
記住我
Diabetic ketoacidosis (DKA) is one of the most serious and acute metabolic failures in diabetes. In the 1970s, the mortality rate from DKA was reported to be 10%.1, 2 Since then, the overall mortality from DKA has decreased to <1%,3, 4 although it remains higher than 5% in the elderly,5 and intensive treatment is still required. When treating DKA, insulin administration and correction of dehydration through fluid replacement are essential. Intravenous insulin infusion at an initial rate of 0.1 U/kg/h has been recommended for adults.6, 7 For treatment of pediatric DKA, some reports have recommended a dose of 0.05 U/kg/h.8, 9 Notably, Japanese adult DKA patients are often treated with an insulin dose lower than 0.1 U/kg/h,10, 11 because Japanese patients exhibit less insulin resistance than Caucasians.12 It has also been reported that fluid replacement itself corrects hyperglycemia, but the recommended dose differs among reports.6, 13 In addition, glucose is generally infused after blood glucose falls to a level below 200 or 250 mg/dL, but the optimal dose has not yet been investigated. Therefore, treatment guidelines for DKA are still not fully established, especially for Asian patients, who are smaller in size than Americans/Europeans.
The average time required for resolution of DKA is between 10 and 18 h.14, 15 However, that may vary depending on the treatment options and the patient's condition. Generally, venous pH,  , and anion gap (AG) are measured to evaluate the acid–base balance and assess the resolution of DKA.6 We performed this retrospective cohort study to reconsider the optimal treatment for Asian DKA patients through evaluation of the initial doses of both insulin and glucose and the amount of fluid replacement.
, and anion gap (AG) are measured to evaluate the acid–base balance and assess the resolution of DKA.6 We performed this retrospective cohort study to reconsider the optimal treatment for Asian DKA patients through evaluation of the initial doses of both insulin and glucose and the amount of fluid replacement.
This was a retrospective cohort study from a single institution in Japan. Between May 2016 and April 2021, 42 adult patients (≥18 years old) were admitted to St. Marianna University School of Medicine Hospital and treated in our department after being diagnosed with DKA. Therefore, patients who were determined by emergency physicians and nephrologists to require mechanical ventilation or renal replacement therapy in the ICU department were not considered eligible. DKA was defined as a laboratory blood glucose ≥250 mg/dL,  < 18 mmol/L, and pH <7.30. Exclusion criteria were receipt of a SGLT-2 inhibitor (n = 6) or initial management, including insulin infusion, at another facility before arrival (n = 2). The remaining 34 patients were enrolled in the study and divided into two groups: (i) the early resolution group (ER group), which consisted of 21 patients in whom venous pH >7.30,
< 18 mmol/L, and pH <7.30. Exclusion criteria were receipt of a SGLT-2 inhibitor (n = 6) or initial management, including insulin infusion, at another facility before arrival (n = 2). The remaining 34 patients were enrolled in the study and divided into two groups: (i) the early resolution group (ER group), which consisted of 21 patients in whom venous pH >7.30,  ≥ 15 mmol/L, and AG ≤ 12 mmol/L (that is, resolution of DKA) was reached within 18 h from the start of treatment; and (ii) the delayed resolution group (DR group), which consisted of 13 patients in whom DKA resolution was not reached within 18 h (Fig. 1). The threshold of 18 h determined by the average time required for resolution of DKA: 10–18 h.14, 15
≥ 15 mmol/L, and AG ≤ 12 mmol/L (that is, resolution of DKA) was reached within 18 h from the start of treatment; and (ii) the delayed resolution group (DR group), which consisted of 13 patients in whom DKA resolution was not reached within 18 h (Fig. 1). The threshold of 18 h determined by the average time required for resolution of DKA: 10–18 h.14, 15

Flowchart of study participants. SGLT-2, sodium-glucose cotransporter 2.
OutcomesWe compared the baseline characteristics and treatment-related parameters between two groups. The baseline characteristics included age, gender, ethnicity, diabetic type, body weight, body mass index, vital signs, HbA1c, blood glucose, serum creatinine, venous pH, serum  , AG, β-hydroxybutyrate, serum C-peptide, C-reactive protein, time intervals to resolve DKA, proportions of patients with infectious disease and respiratory failure, and outcomes. The patients with infection disease were defined as receiving antibiotic therapy or having some evidence of an infection, and the patients with respiratory failure were defined, as their peripheral blood oxygen saturation was lower than 90%.
