
記住我

Antineutrophil cytoplasmic autoantibody (ANCA)-associated vasculitis (AAV) causes inflammation within the walls of small vessels in multiple organs due to the production of autoantibodies against the antigens myeloperoxidase (MPO) and proteinase 3 (PR3). When MPO and PR3 antigens are stimulated, they are released to the surface of neutrophils and adhere to the vessel wall, which can cause direct damage.1 Activated neutrophils also release chemicals that activate the complement pathway, resulting in more neutrophilic chemoattraction.
Studies have proposed that an inflammatory process, such as an infection or drug reaction, may stimulate ANCA to cause either direct endothelial toxicity or indirectly recruit another autoimmune reaction through a hyperinflammatory state.2 Although the second mechanism is not well understood, several conditions can lead to a hyperinflammatory state, including predisposing genetics, exposures (silica), drugs (hydralazine, minocycline, propylthiouracil, allopurinol, rifampicin), malignancy and autoimmune conditions. Additionally, viral and bacterial infections and an inflammatory response after a vaccination have also been identified as risk factors.1
Only a few cases of AAV after coronavirus disease 2019 (COVID-19) have been reported, including two for patients with associated MPO-ANCA glomerulonephritis, two for patients with MPO-ANCA diffuse alveolar haemorrhage who died and two for patients who had PR3-ANCA lung disease.3-6 One case of PR3-ANCA glomerulonephritis was reported after vaccination. Here, we present two cases of AAV potentially triggered by COVID-19: one triggered by COVID-19 infection and the other after COVID-19 vaccination, which we believe is the first temporal relationship of vaccine to the possible development of PR3-ANCA disease.
