
記住我

Lung cancer, including non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC), is known globally as one of the leading causes of malignant tumor-associated death.1 It has previously been reported that most NSCLC (75%) cases are at an advanced stage when first diagnosed and the opportunity of surgery as a result of metastatic brain disease has been lost.2 The general prognosis for NSCLC patients with metastatic brain disease is poor with an extremely low long-term survival rate.3 At present, whole brain radiotherapy (WBRT) is generally used for controlling metastatic lesions of the brain in NSCLC patients, especially those patients with multiple brain lesions.4 However, the treatment response or prognosis of patients with metastatic brain disease is unsatisfactory with a median survival time of 3–6 months. Therefore, improving the treatment efficacy of NSCLC patients with brain metastasis is important in order to improve their overall survival.5
Tyrosine kinase inhibitors (TKIs) are small molecular targeted drugs that can inhibit tyrosine kinases. Tyrosine kinases are enzymes responsible for the activation of many proteins by signal transduction cascades. Epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs), such as erlotinib and gefinitib, are commonly clinically used in the treatment of patients with advanced NSCLC, especially those with EGFR/KRAS mutation. Several studies have previously evaluated the efficacy and safety of WBRT+EGFR-TKI versus WBRT only in brain metastasis cases of NSCLC.6, 7 However, the conclusion of these studies was different due to different treatment modality and patients clinical heterogeneity. Therefore, we performed this meta-analysis to further evaluate the efficacy and safety of WBRT+EGFR-TKI versus WBRT only in the treatment of brain metastasis of NSCLC with an up-to-date meta-analysis.
METHODS Identification of studies via electronic databasesProspective clinical studies on the efficacy and safety of WBRT+EGFR-TKI versus WBRT only in the treatment of NSCLC patients with brain metastasis were electronically searched in the Pubmed, EMbase, Cochrane, Wangfang, CNKI and Google scholar databases. The electronic database searching words were: Epidermal growth factor receptor-tyrosine kinase inhibitors/EGFR-TKI, lung cancer, carcinoma of the lung, non-small cell lung cancer, whole brain radiotherapy/WBRT, and gefitinib, erlotinib. The references of the identified studies were also reviewed to determine potentially suitable publications.
Study inclusion and exclusion criteriaInclusion criteria: (i) Prospective clinical studies relevant to WBRT+EGFR-TKI versus WBRT only in the treatment of NSCLC patients with brain metastasis. (ii) Patients included in original studies were those with NSCLC confirmed by pathology or cytology. (iii) Studies were published in English or Chinese. (iv) Brain metastasis was confirmed by CT or MRI. (v) Treatment associated response and toxicity could be extracted from the original studies.
Exclusion criteria: (i) Review or case report relevant to WBRT+EGFR-TKI or WBRT in the treatment of NSCLC patients with brain metastasis. (ii) Animal studies. (iii) Brain metastases of other carcinoma not NSCLC. (iv) Studies without enough data to calculate the ORR or treatment toxicity.
Data and information extractionTwo researchers independently reviewed the studies and extracted the data. If there were different opinions in data extraction, a third reviewer was consulted to discuss the divergence and make a final decision. The information extracted from the study included: (1) general data: author's name, publication date and author's country, and (2) literature features: number of cases, median age, EGFR mutation status, treatment methods and outcome indicators in the WBRT+EGFR-TIK and the WBRT only group. The corresponding authors would be contacted by e-mail if the required data could not be obtained. If the required data could not be obtained finally, it would be recorded as “not available/Na”.
Publication bias evaluationThe publication bias was evaluated by Begg's funnel plot and Egger's line regression test. If the funnel plot was left–right symmetrical and Egger' test p > 0.05, the publication bias was considered as not significant.
Statistical analysisSTATA11.0 statistical software (http://www.stata.com) was used for data pooling. The treatment response was demonstrated by objective response rate (ORR) and calculated by the equation of ORR = complete response (CR) + partial response (PR). The ORR and treatment associated toxicity was expressed by odds ratio (OR) and corresponding 95% confidence interval (95% CI). The statistical heterogeneity across the included 18 studies was investigated by I2 test. Publication bias was assessed by Begg's funnel plot and Egger's line regression test (Figure 1).

