
記住我

A 35-year-old primigravida woman presented with severe back pain at approximately 34 weeks' gestation. She had no underlying diseases but had suffered from nonspecific pelvic pain over the previous 2 years. At an outside hospital, the patient underwent full-body computed tomography (CT), where multiple pleural nodules were observed (Figure S1). She was referred to our hospital for further evaluation and delivery. Upon referral, she was at 35 weeks' gestation and had good physical status with independency in activities of daily living. The patient exhibited adequate maternal nutritional status, was 158 cm in height and 72.7 kg in weight. Her vital signs were stable at admission with blood pressure measuring 124/73, pulse rate 89, respiratory rate 18 and body temperature 36.7°C. She was a never-smoker. At 35 weeks' gestation, she underwent a planned cesarean section.
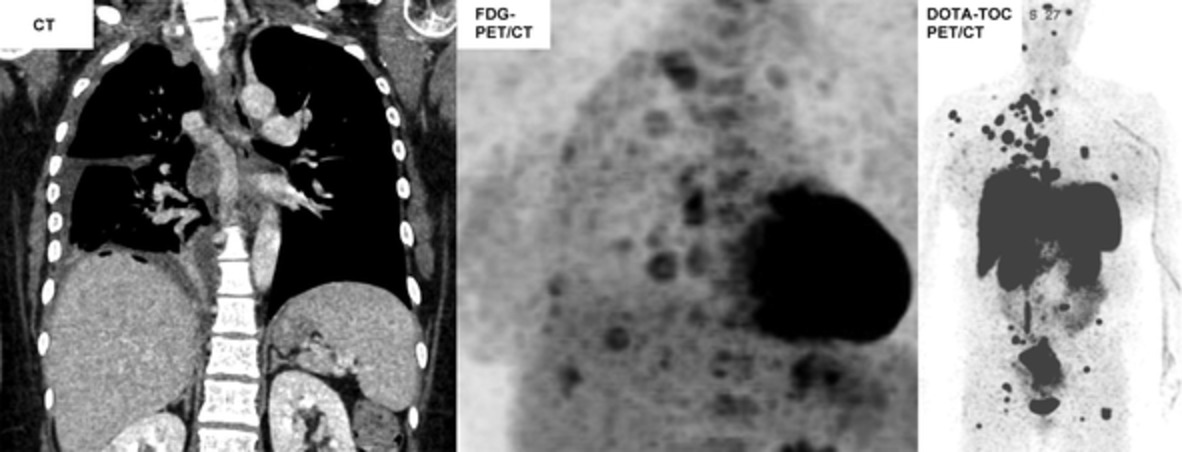
On contrast-enhanced chest CT and 18F-fluorodeoxyglucose (FDG) positron emission tomography-CT (PET/CT) performed after delivery (Figure 1), multiple pleural nodules demonstrated variable degrees of enhancement and metabolism, with some nodules showing internal low attenuation, suggesting necrotic changes. There was a 1.5-cm-sized, well-marginated, ovoid, parenchymal nodule in the left lower lobe with lobulating contours, demonstrating mild enhancement. In the upper inner quadrant of the breast, there was a 2.2-cm-sized, ill-defined lesion with strong enhancement. Compared with the CT examination 1 month prior, an interval increase in pleural effusion was noted, while there were no significant interval changes in the sizes of pleural nodules or lung parenchymal and breast lesions. FDG PET/CT showed variable but generally hot uptake for pleural nodules and breast lesions, while there was no significant uptake in lung parenchymal lesions. Imaging patterns of each of the metastatic lesions are described and presented in Table 1 and Figure 1.