CASE REPORT Case 1An 86-year-old woman with known bronchiectasis (attributable to immunoglobulin G [IgG] deficiency), seronegative inflammatory oligoarthritis and polymyalgia rheumatica presented with increasing shortness of breath, fever, hypotension and an elevated d-dimer level. Polymerase chain reaction testing confirmed COVID-19, and radiography supported COVID-19 pneumonia findings without evidence of pulmonary embolism. Her oxygen requirements escalated, requiring her transfer to the intensive care unit. She had non-massive haemoptysis (<100 ml/24 h) and severe hypoxia, requiring 100% fraction of inspired oxygen from a high-flow nasal cannula. Two days after admission, a repeat chest radiograph showed new alveolar infiltrates in the right upper lobe and lingula, which were concerning for alveolar haemorrhage. The laboratory findings also confirmed a small amount of haemoglobin in the urinalysis, although her renal function remained normal throughout her hospitalization. Given her tenuous oxygenation on 100% high-flow oxygen and a do-not-intubate status, a diagnostic bronchoscopy was deemed unsafe. An autoimmune evaluation was positive for perinuclear-ANCA and MPO antibodies (6 U; reference range, <1). All other autoimmune findings were negative.
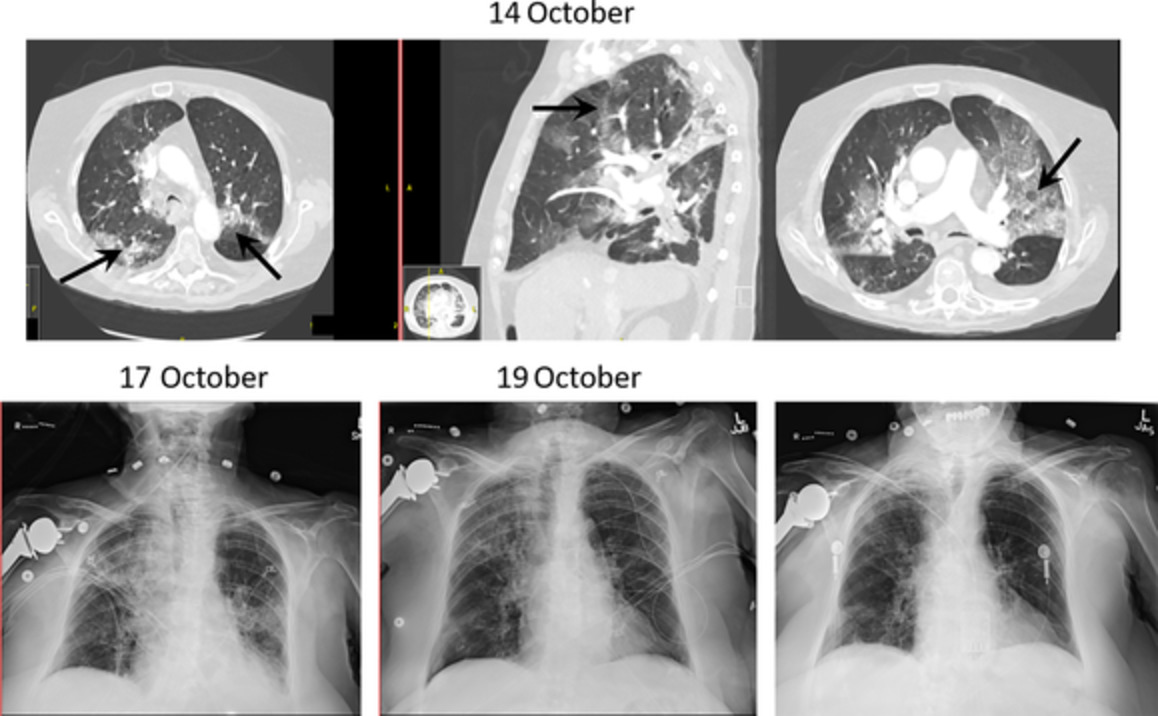
Because of the patient's history of inflammatory gouty arthritis, she underwent an extensive rheumatologic evaluation in 2017, and tests then were negative for MPO and ANCA. Therefore, we believed her condition to be a true serologic conversion induced by COVID-19 infection. She was given methylprednisolone (125 mg IV every 8 h). Over the course of the next few days, her oxygenation slowly improved, and haemoptysis resolved with corresponding radiographic improvement (Figure 1).

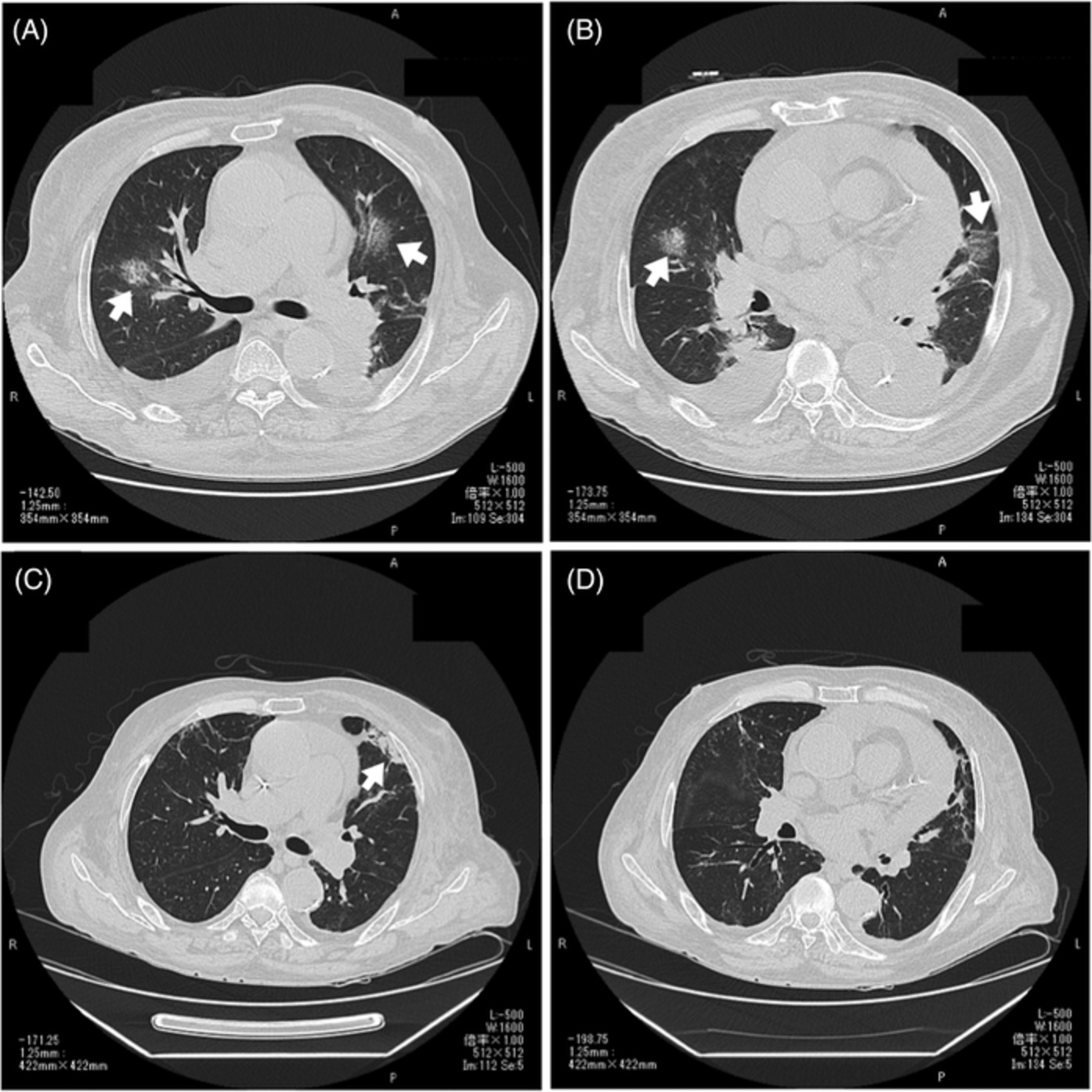