Flow-chart of electronic searching and inclusion procedure of studies included
RESULTS Main features of included studiesAfter removing unsuitable publications, 18 prospective clinical studies were included for clinical data combination. The general features of the studies included are shown in Table 1.
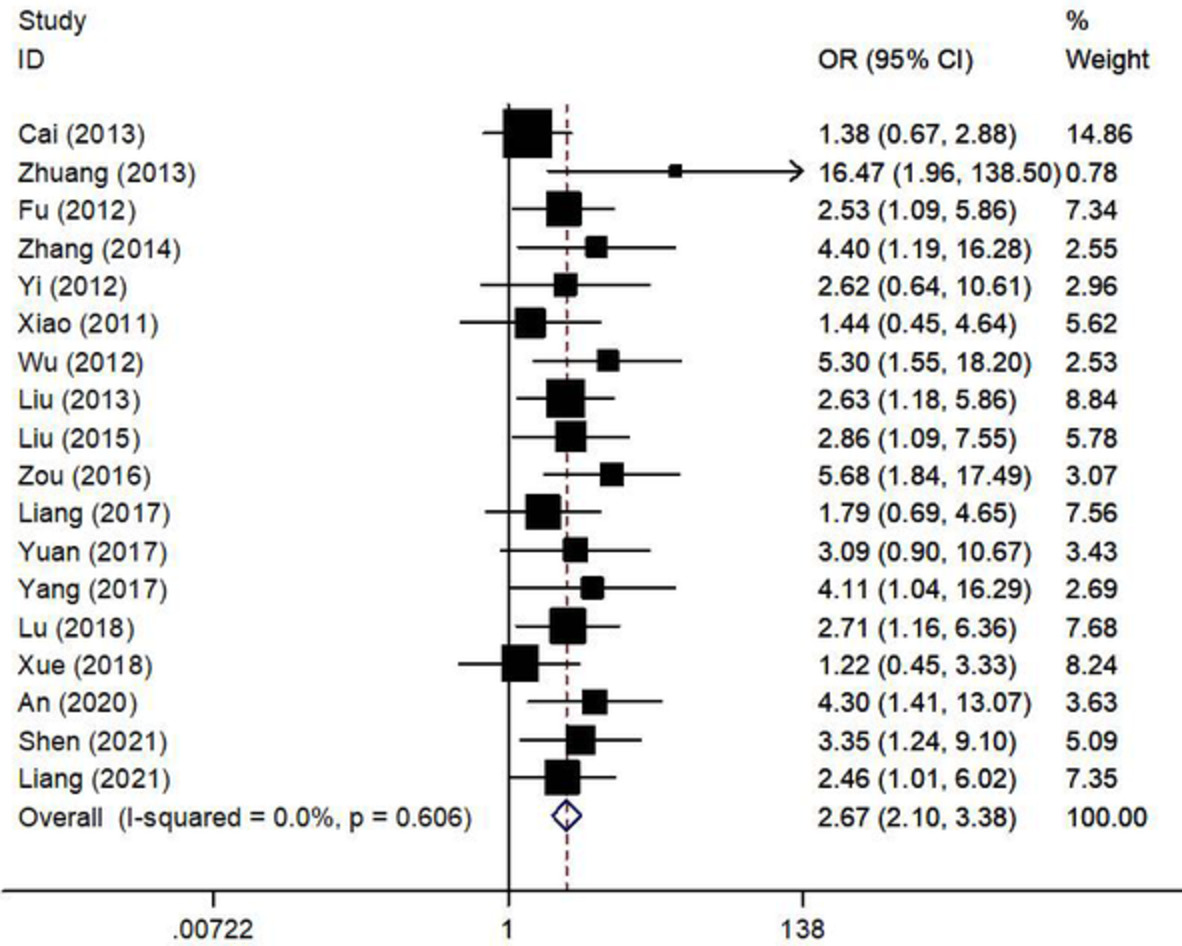
TABLE 1. Main features of the included studies of WBRT+EGFR-TKI versus WBRT only for non-small cell lung cancer patients with brain metastasis Studies Year WBRT+EGFR-TKI WBRT only Outcome EGFR mutation Sample size Age Treatment Sample size Age Treatment Cai et al.6 2013 65 Na WBRT + erlotinib/gefinitib 92 Na Whole brain radiotherapy ORR, 1-year survival, toxicity 27.4% Zhuang et al.7 2013 23 60 WBRT 31 63 WBRT ORR 20.4% Fu et al.8 2012 38 56 Radiotherapy + gefitinib 123 56 Radiotherapy ORR, 1-year survival, toxicity Na Zhang9 2014 20 52 (32–78) Radiotherapy + gefitinib/ erlotinib 27 51 (33–75) Radiotherapy ORR, 1-year survival, toxicity Na Yi & Qin10 2012 21 Na Radiotherapy + gefitinib 21 Na Radiotherapy ORR, DCR, toxicity Na Xiao et al.11 2011 24 Na 3D-CRT + gefitinib 22 Na 3D-CRT ORR, DCR, toxicity Na Wu et al.12 2012 35 Na WBRT + gefitinib 18 Na WBRT ORR,1-year survival rate Positive Liu13 2013 52 54 (28–74) WBRT/3D-CRT + erlotinib 52 51(30–72) WBRT/3D-CRT ORR, DCR, toxicity, PFS Positive Liu et al.14 2015 35 75.8 (65–80) Radiotherapy + gefitinib 35 74.8 (65–80) Radiotherapy ORR, DCR, toxicity Nm Zou et al.15 2016 30 64.12 (20–70) WBRT + gefitinib 30 64.32 (22–7-) WBRT ORR, DCR, KPS, 1-year survival, toxicity Positive Liang et al.16 2017 35 52.5 (45–60) WBRT + erlotinib 35 61.5 (55–68) WBRT ORR, DCR, toxicity