, AG, β-hydroxybutyrate, serum C-peptide, C-reactive protein, time intervals to resolve DKA, proportions of patients with infectious disease and respiratory failure, and outcomes. The patients with infection disease were defined as receiving antibiotic therapy or having some evidence of an infection, and the patients with respiratory failure were defined, as their peripheral blood oxygen saturation was lower than 90%.
For insulin infusion, the treatment-related parameters were initial doses, maximum doses, and total amount administered over 18 h. For fluid replacement, the treatment-related parameters were amount administered in the first hour and total amount administered per body weight over 18 h. For glucose infusion, the treatment-related parameters were blood-glucose levels at the start of glucose administration, elapsed time until glucose administration, initial dose, dose per body weight (i.e., initial glucose infusion rate [GIR]), and total amount per body weight over 18 h. In addition, the percentages of patients initially administered an insulin bolus and/or sodium bicarbonate were determined.
Statistical analysisResults are presented as the mean (standard deviation), median ([interquartile range]), frequencies, and proportion unless otherwise stated. Clinical parameters were compared between two groups using paired Student's t-test and the Mann–Whitney U test for continuous variables and the χ2 test for discrete variables. Multivariable logistic regression analysis was performed using explanatory variables, which were the parameters showing significant differences between the two groups. A receiver operating characteristic (ROC) curve analysis was performed using the Youden index to determine the optimal cut-off point for variables to resolve DKA within 18 h. Values P < 0.05 were considered statistically significant. All analyses were performed using JMP 14.2.0 (SAS Institute, Cary, NC, USA).
RESULTS Baseline characteristicsThe baseline characteristics of the patients are shown in Table 1. All patients were Japanese. β-hydroxybutyrate was significantly lower in the ER than the DR group (7.2 [3.2] versus 9.9 [2.6] mmol/L; P = 0.024) and  was significantly higher in the ER than the DR group (11.2 [4.1] versus 7.7 [3.1] mmol/L; P = 0.014). However, no significant differences were observed for other baseline characteristics. All patients recovered from their DKA and were discharged.
was significantly higher in the ER than the DR group (11.2 [4.1] versus 7.7 [3.1] mmol/L; P = 0.014). However, no significant differences were observed for other baseline characteristics. All patients recovered from their DKA and were discharged.
 (mmol/L)
9.9 ± 4.1
11.2 ± 4.1
7.7 ± 3.1
0.014*
Anion gap (mmol/L)
25.5 ± 5.2
25.4 ± 5.7
25.7 ± 4.4
0.866
β-hydroxybutyric acid (mmol/L)
8.4 ± 3.2
7.2 ± 3.2
9.9 ± 2.6
0.024*
Serum C-peptide (ng/mL)
0.35 [0.10–0.93]
0.15 [0.10–0.83]
0.55 [0.10–1.13]
0.451
CRP (mg/dL)
0.26 [0.12–3.18]
0.20 [0.08–1.33]
0.19 [0.14–2.85]
0.607
Time interval to resolve diabetic ketoacidosis (h)
16.6 [12.0–21.2]
12.8 [9.3–15.8]
27.9 [21.3–31.7]
–
Infection disease (%)
6 (17.6)
3 (14.3)
3 (23.1)
0.653
Respiratory failure (%)
2 (5.9)
2 (9.5)
0 (0.0)
0.513
Outcome (recovered)
34/34
21/21
13/13
–
BMI, body mass index; HbA1c, hemoglobin A1c; CRP, C-reactive protein.
Data are expressed as the mean ± standard deviation or median [interquartile range] for continuous variables or the number (%) for categorical variables.
Treatment-related parameters
(mmol/L)
9.9 ± 4.1
11.2 ± 4.1
7.7 ± 3.1
0.014*
Anion gap (mmol/L)
25.5 ± 5.2
25.4 ± 5.7
25.7 ± 4.4
0.866
β-hydroxybutyric acid (mmol/L)
8.4 ± 3.2
7.2 ± 3.2
9.9 ± 2.6
0.024*
Serum C-peptide (ng/mL)
0.35 [0.10–0.93]
0.15 [0.10–0.83]
0.55 [0.10–1.13]
0.451
CRP (mg/dL)
0.26 [0.12–3.18]
0.20 [0.08–1.33]
0.19 [0.14–2.85]
0.607
Time interval to resolve diabetic ketoacidosis (h)
16.6 [12.0–21.2]
12.8 [9.3–15.8]
27.9 [21.3–31.7]
–
Infection disease (%)
6 (17.6)
3 (14.3)
3 (23.1)
0.653
Respiratory failure (%)
2 (5.9)
2 (9.5)
0 (0.0)
0.513
Outcome (recovered)
34/34
21/21
13/13
–
BMI, body mass index; HbA1c, hemoglobin A1c; CRP, C-reactive protein.
