
記住我

Expiratory central airway collapse (ECAC) is a diagnostic challenge due to its unspecific symptoms, and its gold standard for diagnosis, dynamic bronchoscopy, is invasive. There is an increased need for accurate non-invasive diagnostic workup. We report a case with suspected ECAC, where initial workup with standard forced expiratory computed tomography (CT) could not detect expiratory collapse. Given the high index of suspicion for ECAC, the patient underwent dynamic bronchoscopy confirming the diagnosis. Subsequently, the implementation of a novel CT protocol, dynamic forced expiratory (cinematic), which comprises detailed, consecutive helical imaging of the central airway throughout the entire respiratory cycle could also confirm severe ECAC as proven by dynamic bronchoscopy.
CASE REPORTA 77-year-old man was presented, with a past medical history of coronary artery disease, type 2 diabetes mellitus, obstructive sleep apnoea, ex-smoker quit 40 years ago, complaining of shortness of breath on minimum exertion and wheezing. Symptoms kept worsening for 4 weeks; pulmonary function tests ruled out obstructive and restrictive disease. Cardiac complications were ruled out. End-expiratory chest CT scan ruled out worsening parenchyma and ECAC as the culprit. Despite these results, dynamic bronchoscopy evidenced a greater than 70% reduction in the upper, middle and lower trachea; 80% collapse of cricoid; 70% left mainstem bronchus; 90% right mainstem bronchus; and 100% in bronchus intermedius, confirming expiratory dynamic airway collapse (EDAC). The patient did not wish to pursue surgical evaluation, presenting deterioration of his condition, requiring re-evaluation a year after. We performed a newly implemented CT protocol for ECAC, with good diagnostic correlation at dynamic bronchoscopy for stent trial (Figures 1-7).

