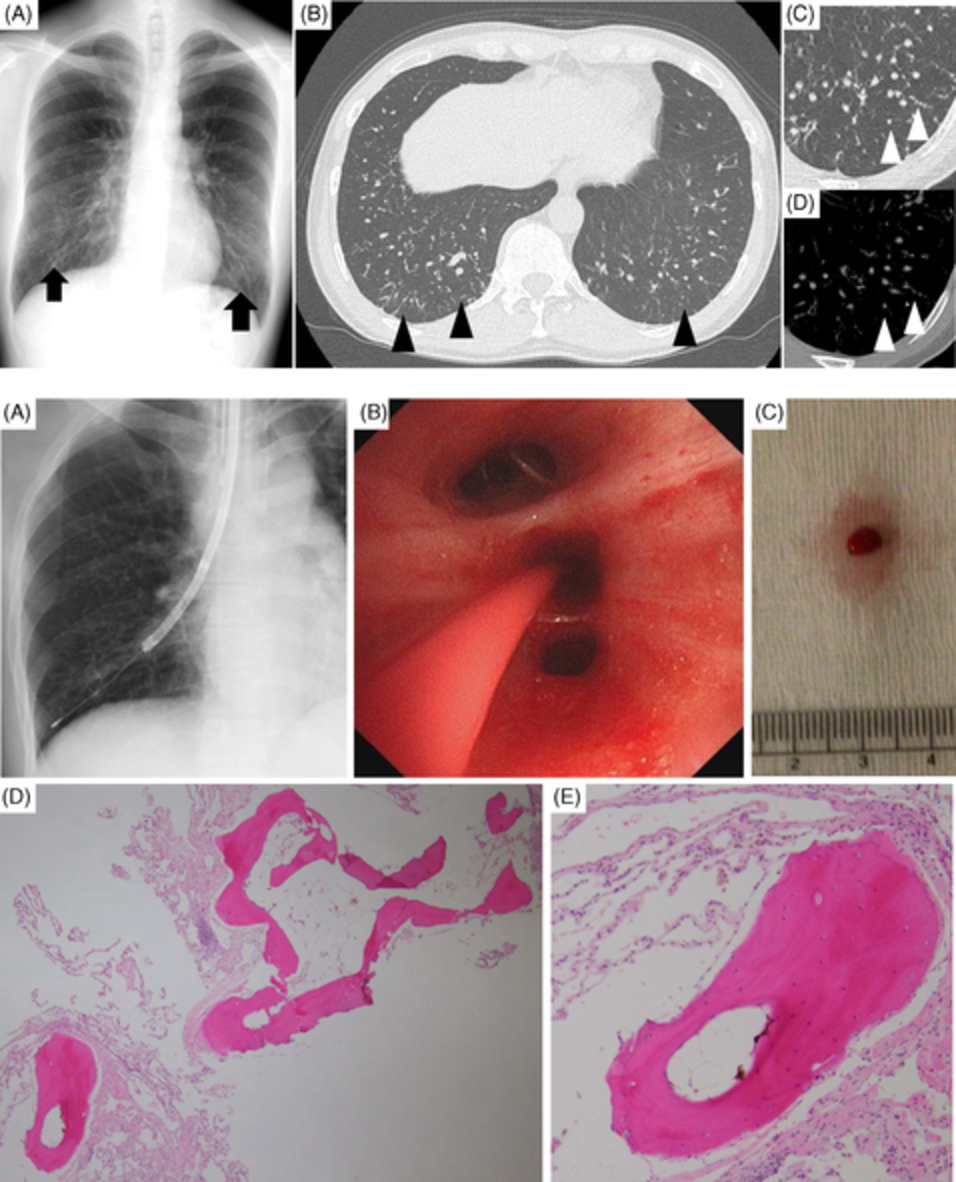
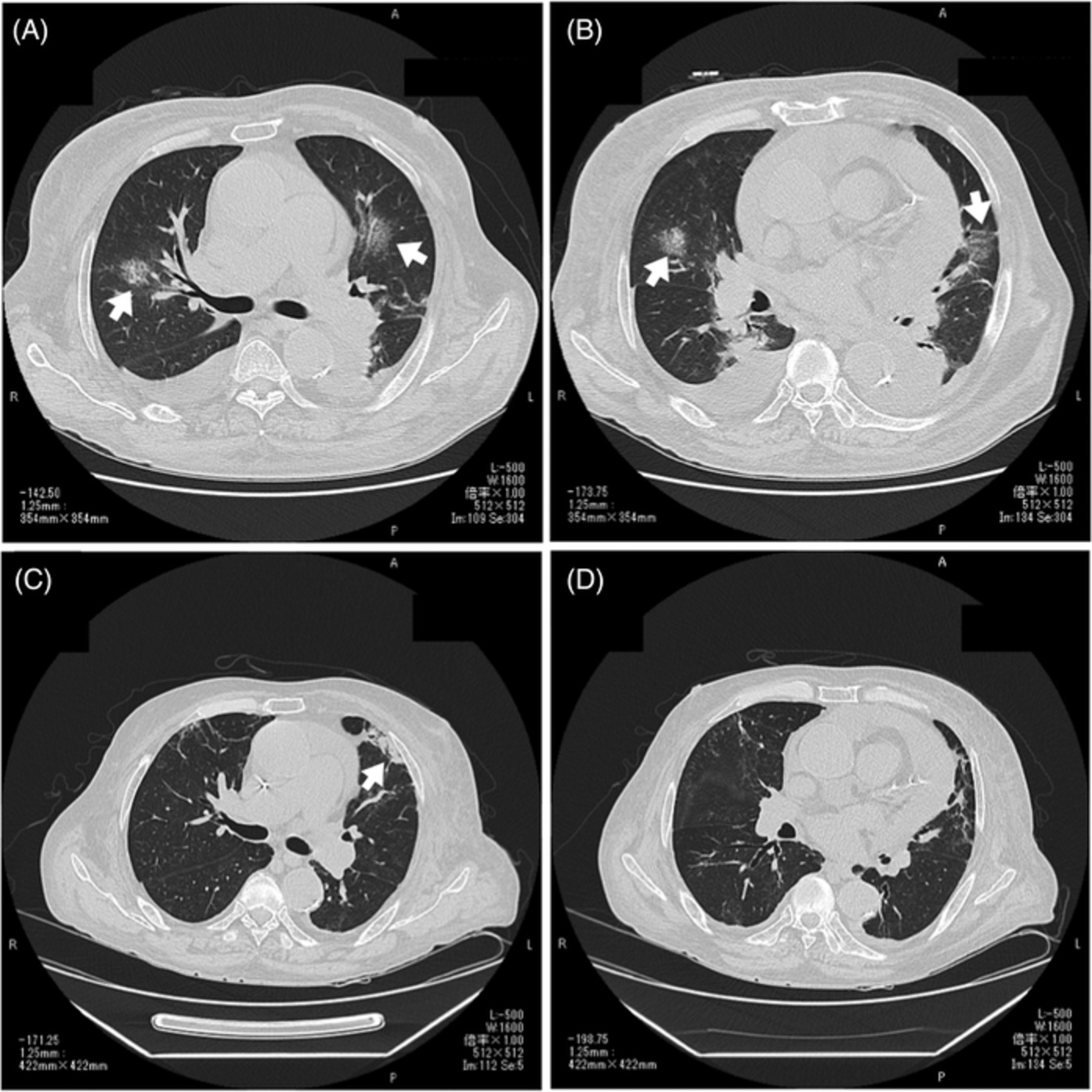
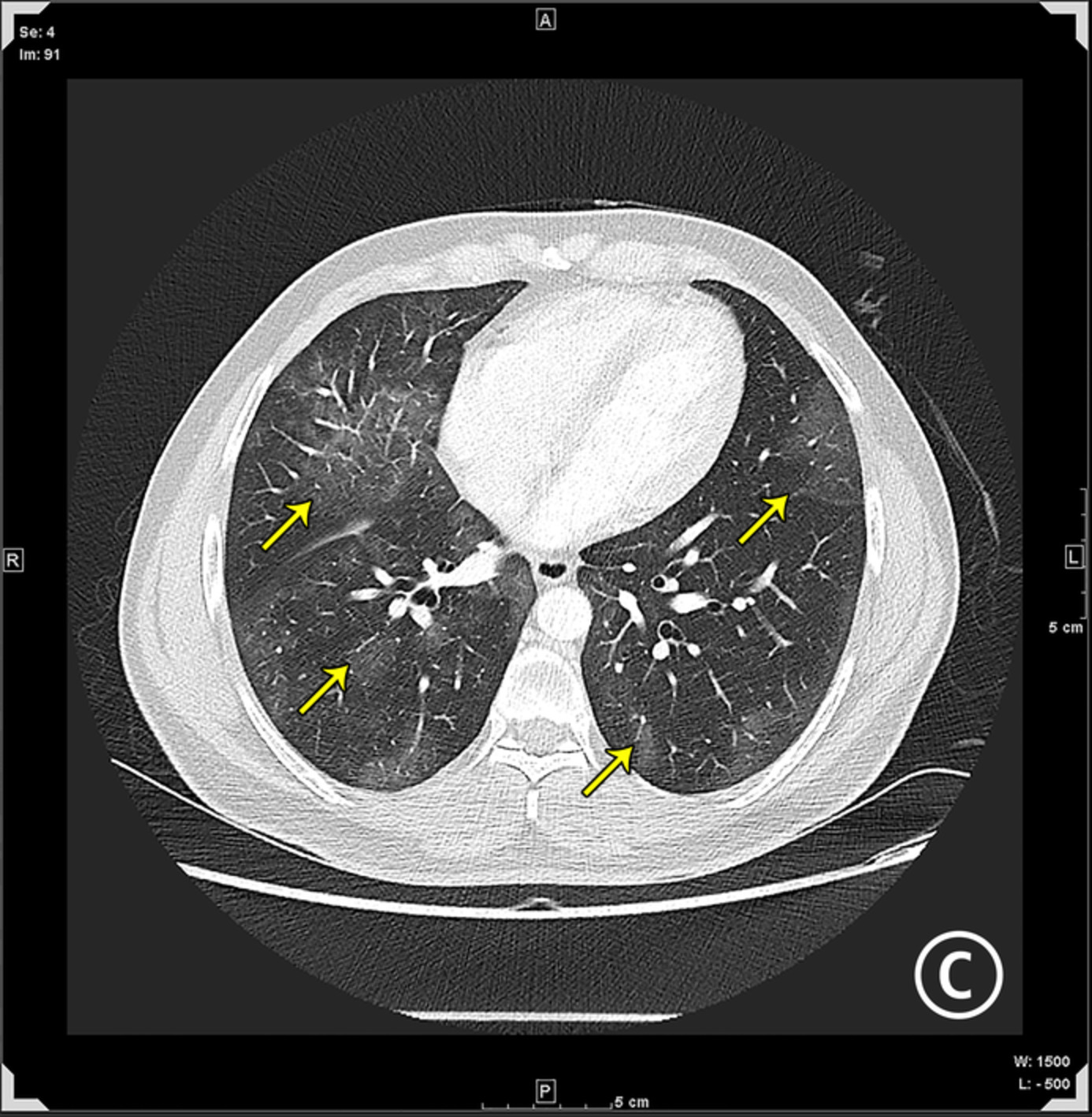
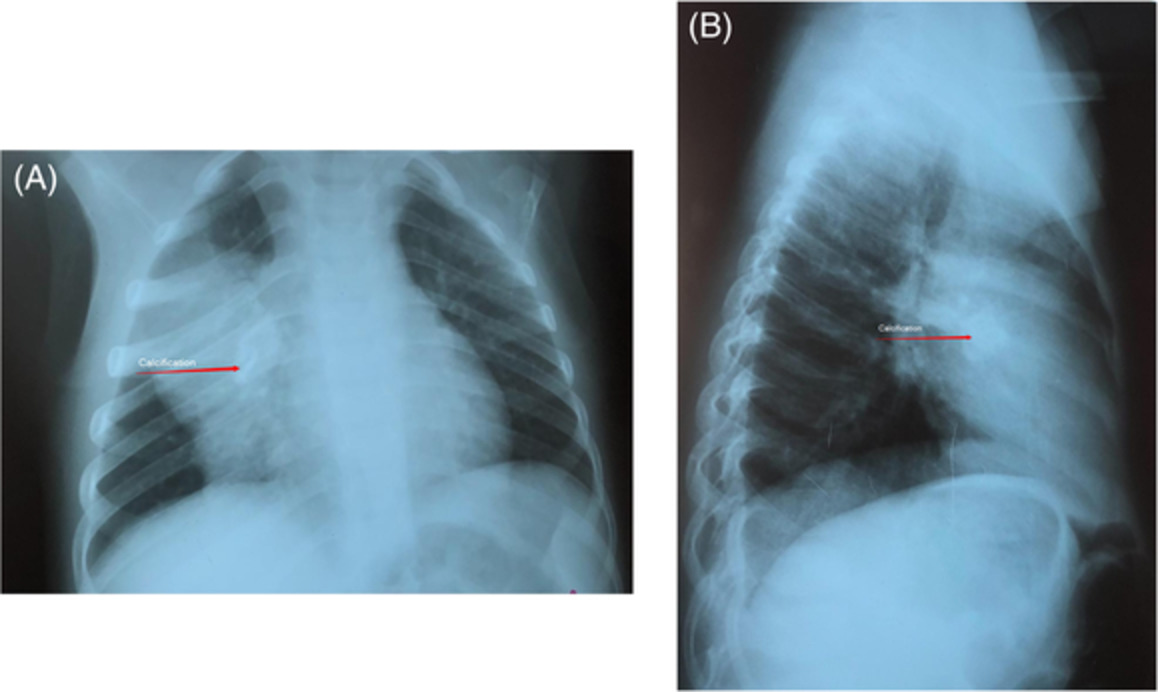
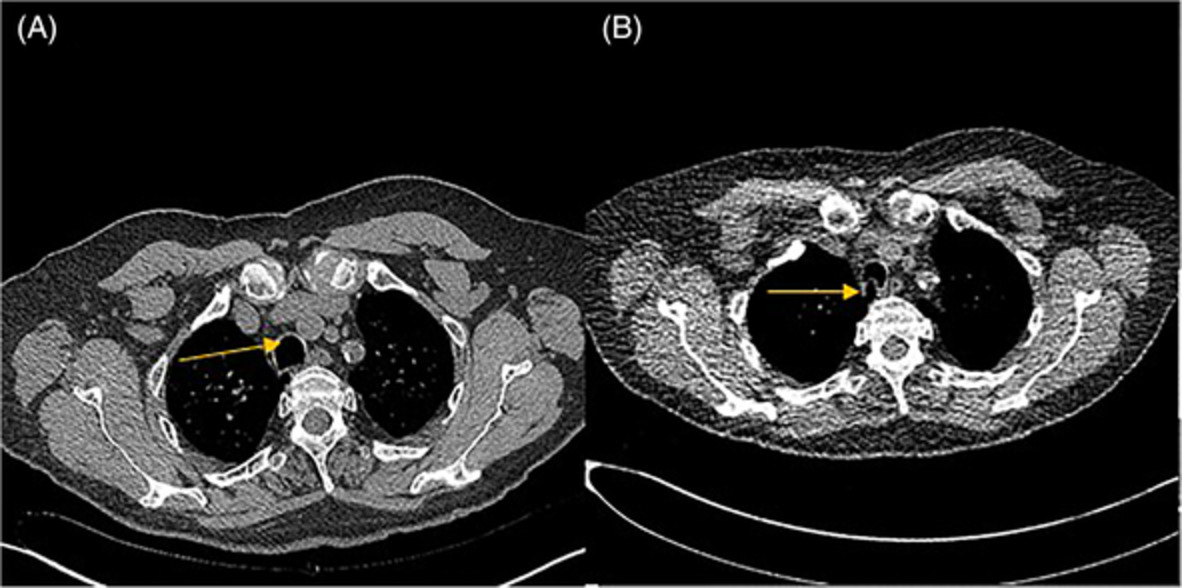
CASE REPORTA 37-year-old man visited our hospital due to abnormal findings on chest x-ray in medical examination. He reported no respiratory symptoms and no previous pulmonary disease. He was a non-smoker and had no family history of lung disease. His initial vital signs were normal. Physical examination, including the chest and lung findings, was unremarkable. His blood test, electrocardiogram and pulmonary function test were also normal. Chest x-ray revealed ground-glass opacities in both lower lung fields (Figure 1A). Chest high-resolution computed tomography (HRCT) revealed diffuse reticular shadows and micronodules mainly in the peripheral region, without lung shrinkage or traction bronchiectasis, on both lower lobes (Figure 1B). The density of the shadows in his computed tomography scans was indicative of bone or calcification by mediastinal window (Figure 1C,D).