Data are expressed as the mean ± standard deviation or median [interquartile range] for continuous variables or the number (%) for categorical variables.
Treatment-related parameters
Comparisons of the treatment-related parameters between two groups are shown in Table 2. The initial insulin dose was significantly higher in the ER than the DR group (0.053 [0.021] versus 0.031 [0.014] U/kg/h; P = 0.003). However, no significant differences were observed in other parameters about insulin. There was also no significant difference in parameters about fluid replacement, glucose and others except for the initial amount of glucose infused (6.44 [2.83] versus 8.84 [3.10] g/h; P = 0.039). By contrast, no significant difference was observed in the initial GIR.
Table 2. Comparison of treatment-related parameters between the early and delayed resolution groups Treatment Early resolution group (n = 21) Delayed resolution group (n = 13) P Insulin Initial dose (U/kg/h) 0.053 ± 0.021 0.031 ± 0.014 0.003** Maximum dose (U/kg/h) 0.061 ± 0.020 0.045 ± 0.024 0.222 Total amount for 18 h (U) 47.1 ± 22.8 37.4 ± 21.0 0.237 Fluid replacement Initial replacement in the first hour (mL) 795.2 ± 534.9 784.6 ± 483.3 0.955 Total fluid amount for 18 h (mL/kg) 56.1 ± 14.8 65.7 ± 19.7 0.127 Glucose BG level at the start of glucose administration (mg/dL) 267.2 ± 96.4 331.8 ± 122.2 0.107 Elapsed time until glucose administration (h) 6.71 ± 3.33 9.23 ± 4.63 0.083 Initial dose (g/h) 6.44 ± 2.83 8.84 ± 3.10 0.039* Initial GIR (mg/kg/min) 1.90 ± 0.82 2.36 ± 1.01 0.170 Total amount for 18 h (g/kg) 1.75 ± 0.72 1.74 ± 1.07 0.960 Others Patients who received an initial bolus of insulin, n (%) 6 (28.6) 3 (23.1) 0.724 Patients who received initial sodium bicarbonate, n (%) 2 (9.5) 3 (23.1) 0.278 BG, blood glucose; GIR, glucose infusion rate. Data are expressed as the mean ± standard deviation or median [interquartile range] for continuous variables or the number (%) for categorical variables. Identification of the factors affecting early resolution of DKAMultivariable logistic regression analysis was carried out to identify factors affecting the early resolution of DKA. Of the baseline characteristics and treatment-related parameters, the initial insulin dose and the baseline  , which significantly differed between two groups, were set as explanatory variables. Although baseline β-hydroxybutyrate levels also significantly differed between two groups, they significantly correlated with the baseline
, which significantly differed between two groups, were set as explanatory variables. Although baseline β-hydroxybutyrate levels also significantly differed between two groups, they significantly correlated with the baseline  (Pearson's product–moment correlation coefficient value = 0.695; P < 0.001). Therefore, to avoid multicollinearity, we chose baseline
(Pearson's product–moment correlation coefficient value = 0.695; P < 0.001). Therefore, to avoid multicollinearity, we chose baseline  as representative of metabolic acidosis, because there were missing data for the baseline β-hydroxybutyrate, but not
as representative of metabolic acidosis, because there were missing data for the baseline β-hydroxybutyrate, but not  . The analysis showed that the initial insulin dose was significantly associated with early resolution of DKA (odds ratio [OR] for a 0.01 U/kg/h increase, 1.80; 95% confidence interval [CI], 1.05–3.10; P = 0.034) and was independent of the baseline
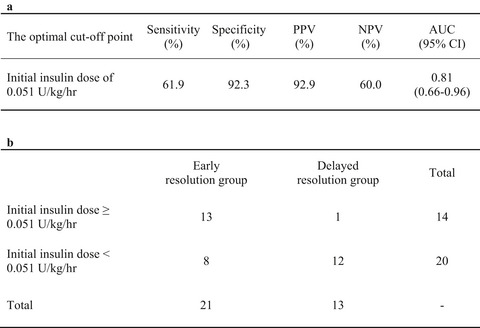
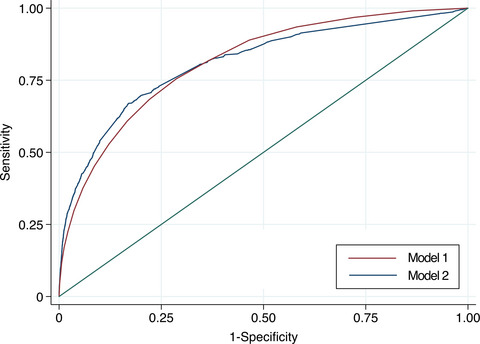
. The analysis showed that the initial insulin dose was significantly associated with early resolution of DKA (odds ratio [OR] for a 0.01 U/kg/h increase, 1.80; 95% confidence interval [CI], 1.05–3.10; P = 0.034) and was independent of the baseline  (Table 3). ROC curve analysis was then performed to identify the optimal cut-off point for the initial insulin dose (Fig. 2). The Youden index revealed that a cut-off point of 0.051 U/kg/h for the initial insulin dose provided the optimal balance between sensitivity and specificity for the early resolution of DKA (Table 4). As shown in Table 4b, these results mean that 92.3% of the patients in the DR group had been started with an initial insulin dose <0.051 U/kg/h and that early resolution of DKA was obtained in 92.9% of patients if the initial insulin dose was 0.051 U/kg/h or higher.
