
記住我

Adult T-cell lymphoma/leukaemia (ATLL) is a rare lymphoproliferative neoplasm of mature CD4+ CD25+ T cells caused by infection with the retrovirus human T-lymphotropic virus type 1 (HTLV-1).1 The subtypes of ATLL were classified according to the Shimoyama criteria: acute, lymphoma-type, chronic and smouldering, which differ in their presentation and prognosis.2 The onset of Pneumocystis jirovecii pneumonia (PJP) may be the first sign of ATLL. A case of transbronchial lung cryobiopsy (TBLC) performed on a lung lesion in a patient with ATLL diagnosed with PJP is presented. This is an important report that shows the usefulness of TBLC in differentiating pulmonary lesions in ATLL.
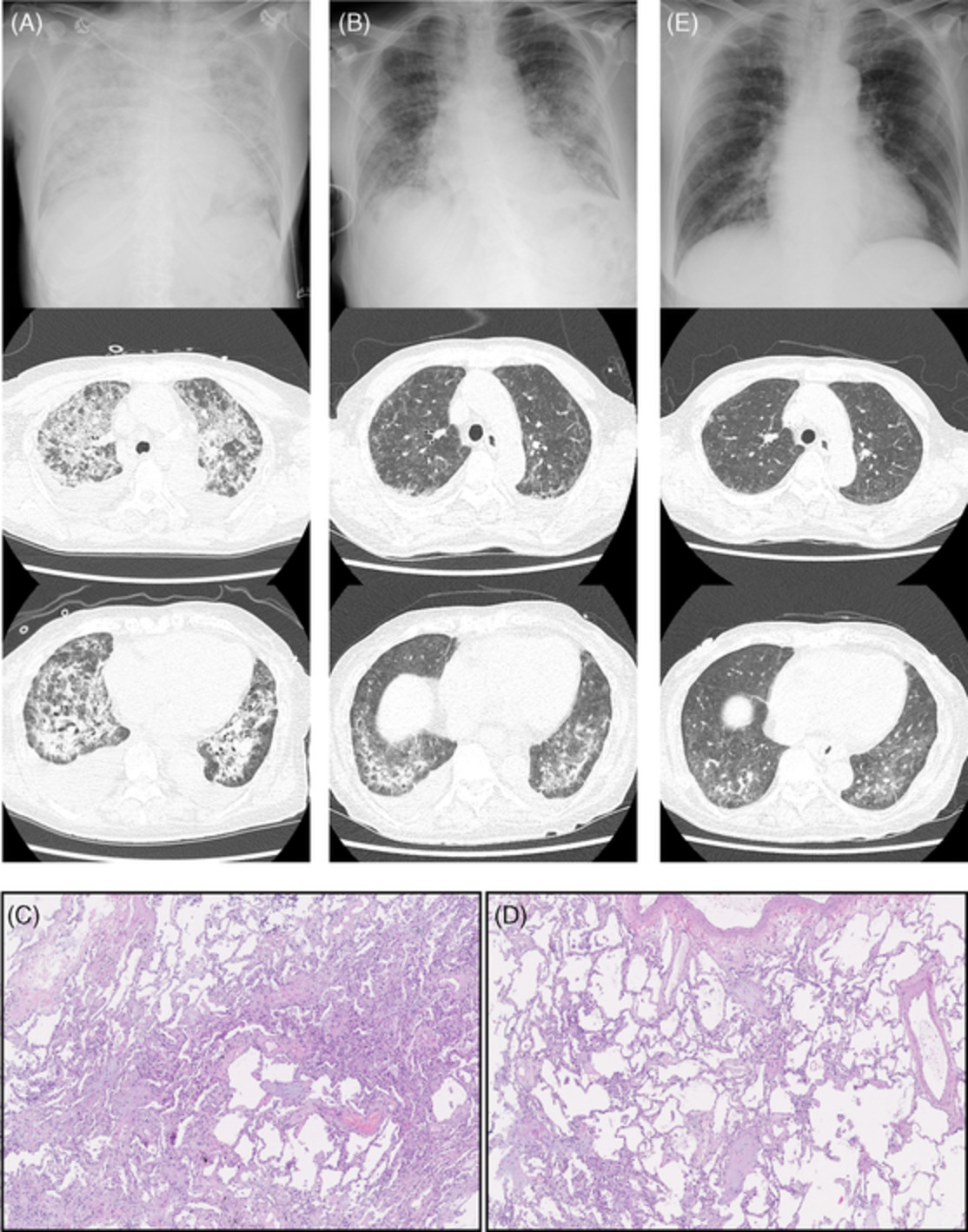
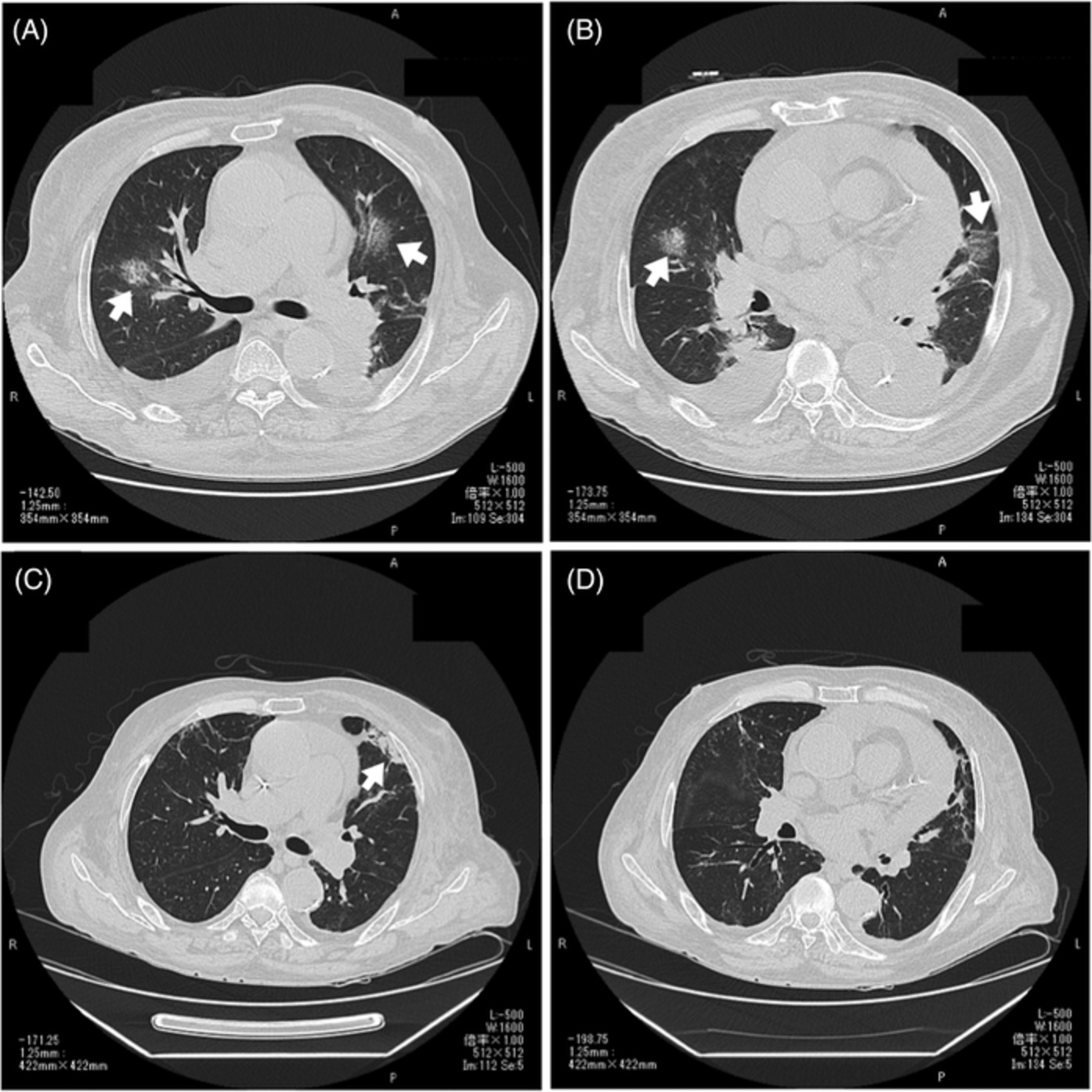
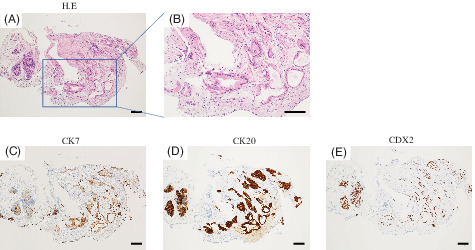
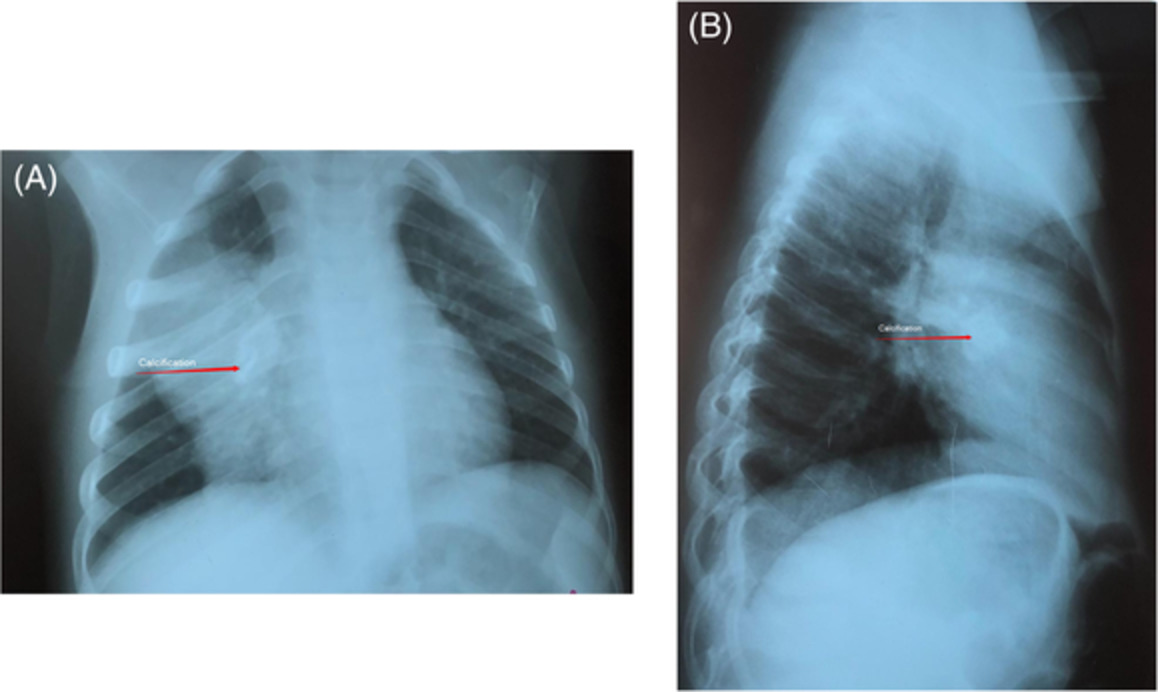
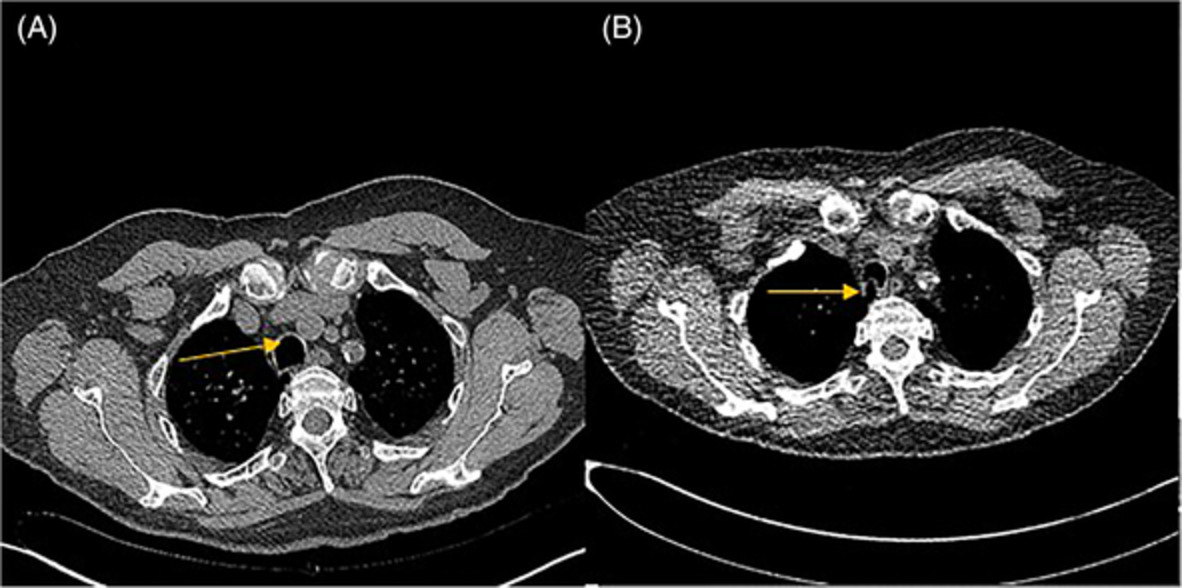
CASE REPORTA 79-year-old woman presented to the emergency department with a 1-week history of progressively worsening exertional dyspnoea. She denied other extrapulmonary symptoms or occupational or domestic exposures. She was