Progression of lung injury from the time of patient admission, with possible early findings of diffuse alveolar haemorrhage (DAH) on computed tomography (14 October 2020) to development of DAH shown on chest radiograph (17 October) (arrows). After the patient received methylprednisolone, radiography showed improvement (19 October and 25 October) (arrow)
The patient was not given immunosuppressive therapy other than glucocorticoids because of her acute, severe COVID-19 infection and the underlying IgG deficiency. She was, however, given two doses of convalescent plasma to help mount an appropriate antibody response to COVID-19. Methylprednisolone was tapered after her oxygen level improved, and she was given rituximab infusions. When her antibody tests were consistently positive 5 months later, methotrexate was attempted to avoid corticosteroids, but the patient could not tolerate it. At 6 months, her clinical condition was markedly improved, and she required only 1 L/min of oxygen.
Case 2A 60-year-old previously healthy woman presented to our outpatient pulmonary clinic with concerns of fatigue, 10-pound weight loss and loss of appetite for 1 month. Her symptoms began 1 day after she received her first COVID-19 vaccination (Moderna). One week after she received the second dose of the vaccine, she developed shortness of breath and flu-like symptoms. Her new symptoms were associated with tingling in the right ulnar and left sural nerve distribution. No nerve conduction study was performed. The numbness affected her daily function and required oral analgesics. Doppler venous ultrasonography of both lower extremities did not reveal deep venous thrombosis. She had transient vertigo with intermittent left-ear fullness for 1 week (third week of symptoms), which resolved spontaneously. She did not report skin rash, haematuria, sinus symptoms, ocular irritation, loss of vision, arthralgias or joint swelling.
