
記住我

BRAF mutations are detected in 1%–3% of lung cancer, predominately in lung adenocarcinoma, with the BRAF V600E mutation representing approximately half of all BRAF mutations.1-3 Acquired BRAF V600E mutation can occur in tumors with EGFR mutation and is suspected as a resistance mechanism to third-generation EGFR-tyrosine kinase inhibitors (TKIs).4, 5 Vemurafenib and osimertinib have been reported to have marked clinical activity in non-small cell lung cancer (NSCLC) patients with BRAF V600E and EGFR T790M mutation, respectively.6, 7 Ho et al. first proposed the synergistic effectiveness of the blockade of EGFR plus BRAF mutation in a lung cancer patient in an in vitro study.8 However, the treatment strategy of coexistence of EGFR and acquired BRAF mutation with heterogeneity in lung cancer has not been systematically established. In this study, the patient who progressed on osimertinib and developed acquired BRAF V600E mutation with heterogeneity between primary and metastatic lesions, responded well to concurrent therapy with vemurafenib and osimertinib.
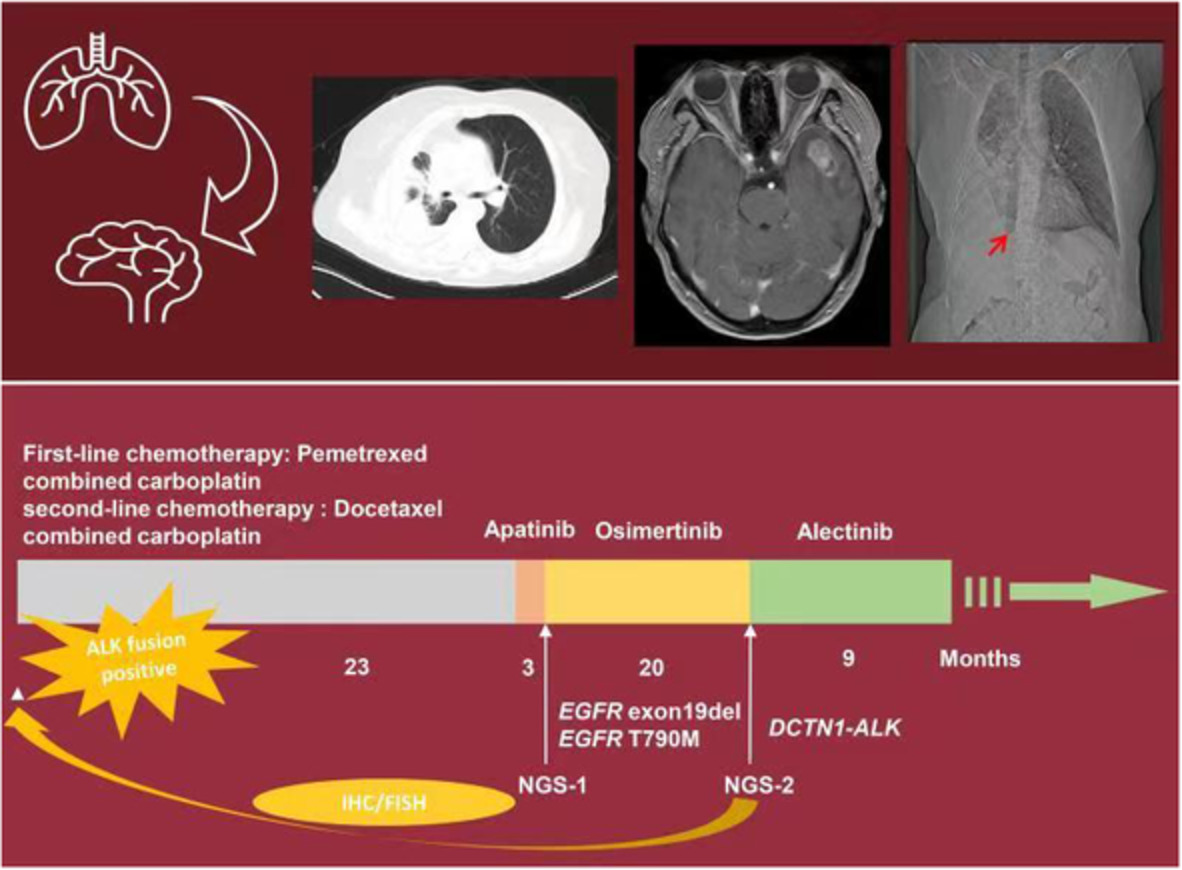
CASE REPORTA 46-year-old woman with no history of smoking was admitted to hospital in June 2016 for further diagnosis and treatment. She was found to have a mass in the upper lobe of the right lung and multiple nodules in both lungs and subpleural location revealed by a chest computed tomography (CT) scan during a medical examination. No enlarged lymph nodes or distant metastasis were detected on brain magnetic resonance imaging (MRI) and positron emission tomography computed (PET-CT). Pathological assessment confirmed the diagnosis of lung adenocarcinoma following transbronchial and percutaneous lung biopsy (T2N0M1 IV). Quantitative real-time PCR was positive for EGFR mutation (19 exon deletion), and daily oral doses of gefitinib (250 mg once daily) were administered. Regular physical review showed stable disease (SD) until January 2018. Chest CT imaging showed the mass had increased in size. The patient had progression-free survival (PFS) of 18.5 months when no distant metastasis had been detected. Quantitative real-time PCR detected the emergence of T790M mutation and the patient commenced treatment with osimertinib (80 mg once daily) from mid-January 2018. In June 2018, pericardial effusion and multiple metastatic lesions were revealed by chest CT, indicating progressive disease (PD). Whole-exome sequencing (WES) of the pericardial effusion showed EGFR mutation (19 exon deletion) and BRAF V600E mutation. From mid-July 2018, osimertinib therapy was discontinued, and the BRAF inhibitor vemurafenib, at a dose of 480 mg twice daily, was started. After 3 months, chest CT showed shrinkage of the majority of the metastatic lesions which suggested the effectiveness of vemurafenib. However, the size of the primary lesion in the right upper lobe had increased. Given the progression of the primary lesion was noted, the patient was commenced on osimertinib 80 mg once daily plus vemurafenib 480 mg twice daily from October 17, 2018. However, she developed intolerable palpitation and fatigue (grade 3), which are drug-related symptoms. Vemurafenib was subsequently reduced to 240 mg twice daily. After 3 months of combined therapy, notable shrinkage of the primary and metastatic lesions were observed, suggesting partial response (PR) of the disease. All combined therapy-related adverse events after the reduction in the dose of vemurafenib, including palpitations and rash (grade 2), were tolerable. In May 2019, the disease progressed with PFS of 7 months following presentation of the patient with dyspnea, and bilateral pleural effusion revealed by chest CT scan. Gene testing of the left pleural effusion identified EGFR mutation (19 exon deletion) and BRAF V600E mutation. We considered adding a MEK inhibitor; however, the patient refused to use this drug due to its lack of availability and absence of sufficient clinical data. She subsequently commenced chemotherapy and after two cycles of pemetrexed plus carboplatin, the chest CT scan showed enlargement of the left side of the lesion and shrinkage of the right side of the lesion. Hence, she was switched to four cycles of gemcitabine plus osimertinib 80 mg once daily. However, the disease was not controlled and the clinical condition of the patient worsened with tumor progression. The patient subsequently died in August 2020, with OS of nearly 4 years. The treatment timeline is shown in Figure 1.

Treatment history of the patient in the study