Chest x-ray and high-resolution computed tomography (HRCT). Chest X-ray (A) revealed ground-glass opacities in both lower lung fields (arrows). Chest HRCT of the lower lobe (B) revealed diffuse reticular shadows and micronodules (black arrowheads). The density of the shadows (white arrowheads) in HRCT (C) was indicative of bone or calcification by mediastinal window (D)
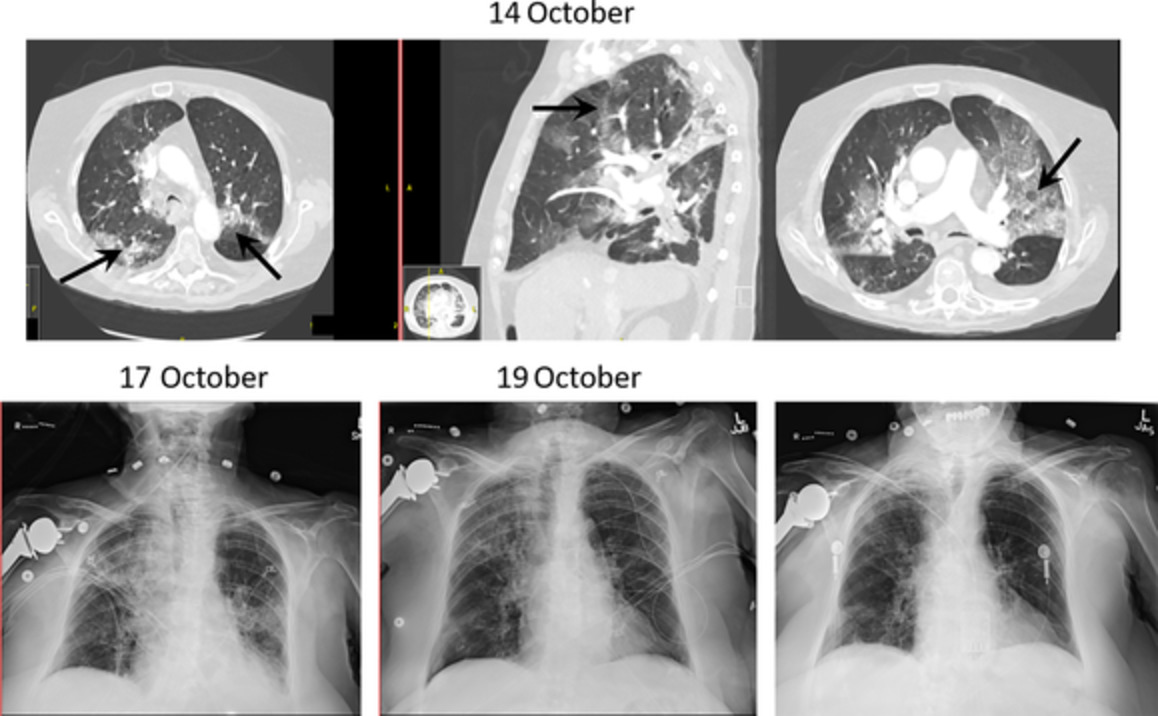
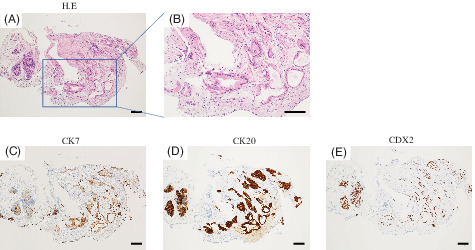
The patient underwent TBLC of the right lung's lower lobe (Figure 2A–C) for a definitive diagnosis, revealing a dendriform ossification with bone marrow in the lung parenchyma, without any other interstitial lung disease (Figure 2D,E). There was no evidence of secondary DPO; therefore, the patient was diagnosed with idiopathic DPO. There was no reported adverse event except for a small amount of blood in the sputum after the TBLC. After the diagnosis of idiopathic DPO, there was no progression of the chest radiological findings and no worsening of pulmonary function and respiratory symptoms. Therefore, the patient was followed up and managed conservatively.