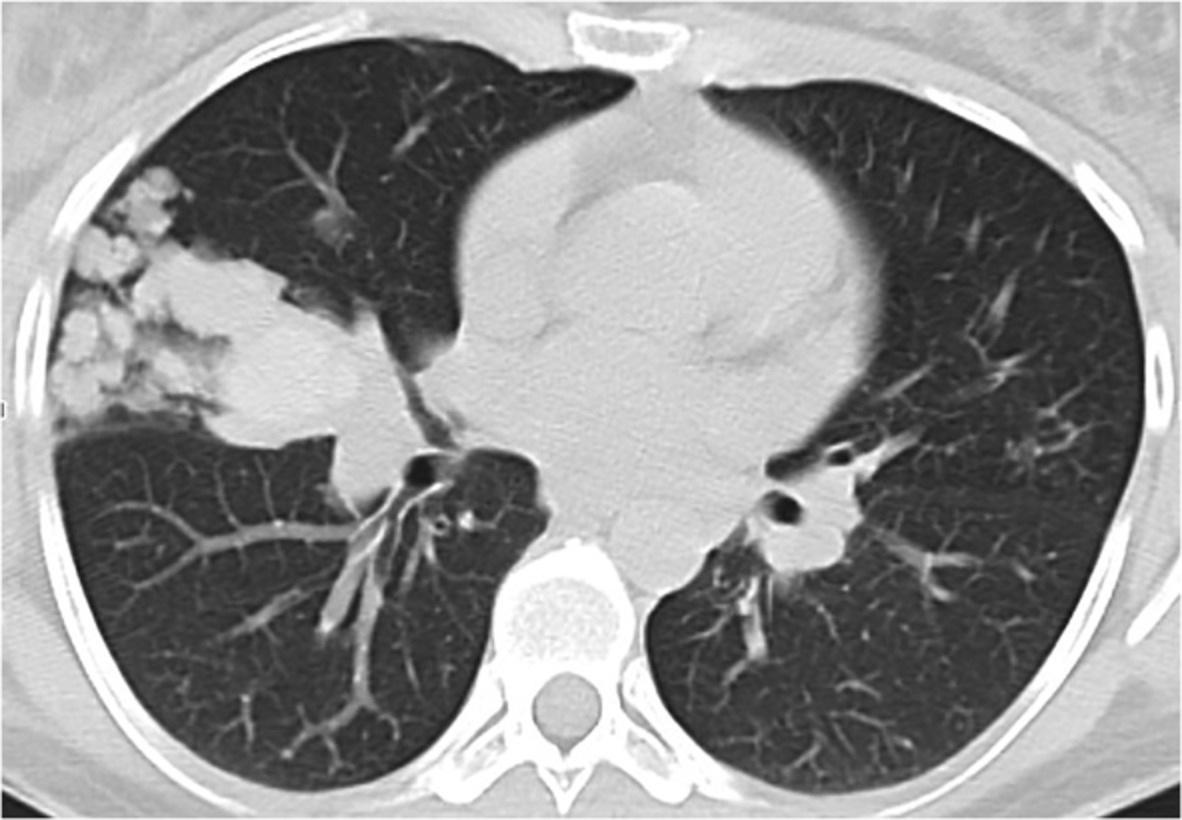
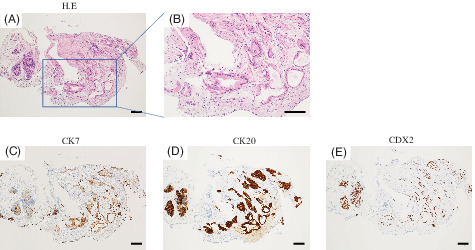
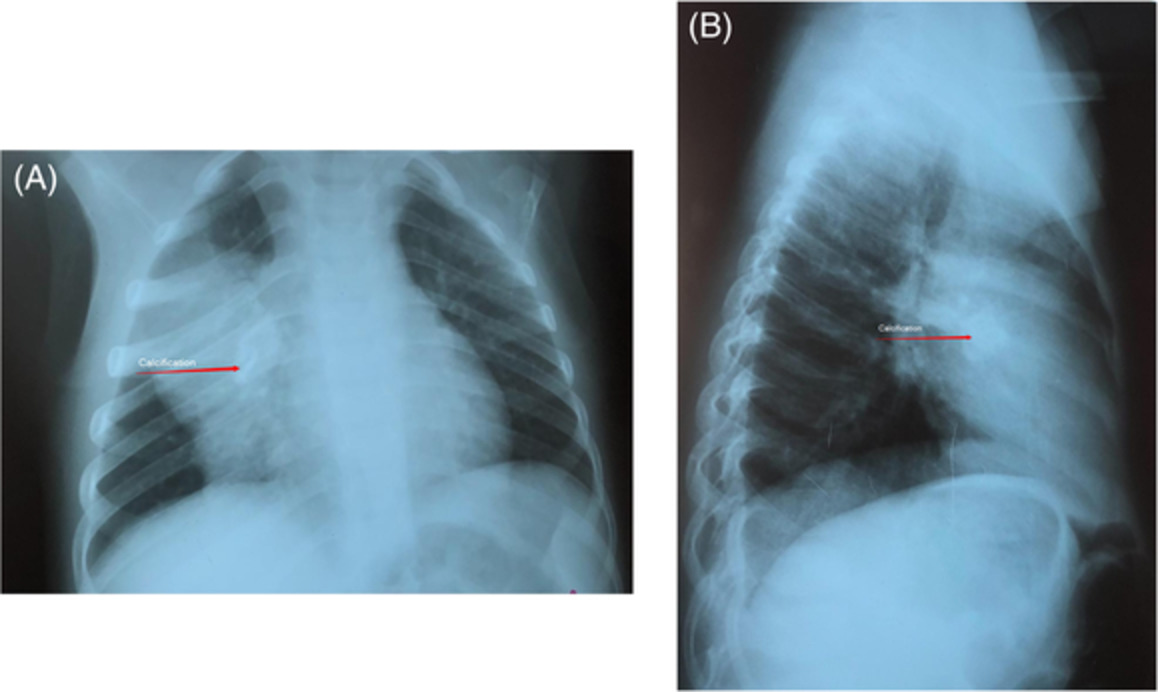
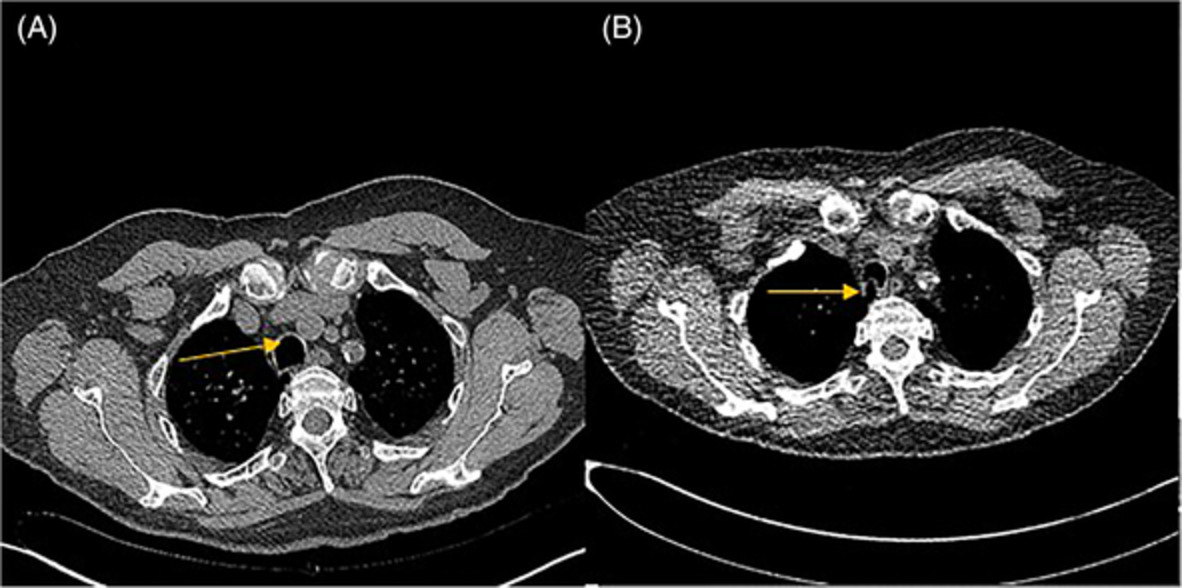
During the evaluation for weight loss, a chest radiograph was obtained, which showed bilateral consolidated mass-like lesions (Figure 2). The largest lesion measured 7 cm in diameter and was located in the right lower lobe. To rule out malignancy, a computed tomography-guided needle biopsy was done of the right lower lobe lesion, which showed acute necrotizing granulomatous inflammation. Histologic stains for fungi and mycobacteria were negative, and no organism was cultured. ANCA serologic testing was strongly positive (1:640 with PR3 at 979 AU/ml; reference, <19). A urinalysis showed haematuria with a count of 10 red blood cells/high-power field. The patient was diagnosed with granulomatosis with polyangiitis. She was given prednisone (60 mg orally daily), which was tapered over 12 weeks, and she was subsequently given rituximab. Her clinical condition improved, and repeat radiographs also showed near resolution of mass-like lesions. At follow-up, she had regained the weight that was initially lost and had improved energy, but she still had some tingling in the same nerve distributions.