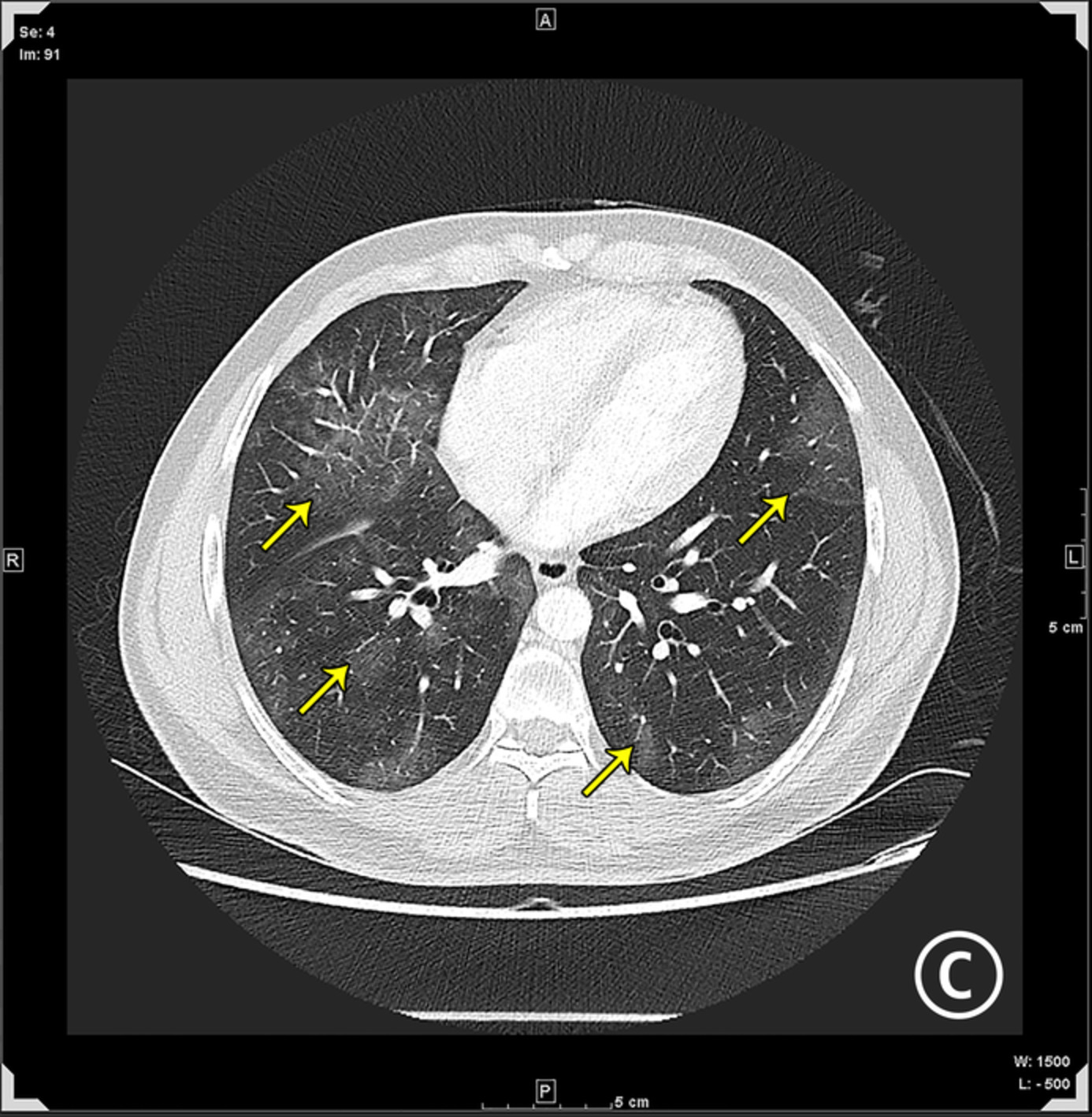
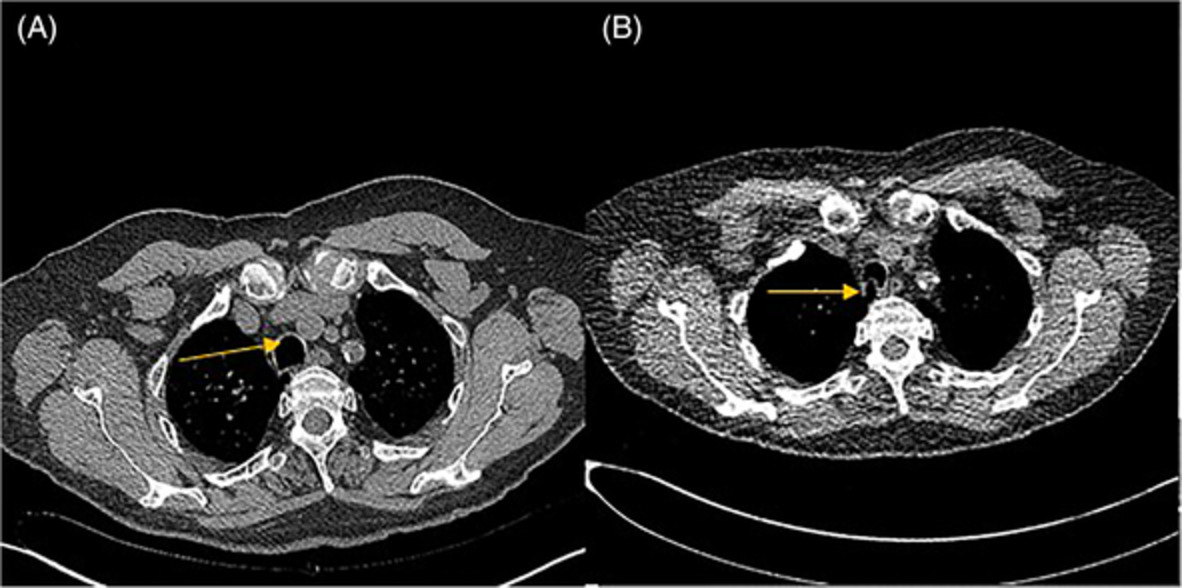
(A) Computed tomography (CT) image, with yellow arrow displaying mid-trachea during inspiration. (B) CT image, with yellow arrow indicating mid-trachea during forced expiration

(A) Computed tomography (CT) image, with yellow arrow indicating lower trachea during inspiration. (B) CT image, with yellow arrow showing lower trachea during forced expiration

(A) Computed tomography (CT) image, with yellow and blue arrows indicating the right and left mainstem bronchi, respectively, during inspiration. (B) CT image, with yellow and blue arrows displaying the right and left mainstem bronchi, respectively, during forced expiration

(A) Dynamic bronchoscopy showing collapse in the left mainstem bronchus. (B) Dynamic bronchoscopy showing the collapse in the right mainstem bronchus

(A) Static computed tomography (CT) image, with yellow arrow displaying mid-trachea during inspiration. (B) Static CT image, with yellow arrow indicating mid-trachea during expiration

(A) Static computed tomography (CT) image, with yellow arrow indicating lower trachea during inspiration. (B) Static CT image, with yellow arrow showing lower trachea during expiration