a former smoker with a history of 10 pack-years and occasional drinking. She had hypertension and dyslipidaemia. She had been taking anti-cholesterolaemic and antihypertensive drugs orally for a long time, and she took no herbal medicines or supplements. She had no history of heart failure, cancer, asthma, allergic rhinitis or other connective tissue disease. There was no family history of lung disease, cardiac disease or malignancy. In the emergency room, the patient was sick, with a blood pressure of 104/70 mmHg, temperature of 38.0°C, pulse of 96 beats/min, respiratory rate of 30 breaths/min and oxygen saturation of 97% with a non-reservoir mask at 10 L O2/min. On examination, there were coarse crackles over the lungs and systolic murmurs over the heart. No swollen lymph nodes, dilated jugular veins or lower extremity oedema was observed. The electrocardiogram showed normal sinus rhythm. Transthoracic echocardiography showed nearly normal left ventricular wall motion, a left ventricular ejection fraction of 60% and trivial mitral/tricuspid/aortic regurgitation. The chest x-ray showed bilateral diffuse infiltrative shadows (Figure 1A). Chest high-resolution computed tomography (CT) showed bilateral diffuse infiltrative shadows and pleural effusions with no obvious lymph node enlargement, organomegaly or ascites (Figure 1A). On the admission day, bronchoscopy was performed under intubation in the intensive care unit. In the bronchoalveolar lavage fluid, a small number of atypical lymphocytes were detected, and polymerase chain reaction for PJP was positive. Pleural fluid examination showed atypical lymphocytes. Sulfamethoxazole-trimethoprim and corticosteroids improved the lung shadows and pleural effusions. However, consolidation remained on the dorsal side of bilateral lower lobes, and ATLL cell infiltration was suspected. On day 17, tissues from the residual infiltrative shadows in bilateral lower lung fields were obtained by TBLC (Figure 1B). TBLC showed a non-specific interstitial pneumonia pattern with a focal organizing pneumonia pattern without ATLL cell infiltration in the lung (Figure 1C,D). It was diagnosed as organizing pneumonia secondary to PJP. The chest consolidation showed an improving trend on chest CT (Figure 1E), and the patient was discharged in stable condition without chemotherapy.

(A) On admission, chest x-ray shows bilateral infiltration, and chest computed tomography shows bilateral consolidations and pleural effusions. (B) Before transbronchial lung cryobiopsy, the dorsal side of the bilateral lower lobe infiltration remains. Bilateral pleural effusions also remain. (C) Fibrosis forms towards the alveolar septa and intraluminal space, showing an organizing pneumonia pattern. (D) Alveolar septa are mildly thickened, infiltrated with small lymphocytes, showing a non-specific interstitial pneumonia pattern. (E) Before discharge from hospital, pulmonary infiltration continues to improve, and bilateral pleural effusions also continue to improve
DISCUSSIONA case that underwent cryobiopsy for PJP secondary to ATLL was described. Pulmonary lesions in ATLL can be divided roughly into opportunistic infections and non-infectious diseases. ATLL is a highly immunocompromised state, with a high risk of opportunistic infections including PJP.3 The development of PJP in ATLL patients is not uncommon.