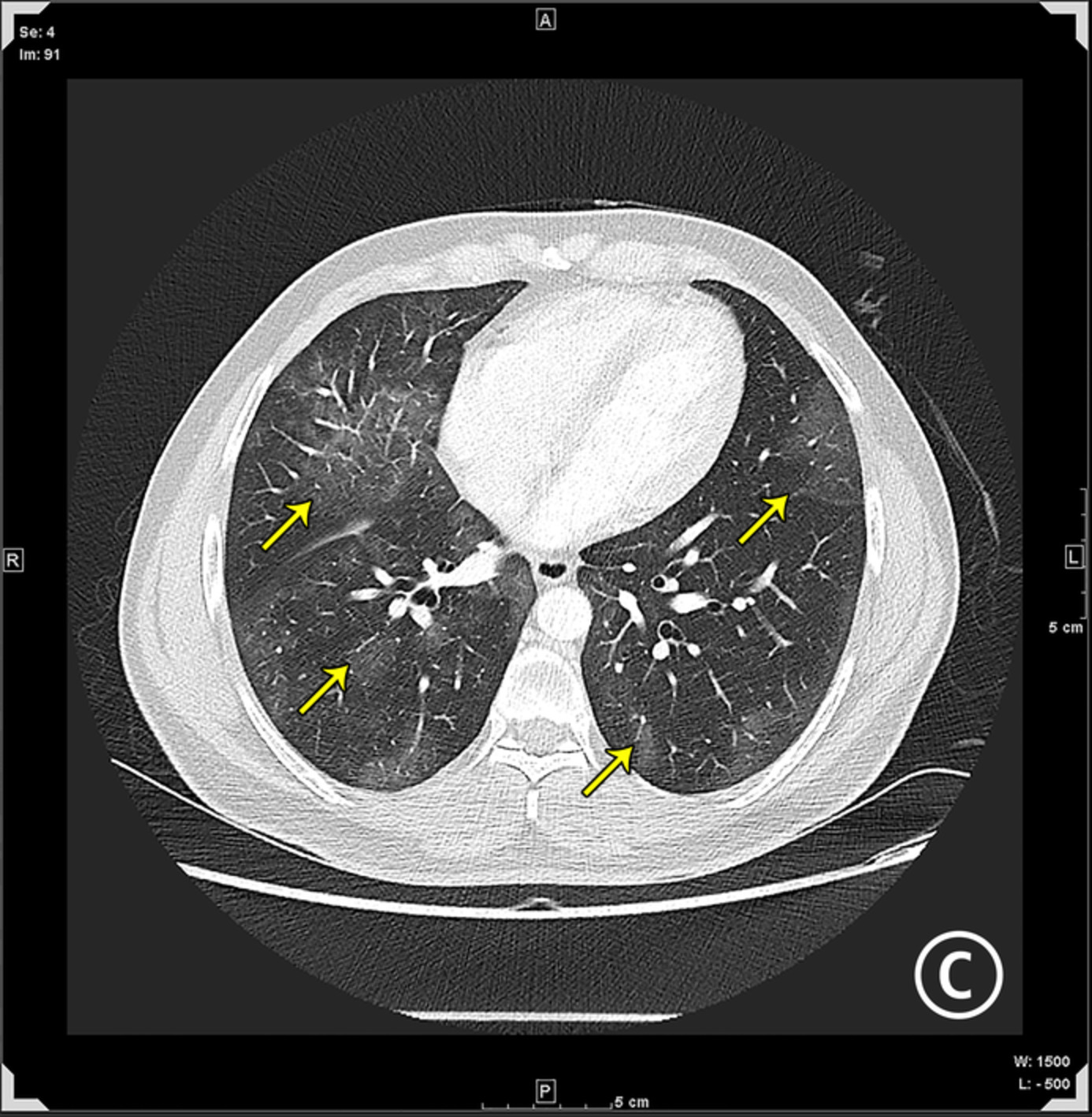
Initial computed tomographic images for the patient in case 2, showing nodular opacities. (A) The right lower lobe lesion, the largest, was the target for the needle biopsy (arrow). (B) Additional smaller opacities are shown in the left upper lobe (arrows)
DISCUSSIONWe presented two cases of potential COVID-19-associated AAV, one occurring in a patient with active infection and the other occurring shortly after vaccination. In both cases, early diagnosis of AAV allowed for appropriate administration of immunosuppressive therapies, with patient recovery.