Different imaging findings of atypical carcinoids in CT, FDG PET/CT, and DOTA-TOC PET/CT (rows) arranged by organ (column). (a) Solid (arrow) pleural nodule in right lung apex and necrotic (asterisk) pleural nodule on contrast-enhanced chest CT scan. (b) FDG PET/CT showing uptake in nodular pleural lesions and diffuse uptake for vertebral bodies. (c) DOTA-TOC PET/CT scan showing uptake for pleural lesions, vertebral bodies, and nodule in left lower lobe (blue arrow). (d) Solid pleural nodules of lung apex (asterisks) on contrast-enhanced chest CT scan. (e) Variable FDG PET/CT uptake of apical pleural nodules (arrows). (f) Strong uptake of apical pleural nodules on DOTA-TOC PET/CT scan. (g) Necrotic pleural nodule (arrow) on contrast-enhanced chest CT scan. (h) FDG PET/CT scan of necrotic nodule (arrow). (i) DOTA-TOC PET/CT scan of necrotic nodule (arrow). (j) Breast nodule (arrow) on contrast-enhanced chest CT scan. (k) FDG PET/CT scan of breast nodule (arrow). (l) DOTA-TOC PET/CT scan of breast nodule (arrow). (m) Parenchymal nodule with lobulating contour in left lower lobe (arrow). Note pleural effusion in right hemithorax (asterisk) on contrast-enhanced chest CT scan. (n) Low uptake for parenchymal lesion in FDG PET/CT (arrow). (o) High uptake of parenchymal lesion on DOTA-TOC PET/CT scan. (p) Contrast-enhanced chest CT scan showing no discernible thyroid lesion. (q) FDG PET/CT showing no significant uptake in thyroid. (r) Strong uptake noted in left thyroid on DOTA-TOC PET/CT scan (arrow). (s) Ill-defined osteolytic lesion noted in sacrum, bone window of abdominal CT. (t) High uptake of sacral lesion on FDG PET/CT. (u) High uptake of sacral lesion on DOTA-TOC PET/CT scan
TABLE 1. Radiological spectrum of atypical carcinoids Location CT features SUVmax on FDG PET/CT 68 Ga–DOTA-TOC PET/CT Solidity Margin Other characteristics Lung parenchymal lesion (LLL) Solid Well defined Low High Pleura Solid or necrotic Well defined Multiple solid nodules, some with necrosis Variable High Breast Solid Poorly defined High High Right axillary lymph node Solid Smooth Low High Left thyroid Solid Indiscernible Low High Bone Osteolytic - Mainly involving ribs, vertebral body, and sacrum High High Abbreviations: CT, computed tomography; ID, ill-defined; LLL, left lower lobe; PET/CT, positron emission tomography/computed tomography; SUV, standardized uptake value; WD, well-defined.Under clinical suspicion of malignant mesothelioma or metastasis of unknown primary site including lung and breast cancers, video-assisted thoracoscopic surgery (VATS) biopsy of the pleural lesions was performed. Frozen section examinations indicated malignant mesothelioma. Subsequent staining for mesothelioma, however, was negative for Calretinin, TTF-1, WT-1, and D2-40. Under suspicion of breast cancer, ultrasonography was performed and showed an irregular-shaped, low echoic mass in the upper inner quadrant of the right breast (Figure S2). The mass was graded as 4C based on breast imaging-reporting and data system (BI-RADS), indicating a high suspicion of malignancy. On subsequent breast biopsy, the histological findings of