(A) Static computed tomography (CT) image, with yellow and blue arrows indicating the right and left mainstem bronchi, respectively, during inspiration. (B) Static CT image, with yellow and blue arrows displaying the right and left mainstem bronchi, respectively, during expiration
DISCUSSIONECAC includes EDAC and tracheobronchomalacia (TBM). Although both present with non-specific symptoms such as shortness of breath, cough and frequent respiratory infections, they have different pathophysiology. EDAC is a posterior membrane wall invagination into the tracheal lumen with a forward displacement during expiration due to weakness of the longitudinal muscle fibres. In contrast, TBM affects the anterolateral portion of the tracheobronchial tree, mainly a consequence of cartilage weakness.1 Various morphological types of ECAC have been described in the literature.2 A study by Litmanovich et al. recommended a threshold level of at least 70% of expiratory collapse on dynamic CT for considering ECAC to avoid false negatives encountered with the previous criteria of 50% airway collapse.3 Diagnosis requires a low threshold for suspicion as symptoms are often explained by other diagnostic entities and objective data.
Dynamic bronchoscopy is the current gold standard, involving a real-time assessment of the degree of collapsibility visually determined as mild (70%–79%), moderate (80%–89%) and severe (>90%).2 In some studies, expiratory CT is a diagnostic modality that reported high sensitivity for ECAC.4 Unfortunately, these are single-centre studies, and other centres have not replicated the same data, perhaps in part to overall resources invested in acquiring the images, respiratory coaching and spirometry guidance, making it hard to reproduce and generalize these findings in other centres.
The expiratory acquisition is timed to begin with the onset of the patient's forced expiration. The patient is instructed to take a deep breath and hold it (end-inspiratory scan), and then all the air is blown out (begin expiratory scan immediately). Initially, our patient underwent static forced expiratory in which images were obtained following the end-expiratory scan. This expiratory imaging did not elicit ECAC.
Subsequently, we performed our novel dynamic forced expiratory CT (cinematic), which involves sequential, helical acquisitions of the central airway over a 13.6-s period during a single forced expiration. The patient is instructed to take a deep breath-in (begin expiratory scan), forcefully blow out through his mouth (instruction given after the first shuttle was complete) and continue to blow out until the end of the scanning time. This diagnostic modality demonstrated ECAC as previously shown by dynamic bronchoscopy.
The cinematic view has evolved since the advent of multi-row CT detectors and is becoming the imaging method of choice for ECAC screening, giving a better sensitivity than static and end-expiratory protocols. Our protocol differs in that the degree of collapsibility is measured at the same anatomic level with dynamic bronchoscopy and expiratory chest CTs to have a common ground between radiology and pulmonology; this is compared to other imaging studies, in which the collapsibility index registered is obtained 1 cm above the aortic arch and 1 cm above the carina.4, 5
In a study conducted by Boiselle et al., the correlation coefficients for the static forced expiratory and end-expiratory modality were high using the previous definition of >50% airway collapse on CT.4 However, this was missed when applied to this case, potentially due to the lack of respiratory physiologist coaching and spirometry monitoring during the imaging capturing in this setting. The latter was not required with the cinematic modality, providing real-time imaging of the trachea and central bronchi during forced expiration of this patient. The technique requires minimal training of CT technologists on breathing instructions for the patients and scanning parameters.6
We believe that cinematic CT does not intend to replace the gold standard, but estimates the degree of severity and may benefit in the planning and execution of stent trial for patients detected with severe ECAC (>90% collapse) considering the invasive nature of the treatment in this category.
In conclusion, ECAC imaging remains controversial. The currently stablished techniques are challenging to reproduce in other centres, increasing the odds of false negatives. Our novel cinematic protocol is easier to reproduce and may potentially have a better correlation with the current gold standard, dynamic bronchoscopy. Cohort studies are needed to evaluate its standardized implementation.
ACKNOWLEDGMENTSWe are very grateful to the patient and his family.
AUTHOR CONTRIBUTIONSebastian Fernandez-Bussy, David Abia-Trujillo and Carlos Rojas were responsible for the diagnosis, treatment and care of the patient and obtained the images. Daniel Hernandez-Rojas wrote the original draft of the manuscript. Alejandra Yu Lee-Mateus, Rocio Castillo-Larios and Sai Priyanka Pulipaka supervised the manuscript. All authors edited and finalized the final version.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this case report and accompanying images.
留言 (0)