Positive Yuan et al.17 2017 23 58.4 (45–73) WBRT + erlotinib 23 58.5 (44–72) WBRT ORR, DCR, 1-year survival, toxicity Na Yang18 2017 40 59.4 (43–75) WBRT + erlotinib 40 59.8 (45–73) WBRT ORR, DCR, 1-year survival Mixed Lu19 2018 45 67.45 (52–83) WBRT/3D-CRT + erlotinib 45 68.06 (55–85) WBRT/3D-CRT ORR, DCR, 1-year survival Na Xu et al.20 2018 31 54.47 (36–69) WBRT + gefitinib 30 53.52 (35–70) WBRT ORR, DCR, toxicity Positive An et al.21 2020 30 39–78 WBRT + gefitinib 30 39–78 WBRT ORR, DCR, toxicity Na Shen22 2021 36 57.43 (35–67) WBRT + gefitinib 36 58.52 (37–64) WBRT ORR, DCR, toxicity Na Liang23 2021 41 68.2 (41–82) WBRT + erlotinib 41 68.9 (53–83) WBRT ORR, DCR, toxicity,1-year survival Na Combined objective response rate between WBRT+TKI and WBRT only groupsAll the 18 studies reported a response rate between the WBRT+TKI and WBRT only groups. The combined result indicated that ORR in the WBRT + TKI group was superior to WBRT only with a statistical difference (OR = 2.67, 95% CI: 2.10–3.38, p < 0.05) under a fixed effect model, Figure 2.

The forest plot of objective response rate between WBRT+TKI versus WBRT only for non-small cell lung cancer patients with brain metastasis
1-year survival analysis between WBRT+TKI and WBRT only groupsTen studies reported the 1-year survival rate between the WBRT+TKI and WBRT only groups. The data was combined under a fixed effect mode because of nonstatistical heterogeneity (I2 = 0.0%, p = 0.666). The combined results showed that the 1-year survival rate in the WBRT+TKI group was higher than that of the WBRT only group with a statistical difference (OR = 2.70, 95% CI: 1.95–3.74, p < 0.05), Figure 3.