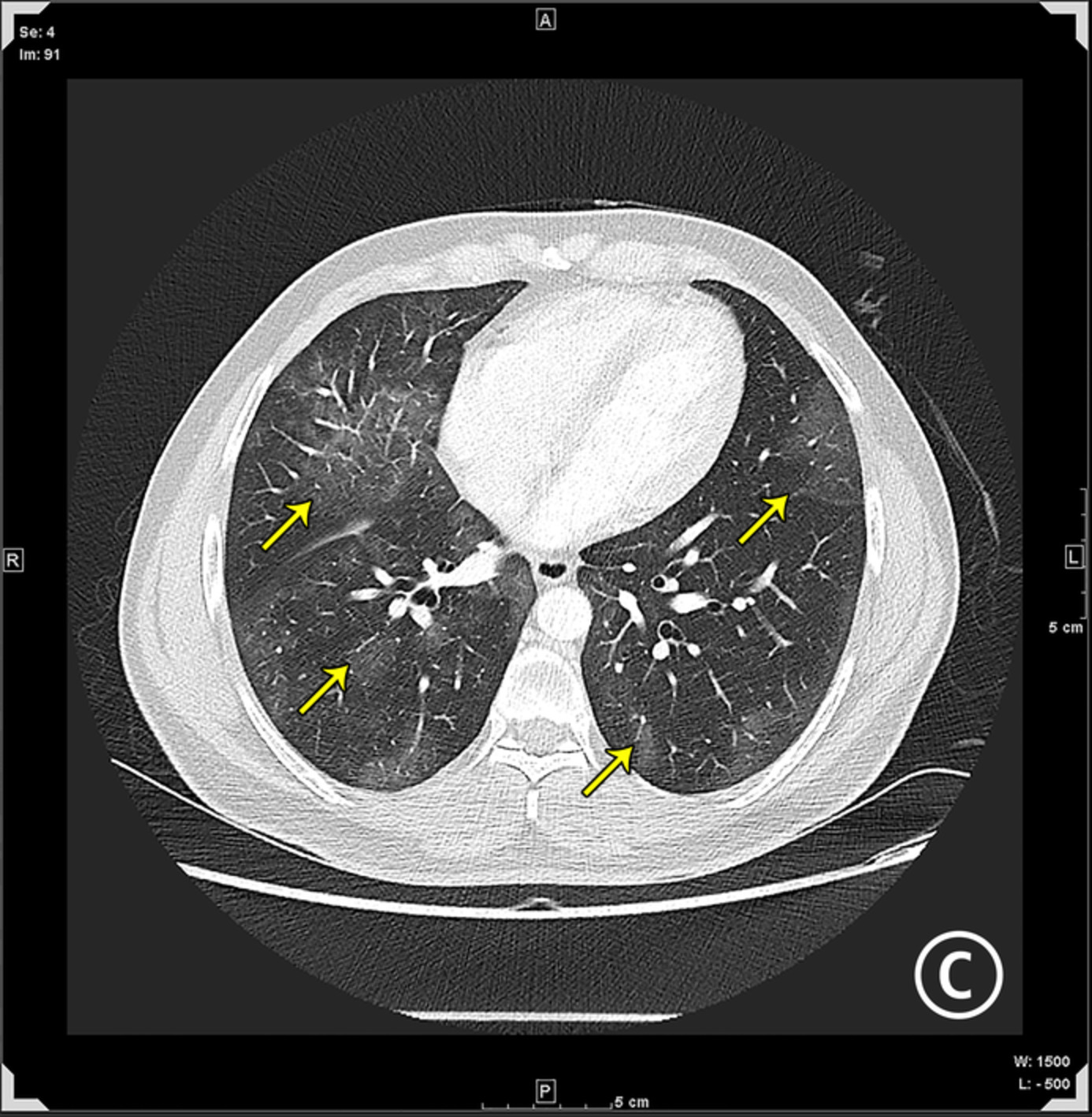
In terms of non-infectious pulmonary disease in ATLL patients, abnormal chest CT findings are diverse, including ground-glass opacities, bronchiectasis, centrilobular nodules and interlobular septal thickening.4 The incidence of abnormal findings was higher in aggressive ATLL than in indolent ATLL.5 In the present case, aggressive ATLL was suspected because of the extensive ground-glass opacities on chest CT and abnormal T lymphocytes and flower cells in peripheral blood. Some reports showed that HTLV-1-associated pulmonary diseases were caused by HTLV-1-infected lung epithelial cells,6 and another showed pulmonary infiltration of ATLL cells on lung biopsy.7 Various factors contribute to the lung disease, and lung biopsy plays an important role.