(Table 3). ROC curve analysis was then performed to identify the optimal cut-off point for the initial insulin dose (Fig. 2). The Youden index revealed that a cut-off point of 0.051 U/kg/h for the initial insulin dose provided the optimal balance between sensitivity and specificity for the early resolution of DKA (Table 4). As shown in Table 4b, these results mean that 92.3% of the patients in the DR group had been started with an initial insulin dose <0.051 U/kg/h and that early resolution of DKA was obtained in 92.9% of patients if the initial insulin dose was 0.051 U/kg/h or higher.
 , for every 1 mmol/L increase
1.22
0.95–1.58
0.119
DKA, diabetic ketoacidosis; OR, odds ratio; CI, confidence interval.
This analysis revealed that the initial insulin dose was an only independent factor significantly associated with early resolution of DKA.
, for every 1 mmol/L increase
1.22
0.95–1.58
0.119
DKA, diabetic ketoacidosis; OR, odds ratio; CI, confidence interval.
This analysis revealed that the initial insulin dose was an only independent factor significantly associated with early resolution of DKA.

Receiver operating characteristic curves to determine the optimal cut-off point for the initial insulin dose. AUC, area under the curve. The optimal cut-off point for initial insulin dose was 0.051 U/kg/h determined from the Youden index (sensitivity: 61.9%; specificity: 92.3%; AUC 0.81 [95% confidence interval: 0.66–0.96]).
Table 4. Parameters of the optimal cut-off point for initial insulin dose determined with receiver operating characteristic curve analysis and a cross-tabulation table a The optimal cut-off point Sensitivity (%) Specificity (%) PPV (%) NPV (%) AUC (95% CI) Initial insulin dose of 0.051 U/kg/h 61.9 92.3 92.9 60.0 0.81 (0.66–0.96) b Early resolution group Delayed resolution group Total Initial insulin dose ≥0.051 U/kg/h 13 1 14 Initial insulin dose <0.051 U/kg/h 8 12 20 Total 21 13 – CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; AUC, area under the curve. a: The optimal cut-off point determined by the Youden index (Fig. 2). b: Cross-tabulation table used to determine the optimal cut-off point. DISCUSSIONOur findings indicate that in the treatment of DKA in Asian patients, an initial insulin dose of 0.05 U/kg/h would be generally necessary to provide an early resolution of their DKA. On the other hand, a dose lower than 0.05 U/kg/h may delay DKA resolution. This dose is lower than is generally recommended in western countries. For example, the United States (US) and United Kingdom (UK) guidelines recommended an initial insulin dose of ~0.1 U/kg/h.6, 7 In 1976, Kitabchi et al.16 showed in a randomized controlled trial that a dose of 0.1 U/kg/h could improve hyperglycemia with fewer adverse effects than were seen with a dose of 1.0 U/kg/h. They subsequently reported that a dose of 0.07 U/kg/h following a priming injection could achieve outcomes comparable to those achieved with 0.14 U/kg/h.17 On the other hand, an insulin dose of 0.07 U/kg/h without a priming injection reduced blood glucose and ketone body levels at a slower rate than higher doses. Nonetheless, no significant difference was observed in the time to DKA resolution between the two groups.