the breast lesion were identical to those of the pleural lesions (Figures S2 and S3). On immunohistochemistry, the markers related to the breast cancer such as ER, PR, HER2, BRST-2, and GATA3 were all negative. On a second analysis, hematoxylin and eosin staining revealed monotonous cells with organoid or glandular distribution. Tumor cells had round to oval nuclei, some with eosinophilic cytoplasm, suggestive of neuroendocrine carcinoma (Figure S3). Staining for neuroendocrine markers including cytokeratin, CD56, chromogranin, and synaptophysin showed positive results for both pleural and breast tissues, leading to diagnosis of atypical carcinoid tumor. The Ki-67 proliferation index was between 5% and 10%.
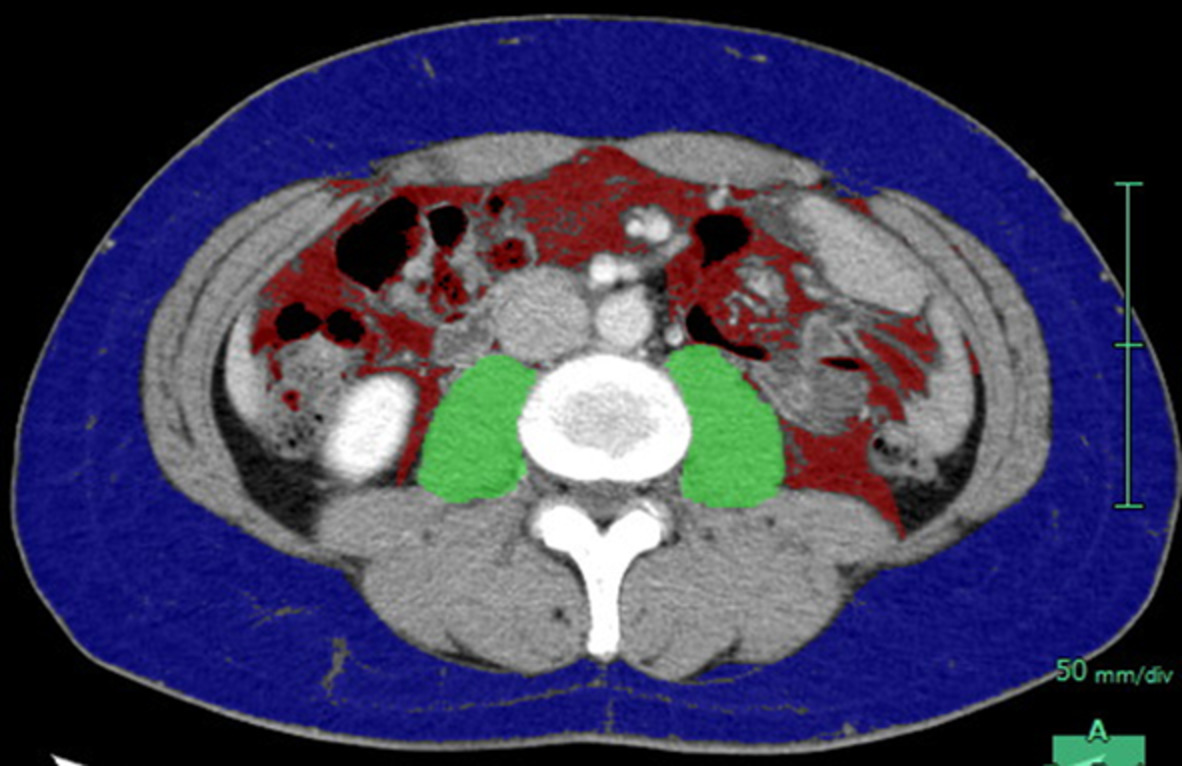
To assess the extent of the tumor, 68Ga–DOTA-TOC PET/CT scan was performed (Figure 2). The scan showed similar degrees of metabolic uptakes in the lung parenchymal, pleural, and breast lesions. This scan revealed a thyroid lesion, which was not conspicuous on CT and FDG PET/CT (Figure 1). Multifocal bony involvement including the skull, whole spine, left eighth rib, and bilateral pelvic bones was also noted (Figures 1 and 2). In atypical carcinoid tumor with multiple metastasis, identification of the primary site is difficult1 and was not possible in our case. The patient was discharged with no postpartum or fetal complications. The patient is under treatment with Luthathera, a peptide receptor radionuclide therapy using radionucleotide 177Lu with a somatostatin analogue.2

DOTA-TOC PET/CT scan of the patient showing multiple involvement of the pleura, lung parenchyma, breast, lymph nodes, thyroid, and bone
DISCUSSIONThe intriguing and unusual findings of our case can be summarized in three points: (1) multiple pleural lesions mimicking mesothelioma with extensive metastasis, (2) discrepancy of mild symptoms with good performance of the patient and advanced disease status, and (3) extremely rare case of atypical carcinoid in pregnancy. What added to the difficulty of final diagnosis was heterogenous manifestation of each lesion in each organ, to the degree that they could have been mistaken as separate entities.
This case adds to our understanding of atypical carcinoids by reporting the first rare image findings of pseudomesotheliomatous manifestation in pregnancy. Imaging features of typical and atypical carcinoid tumors in the lungs are similar: well-defined lobulated spherical, ovoid nodule, or mass. Unlike the usual findings, our case presented with multiple pleural nodules manifesting as malignant mesothelioma, deserving the name “pseudomesotheliomatous carcinoma (PCL).” PCL was first introduced in 1976 by Harwood et al. as a subtype of lung cancer3 but currently is understood to describe a condition mimicking malignant mesothelioma clinically, radiologically, or pathologically. It is a pathologically heterogeneous tumor with a poor prognosis.4 The most common cause of PCL is lung adenocarcinoma.5 Atypical carcinoid presenting as PCL is extremely rare, with only two cases having been previously reported, both by Hengel et al.6 (Table 2).