TBLC makes it possible to make a histopathological assessment, even in patients who cannot undergo a surgical lung biopsy. Recently, it was reported that TBLC was also safe and effective for diagnosis in patients with suspected pulmonary involvement of lymphoproliferative disorders.8 In the present case, TBLC confirmed that HTLV-1-infected cells did not infiltrate the lung tissue. In addition, as the pulmonary infiltration shadows tended to improve with treatment for PJP, the pulmonary infiltration shadows were considered to be due to organizing pneumonia secondary to PJP. With the results of the histopathological pulmonary findings by TBLC, it was possible to make the decision not to give chemotherapy.
In conclusion, the pulmonary lesions of ATLL patients vary with findings of infectious and non-infectious diseases. For accurate diagnosis, TBLC was useful for the pulmonary lesions of ATLL.
ACKNOWLEDGMENTThe authors would like to thank Forte Science Communications for the English language editing of our manuscript.
CONFLICT OF INTERESTNone declared.
AUTHOR CONTRIBUTIONHiroshi Kobe: writing – original draft. Kenki Saito: writing – review and editing. Machiko Arita: supervision; writing – review and editing. Tadashi Ishida: visualization; writing – review and editing.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
1Mehta-Shah N, Ratner L, Horwitz SM. Adult T-cell leukemia/lymphoma. J Oncol Pract. 2017; 13(8): 487– 92. 2El Hajj H, Tsukasaki K, Cheminant M, Bazarbachi A, Watanabe T, Hermine O, et al. Novel treatments of adult T cell leukemia lymphoma. Front Microbiol. 2020; 11:1062. 3Shahnaz S, Reich D, Arévalo-Valencia D, Kucinska S, Tulczynska J, Fleischman J. HTLV-1-associated adult T cell leukemia lymphoma presenting as granulomatous Pneumocystis jirovecii pneumonia (PJP) and hypercalcemia. J Gen Intern Med. 2007; 22(3): 420– 3. 4Einsiedel L, Chiong F, Jersmann H, Taylor GP. Human T-cell leukaemia virus type 1 associated pulmonary disease: clinical and pathological features of an under-recognised complication of HTLV-1 infection. Retrovirology. 2021; 18(1): 1. 5Yogi S, Yamashiro T, Kamiya H, Kamiya A, Miyara T, Moromizato H, et al. Thoracic manifestations of adult T-cell leukemia/lymphoma on chest CT: difference between clinical subtypes. Diagn Interv Radiol. 2019; 25(1): 55– 61. 6Teruya H, Tomita M, Senba M, Ishikawa C, Tamayose M, Miyazato A, et al. Human T-cell leukemia virus type I infects human lung epithelial cells and induces gene expression of cytokines, chemokines and cell adhesion molecules. Retrovirology. 2008; 5: 86. 7Jankipersadsing V, Tauchi T, Ohyashiki K, Tanaka Y, Setoguchi Y, Mukai K, et al. Spontaneous regression of pulmonary infiltration of adult T-cell leukemia/lymphoma. Int J Hematol. 2007; 86(3): 207. 8Bianchi R, Dubini A, Asioli S, Ravaglia C, Tomassetti S, Puglisi S. Transbronchial cryobiopsy: an effective tool in the diagnosis of lymphoproliferative disorders of the lung. ERJ Open Res. 2020; 6(3):00260-2019.
留言 (0)