During insulin therapy, the decline in blood glucose is the result of multiple of insulin effects, including suppression of hepatic gluconeogenesis, stimulation of peripheral glucose uptake, and renal glycosuria.18 Among them, suppression of hepatic glucogenesis is thought to be particularly important, and plasma insulin levels of 80–100 μU/mL are required to offset hepatic insulin resistance.19 Therefore, it is recommended that any insulin therapy for DKA achieves those levels,8 and a dose of 0.1 U/kg/h reportedly achieves a plasma insulin level much higher than that (100–200 μU/mL).16, 20 Additionally, a dose of 0.1 U/kg/h reportedly suppresses hepatic gluconeogenesis by ~50%,18 which may be one of the reasons for the efficacy of that dose.
However, most of the patients in those studies are not Asians, and Fukushima et al.12 reported that Japanese patients exhibit less insulin resistance than Caucasians. It is, therefore, likely that the initial insulin dose recommended for treatment of American/European DKA patients may be excessive for Asian patients. Similarly, several clinical studies recently recommended a dose of 0.05 U/kg/h for treatment of pediatric DKA because there is a concern that the rapid decrease in blood glucose could lead to cerebral edema.9, 21, 22 When treating DKA, an excessively rapid decrease in blood glucose (>100 mg/dL/h) should be avoided because the rapid change in serum osmolarity can increase the risk of cerebral edema.23 A prospective study comparing high-dose (0.1 U/kg/h) and low-dose (0.05 U/kg/h) insulin in pediatric DKA patients reported that cerebral edema occurred only in the high-dose group (in 1 of 25 participants).8 In light of the risk of administering insulin at too high a dose, we suggest using a lower initial insulin dose when treating DKA in Asian patients, who have less insulin resistance than Americans/Europeans.
For initial fluid replacement in DKA patients, 15–20 mL/kg/h during the first hour is recommended in the US guidelines, and 1 L in each of the first 2 h is recommended in the UK guidelines.24 Injection of insulin is not recommended during the first hour23 because fluid replacement alone reduces hyperglycemia, serum osmolality, and acidosis because of a decrease in counter-regulatory hormones, decreased peripheral insulin resistance, and increased renal prefusion.25 Blood glucose levels are reportedly decreased by an average of 109 mg/dL by these multiple effects.23 In the present study, the initial fluid replacement tended to be less than suggested in the US and UK guidelines, and there was no significant difference between two groups.
Once the blood glucose level reaches 200–250 mg/dL, it is recommended that glucose administration be initiated to continue insulin infusion until the ketosis is corrected while avoiding hypoglycemia.6, 13 In the present study, the initial glucose infusion rate was significantly lower in the ER than DR group, but the initial infusion rate of glucose per body weight (i.e., initial GIR) did not significantly differ between the two groups.
LimitationsBecause this study is a retrospective cohort study, its interpretation is limited. Although a prospective study of treatments for DKA in Asian patients is awaited, ethical guidelines would make it difficult to perform randomized trials with sufficient informed consent during emergency medical care. In addition, this study did not include extremely severe cases that required management in the ICU with administration of mechanical ventilation and/or renal replacement therapy. Therefore, to apply the results of this study to clinical practice, indications for mechanical ventilation or renal replacement therapy should be assessed. Mechanical ventilation is needed for hypoxemia, hypercapnia, shock, or altered mental status. Renal replacement therapy is for severe azotemia or hyperkalemia with severe oliguria or anuria. Such severe conditions may require further adjustment of insulin infusion, fluid replacement, and glucose infusion.
CONCLUSIONFor treatment of DKA in Asian patients, an initial insulin of 0.05 U/kg/h would be necessary to provide an early resolution of the DKA. However, a dose lower than 0.05 U/kg/h may delay DKA resolution. These results provide practical information supporting the acute phase treatment of DKA in Asian patients.
ACKNOWLEDGEMENTSThe authors are indebted to Yuko Yasuda for her expert assistance.
DISCLOSUREApproval of the Research Protocol: The study protocol was approved by the Human Ethical Committee of St. Marianna University School of Medicine (No. 4606) on December 5, 2019. This study was performed according to the ethical guidelines of the Declaration of Helsinki with an opt-out methodology.
Informed Consent: The Human Ethical Committee of St. Marianna University School of Medicine waived informed consent because we collected and analyzed demographic and clinical data in an anonymized manner.
Registry and the Registration No. of the Study/Trial: Not applicable.
Animal Studies: Not applicable.
Conflict of Interest: None declared.
留言 (0)