The forest plot of the 1-year survival rate between WBRT+TKI versus WBRT only for non-small cell lung cancer patients with brain metastasis
Treatment-related toxicity between WBRT+TKI and WBRT only groupsThe combined results demonstrated that the treatment-related rash in the WBRT+TKI group was significantly higher than that of the WBRT only group with a statistical difference (OR = 2.72, 95% CI: 1. 53–4.84, p < 0.05). However, the incidence of nausea/vomiting (OR = 0.84, 95% CI: 0.60–1.17, p > 0.05), diarrhea (OR = 1.31, 95% CI: 0.83–2.07, p > 0.05), fatigue (OR = 1.40, 95% CI: 0.70–2.81, p > 0.05) and myelosuppression (OR = 0.86, 95% CI:0.56–1.32, p > 0.05) were not statistically different between the WBRT+TKI and WBRT only groups, Figure 4.

The forest plot of treatment-related toxicity between WBRT+TKI versus WBRT only for non-small cell lung cancer patients with brain metastasis
Publication biasThe funnel plot was left–right asymmetric which indicated an obvious publication bias. The Egger's line regression test also showed statistical publication bias (p < 0.05), Figure 5.

The funnel plot of treatment-related toxicity between WBRT+TKI versus WBRT only for non-small cell lung cancer patients with brain metastasis
DISCUSSIONBrain metastasis in NSCLC patients is common. About 30%–50% of patients with NSCLC will eventually develop brain metastasis leading to neurological dysfunction which seriously reduces their quality of life. The prognosis of NSCLC patients with brain metastatic lesions is extremely poor with a median survival time of 3–6 months. Therefore, how to determine effective treatment methods in lung cancer patients with brain metastasis is important in order to improve their prognosis. It has been reported that the prognosis of brain metastatic driver gene positive NSCLC cases can be significantly improved by gene detection and targeted drug treatment. Lung cancer driver genes usually include epidermal growth factor receptors (EGFRs), anaplastic lymphoma kinase (ALK), ROS1 fusion, HER2 mutation, BRAF mutation, neurotrophic tyrosine receptor kinase (NTRK) fusion, etc.
In recent years, with the rapid development of precision medicine, targeted drugs associated with the aforementioned driver genes play an important role in improving the prognosis of NSCLC patients with brain metastasis. The most applied targeted drugs for patients with advanced NSCLC include epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI), such as gefitinib and erlotinib. EGFR targeted drugs are small molecule drugs of erlotinib and gefitinib which can pass through the blood–brain barrier and can be used in the treatment of NSCLC patients with brain metastasis. For NSCLC patients with brain metastasis and EGFR mutation, the ORR has been reported to be about 60% with a median OS of 13 months, and median PFS of 11.7 months.24, 25
Several studies have indicated that WBRT plus target drugs may have potential survival benefit for improving the treatment response and long-term survival of NSCLC cases with brain metastasis.26 However, the conclusion of these studies was different due to the different treatment modalities and clinical heterogeneity of patients. In the present study, we pooled the treatment response and toxicity of the 18 studies included and found the ORR and 1-year survival rate in the WBRT+TKI group was higher than that of the WBRT only group with a statistical difference (p < 0.05). However, the treatment-associated toxicity of a rash in the WBRT+TKI group was significantly higher than that of the WBRT only group (OR = 2.72, 95% CI: 1.53–4.84, p < 0.05). This study indicates that based on current publications, WBRT+EGFR-TKI can improve the treatment response and 1-year survival rate but not increase the toxicity except for a rash, compared with WBRT alone in NSCLC patients with brain metastasis.
In conclusion, WBRT combined with EGFR-TKIs for NSCLC patients with brain metastasis is better than WBRT only. WBRT+EGFR-TKIs can improve the treatment response and 1-year survival rate, but does not increase the treatment toxicity, except for rash. However, there are also deficiencies in the meta-analysis such as the small samples in each study included, clinical heterogeneity (age of the included cases, treatment modality, gene mutations) language restriction and publication bias. Therefore, the conclusions should be further validated by well-designed multiple center clinical trials.
ACKNOWLEDGMENTThis work was supported by medical and health science and technology project of Zhejiang Province (no.2020ky1076).
CONFLICT OF INTERESTThe authors confirm that there are no conflicts of interest.
留言 (0)