Pathological findings of resected specimen by transbronchial cryobiopsy. The x-ray (A) and the views in bronchial fibrescopy when the patient underwent transbronchial lung cryobiopsy (TBLC) (B), the macroscopic view of resected lung specimen by TBLC (C) and haematoxylin and eosin staining of lung parenchyma in low magnification (×40, D) and high magnification (×100, E)
DISCUSSIONTo our knowledge, this is the first case of idiopathic DPO diagnosed by TBLC.
Cases of DPO are incidentally diagnosed at autopsy because idiopathic DPO has a very slow disease progression. However, the clinical course of DPO is unpredictable. Some patients with idiopathic DPO may develop intractable pneumothorax1, 2 or require lung transplantation due to the progression of ossification with respiratory failure.3 Therefore, it is important to diagnose DPO pathologically, as well as follow-up patients if a diagnosis of DPO is suspected.
Most DPO patients who are diagnosed while living undergo SLB, and only two reported cases were diagnosed using TBLB.4, 5 Four cases were diagnosed by SLB because these patients could not be definitively diagnosed by TBLB.2, 6-8 Thus, the diagnostic accuracy of TBLB for DPO, as well as in other interstitial lung diseases, may be controversial.
Dendriform ossification can be idiopathic or secondary, with the idiopathic type being more frequent. Secondary DPO is associated with primary lung diseases, such as interstitial lung diseases and emphysema. In contrast, the nodular type of diffuse pulmonary ossification is associated with passive congestion secondary to chronic heart failure, mitral stenosis and hypertrophic subaortic stenosis.4, 9 In our case, the patient had not been diagnosed with any prior diseases, and the chest HRCT and pathological findings were consistent with those of DPO. Idiopathic DPO was, therefore, diagnosed.
In the 1960s, cryoprobes were mainly utilized for therapeutic purposes. However, recently, cryoprobes are also being used in endobronchial procedures for diagnostic yield. TBLC is now being used for the diagnosis of lung diseases as it provides larger resected specimens of higher quality than those obtained by TBLB. Therefore, it has a high diagnostic yield for interstitial lung disease.10-12
TBLC is less invasive than SLB and can collect larger and higher-quality specimens than TBLB, despite the risk of complications, such as pneumothorax and haemoptysis. TBLC can be a good diagnostic procedure for DPO, as well as for other interstitial lung diseases.
ACKNOWLEDGMENTWe would like to thank Editage for English language editing.
AUTHOR CONTRIBUTIONYasuhito Sekimoto, Yuichi Nagata, Yuta Arai, Motoyasu Kato, Haruhi Takagi, Takehiko Shukuya, Tetsutaro Nagaoka and Kazuhisa Takahashi were the attending doctors who treated the patient on admission. Motoyasu Kato, Yuichi Fujimoto and Yasuko Yoshioka were outpatient doctors. Takuo Hayashi diagnosed the patient pathologically. Yasuhito Sekimoto and Motoyasu Kato drafted the manuscript. Yasuhito Sekimoto submitted the final manuscript. All authors read and approved the final manuscript.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this case report and accompanying images.
留言 (0)