DISCUSSIONDrug resistance represents a major challenge in targeted therapy, including therapeutic strategies of acquired BRAF V600E mediated resistance to osimertinib. We first determined that the use of osimertinib and vemurafenib could concurrently overcome osimertinib resistance induced by BRAF V600E. In the case reported here, the treatment with the single-agent vemurafenib was effective for metastatic lesions but the primary lesion progressed; however, a partial response for both primary and metastatic lesions was achieved after concurrent therapy with osimertinib and vemurafenib, which exhibited distinct tumor subclones harboring different alterations and displaying distinct responses to respective inhibitors, suggesting tumor heterogeneity between the primary and metastatic lesions. What is special is that the two alterations EGFR and BRAF, respectively located in different sites, clearly showed the responses of two alterations to different drugs, which illustrates the heterogeneity between different driver genes following acquired resistance and assists in optimization of the treatment strategy during targeted therapy. From the perspective of anticancer therapy response with several instances of disease progression, the single agent, whether vemurafenib or osimertinib, was only able to block the corresponding pathway but could not inhibit another pathway that contributes to acquired resistance. Therefore, combined targeting of EGFR and BRAF is the treatment strategy for triggering regression of osimertinib resistance. It appears that the concurrent combination of osimertinib and vemurafenib is the result of a process of gradual exploration and generally achieved success.
Of note, the emergence of BRAF V600E mutation and loss of EGFR T790M mutation were revealed in the metastatic lesion of our patient. The concurrent combination treatment of osimertinib and vemurafenib is an alternative treatment to overcome such a resistance pattern to osimertinib. Solasslo et al.9 reported one patient with the same genotype at baseline and disease progression. The patient received dabrafenib and trametinib therapy alternating with osimertinib followed by osimertinib progression and responded to this sequential treatment for 6 months. Compared with the three anticancer drugs used in the case by Solasslo et al., there were only two drugs administered to our patient, which possibly lightens the burden for patients, including the cost of medication and side effects. However, the optimized treatment of such resistance patterns needs to be explored further. In previous studies,10-12 there have been three patients with a different genotype of resistance to osimertinib induced by BRAF, who carried EGFR classical mutation plus T790M mutation and acquired BRAF V600E mutation. They responded well to the concurrent combination of dabrafenib and trametinib plus osimertinib and one patient obtained PFS of 13.4 months.10 Treatment in another two cases was ongoing at the time of the case reports, with PFS of more than 3 and 7.4 months, respectively.11, 12 Despite the limited number of patients treated, promising results have been achieved with the combined targeting of EGFR and BRAF triggering regression of osimertinib resistance.
Although additional adverse events occurred when patients were treated with a combination of vemurafenib and osimertinib (new adverse events not including the respective side effects of vemurafenib and osimertinib), the relevant toxicities were generally mild to moderate in severity and manageable through dosing modifications and supportive medical care. The patient in our case did not receive the full dose of vemurafenib because of her poor condition; furthermore, there was a dose reduction of vemurafenib due to toxicity. At present, the combination therapy dose of BRAF/MEK inhibitor and EGFR-TKI has not been standardized. As reported in previous studies,9-12 different doses of drugs, especially BRAF/MEK inhibitors, have resulted in different adverse events. Given the effectiveness and low risk of combined therapy, well-designed dose escalation clinical trials on coinhibition of EGFR and BRAF mutation used in patients with osimertinib-induced BRAF V600E mutation are rationable.
In conclusion, this case highlights the consideration of heterogeneity between multiple lesions and proposes that combined targeting is the key to treatment during targeted therapy. Here, we provide a successful example of concurrent treatment with vemurafenib and osimertinib for triggering the regression of osimertinib resistance induced by BRAF mutation with heterogeneity between multiple lesions. Clinical studies with larger samples are needed in the future.
CONFLICT OF INTERESTThere are no conflicts of interest in this study.
留言 (0)