TABLE 2. Reported cases of atypical carcinoid with pseudomesotheliomatous manifestation Case no. Author (year) Age/sex CT Initial diagnosis Final diagnosis route Therapy follow-up/outcome Thoracic involvement Pleural effusion Extrapleural extension Other findings 1 P van Hengel et al. (2001) 73/M Right pleura Right Right kidney Enlarged mediastinal LNs Mesothelioma Autopsy Conservative care/expired 2 P van Hengel et al. (2001) 73/M Bilateral pleura Left Peritoneum, subcutaneous fat, liver Alveolar consolidation, lingular atelectasis, enlarged mediastinal LNs Mesothelioma Autopsy Conservative care/expired 3 Kim et al. (2021) This study 35/F Right pleura and LLL Bilateral Bone, thyroid, breast, axillary LN No mediastinal LN enlargement Mesothelioma Biopsy Lutathera Abbreviations: CT, computed tomography; LLL, left lower lobe; LN, lymph node; NA, not available; PET/CT, positron emission tomography/computed tomography; SUVmax, maximum standardized uptake value.The findings of our report provide new insights that atypical carcinoid tumor with extensive metastasis in multiple organs can present with different degrees of CT attenuation and FDG uptake between and within organs, even those with identical histology. Carcinoids are highly vascular tumors that exhibit strong homogeneous enhancement on contrast-enhanced CT.7, 8 Atypical carcinoids are reported to show relatively more heterogeneous enhancement and be located in peripheral lungs.9 While the imaging characteristics of primary or metastatic tumor in each organ is well-established, heterogeneous attenuation among all metastatic lesions has not been reported. Similar to CT findings, FDG PET/CT findings of carcinoid tumors show variable metabolic activity. According to Meisinger et al., FDG uptake was positive in 50% of cases in a study with both typical and atypical carcinoid tumors.7 A study by Moore et al. used the cutoff value of SUV 6 and showed that only 17% of atypical carcinoids were above the cutoff value.10 Some studies reported positive correlation of FDG uptake and lesion size,11, 12 but different FDG uptake in metastatic atypical carcinoids has not been previously reported. Our case showed variable vascularity and metabolic activity for pleural, lung parenchymal, breast, right axillary lymph node, thyroid, and bone lesions. While the breast lesion exhibited strong enhancement up to 135 Hounsfield Units (HU), the enhancement of pleural lesions ranged between 25 to 113 HU. Interestingly, tissues obtained from the pleura and breast, even with different vascularity and metabolic activity, were identical in histology. The 68Ga–DOTATOC PET/CT scan showed equally high uptake for all lesions, reflecting somatostatin receptor activity and functionality.13 In summary, even with the same histological findings and functionality, atypical carcinoid lesions can exhibit heterogeneous attenuation and FDG uptake between and within organs in a patient.
The biggest takeaways of this case is the patient's clinical course of progression of the indolent pathology for an extended period of time, leading to good performance status even with extensive tumor involvement. Tumors with extensive metastasis are usually deemed aggressive. However, when a patient's general condition is contradictorily good compared with their tumor involvement status, long-standing presentation of an indolent tumor should be suspected. In our case, chronic pelvic pain could have been an early manifestation of atypical carcinoid involving the pelvic bone. At the time of diagnosis, the patient had extensive metastatic involvement of the pelvic bone without grave symptoms. A similar case has previously been reported by Tun et al.,14 with shoulder pain the only manifestation of underlying extensive metastasis. Carcinoid tumors exhibit indolent behavior, with 5- and 10-year survival rates of atypical carcinoids of 84 and 59%, respectively.15 In addition, indolent tumors harbor long preclinical asymptomatic periods16 and express lower degree of cellular proliferation markers including Ki-67 which correlate with better prognosis.17 In our case, Ki-67 measured between 5%–10%, just above the reference range for atypical carcinoid of 5%,18 and this also supports the indolent course of disease progression. In addition, radiological heterogeneity might have been accentuated by indolent progression of the tumor, with the plasticity among metastatic lesions allowing different degrees of tumor progression and differentiation. Altogether, the contradictory findings of extensive metastasis and good performance status can be attributed to long-standing presentation of indolent tumor.
The effect of pregnancy in the course of carcinoid tumors remains unclear,19 with some reports of spontaneous regression following pregnancy.20, 21 Possible adverse effects of carcinoid tumors on pregnancy have been suggested, including complications such as fetal loss and preterm delivery.19, 22 In our case, the patient’s CT scans of 1-month intervals exhibited no significant change. Even with an indolent course of the carcinoid tumor, considering possible early manifestation at 2 years prior, the effect of pregnancy on the tumor remains unclear in the case reported here. The patient delivered the term baby at 38 weeks' gestation without fetal or maternal complications.
In conclusion, we present the first case of an atypical carcinoid tumor with pleural involvement in a pregnant woman. In our case, the tumors were located mainly in the pleura with different degrees of enhancement. The characteristics of the imaging findings were complicated by the good performance status of the patient. We ascribe this discrepancy between performance status and aggressive image findings to indolent tumor progression. Also, our case presented with variable enhancement and metabolic activity of metastatic lesions in an atypical carcinoid tumor, adding depth to the understanding of metastatic atypical carcinoid tumors.
ACKNOWLEDGMENTSThe authors deeply appreciate Professor Jungho Han, MD, a thoracic pathologist, for his dedication to reviewing the pathology and providing help with interpretation of the case.
CONFLICT OF INTERESTThe authors declare no potential conflicts of interest.
留言 (0)