The cause of AAV can be difficult to determine and can include a reaction to a drug or various infections and vaccination, both presumed to be mediated by similar mechanisms, likely sequalae of the resultant proinflammatory state.1, 7 Many AAV-associated conditions have been published in case reports,8 which speculate on possible causes including that any drug could cause vasculitis in persons with a susceptible genotype or that patients could already have been ANCA-positive, with the culprit medication simply making the disease more pronounced. More commonly, any infection (influenza and other viral, bacterial or fungal infections) can induce ANCA, which may disappear after the infection resolves, and importantly, vasculitis does not necessarily result from positive ANCA.2 Associations of vasculitis have also been reported for influenza, hepatitis A and B, rubella, smallpox, tetanus, tuberculosis and human papillomavirus vaccines; however, the evidence is from case reports.8 A randomized controlled trial of patients with and without vasculitis who received the influenza vaccine did not report any change in titre levels, disease activity or development of new ANCA antibodies after patients were vaccinated.9, 10 The incidence of reported AAV is still quite low after vaccination, even with the large number of vaccinations given for various diseases.8 The risk of AAV may be increased with COVID-19 infection; however, the risk after vaccination is rare and is even less common than that associated with other immunizations.
We do not know what caused AAV in our two cases, that is, whether it resulted from direct antigen-mediated endotheliitis from COVID-19 or it was de novo ANCA; however, our patients had high levels of inflammatory markers, suggesting that a hyperinflammatory state may have led to ANCA stimulation, which we speculate is due to COVID-19 exposure. The patient's symptoms in case 2 started just 1 day after vaccination, and it is unclear whether another trigger occurred before the first dose of the vaccine, causing a second immune reaction. These cases highlight that early identification of AAV in patients can lead to improved outcomes. Our patient with COVID-19 had negative serologic test results for ANCA 3 years before her COVID-19 diagnosis. However, she had been given prednisone a few months before because her symptoms from polymyalgia had worsened, which may have been the start of her ANCA disease. The patient who had possible vaccine-related ANCA had never previously undergone autoimmune evaluation.
Autopsies of patients with COVID-19 have shown alveolar haemorrhage, but limited reports have described vasculitis histologically in patients who survived.11 In contrast, mononeuritis multiplex is a known component of ANCA vasculitis, which could affect cranial nerves such as the optic nerve. A few cases of optic neuritis have occurred after COVID-19 infection.11
The decision regarding whether to give immunosuppressive therapy to a patient with active infection is always difficult. Given that rituximab, a monoclonal antibody to CD20, depletes B cells, we thought it was safest to administer once our patients no longer had active infections and had mounted an appropriate antibody response. A case–control study from Italy did not show worse outcomes for patients with rheumatologic diseases taking immunosuppressants who developed COVID-1912; however, a study from Spain showed more severe disease for patients with pre-existing lung disease or hypertension who were given glucocorticoids.13 Furthermore, recently published studies showed that patients who were undergoing rituximab infusions and subsequently developed COVID-19 infections did not have worse outcomes.12, 13
Although rare, AAV could possibly be associated with COVID-19 antigenic exposure after infection or immunization. Although AAV after infection or vaccination is not unique to COVID-19, diagnosing it early is vital for giving patients the benefit of immunosuppressive therapy. Although the COVID-19 antigenic association with AAV is described, to date no causative mechanism can be identified.
ACKNOWLEDGMENTSMarianne Mallia, ELS, MWC, Senior Scientific/Medical Editor, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
AUTHOR CONTRIBUTIONJamie R. Felzer cared for patient 1 and wrote most of the paper. Delvise T. Fogwe assisted with manuscript writing. Shaher Samrah cared for patient 2 and wrote the case presentation. Clement J. Michet cared for patient 1 and revised the manuscript. Ulrich Specks and Misbah Baqir advised on care of the patients and writing of the paper. Aahd F. Kubbara supervised care for both patients and oversaw writing of the entire manuscript.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
留言 (0)