
記住我
Since the discovery of the coronavirus disease (COVID-19), significant changes have been made to people’s lifestyles, including avoidance of closed and crowed places, social distancing measures, and wearing of masks to prevent the spread of infection. Considering the significant amount of time an individual wears a mask, it is important to consider the balance between heat exhaustion prevention and daily life activity, and to ensure physical cooling to prevent heatstroke. Moreover, patients with COVID-19 commonly present with fever and hyperthermia, causing difficulties in distinguishing between heatstroke and these symptoms.1, 2 Thus, there is an urgent need to discuss the prevention of heatstroke during this pandemic.
However, the influence of exercise in a hot and humid environment while wearing a mask on the incidence of heatstroke remains unclear.
Therefore, we aimed to measure the influence of wearing masks on the physical status of humans in artificial hot and humid environments.
Materials and Methods Experimental design, subjects, and interventionThis was a prospective experimental study that included human subjects.
Healthy young volunteers without physical or health problems were included in this study. The participants with high (≥37.5 °C) body temperature were excluded. Each participant was exposed to different physical situations, as follows: (i) not wearing a mask (control), (ii) wearing surgical mask (3M surgical mask; bacterial filtration efficiency [BFE], 99%; particle filtration efficiency [PFE], 95%), (iii) wearing a mask for sport use (UNIQLO Airism; BFE, 99%).
Six hours prior to the start of the experiment, the subjects were instructed to stop eating, to ensure precise measurement of the internal core body temperature using an ingestible capsule thermometer (e-Celsius; BodyCap). An emergency physician undertook a health examination on each subject to confirm the stability of their physical status, pre- and postexperiment.
The subjects swallowed an ingestible thermometer and their physical baseline status was measured (body weight, heart rate, respiratory rate, blood pressure, surface body temperature, total body water content, and saturation of percutaneous oxygen [SpO2]). Subsequently, subjects were instructed to perform exercises (standing for 20 min, then walking for 20 min, and running for 20 min on a treadmill [Biomill VO-2000; Sandme]) in an artificial weather room in which the temperature was set at 28°C. The temperature was measured using the internal wet-bulb globe temperature (WBGT),3 calculated with the equation: WBGT = 0.7 × wet-bulb temperature + 0.3 × globe temperature.
The exercise intensity was decided using the Karvonen formula (target heart rate = [(220 − age) − (resting heart rate) × (% of exercise intensity)] + resting heart rate).4
A schematic drawing of the experiment is shown in Figure 1. For each individual, the experiment phases involved three steps: rest (% of exercise intensity = 0), walking (low intensity: % of exercise intensity = 20%), and running phase (moderate intensity: % of exercise intensity = 70%).5 At each step, after deciding the target heart rate using the Karvonen formula, the speed and tilt angle of the treadmill was increased every 2 min by the Bruce method.6 After reaching the targeted heart rate, the speed and tilt angle of the treadmill were maintained for 20 min.

Schema of experiment to determine whether wearing a face mask is a risk factor for heatstroke during increased exercise intensity. Each participant experienced different physical situations: (i) not wearing a mask (control), (ii) wearing a surgical mask, or (iii) wearing a mask for sport use. SpO2, percutaneous oxygen saturation; WBGT, wet-bulb globe temperature.
To ensure the participants’ safety, exercise was discontinued when: (i) core body temperature reached 40°C, (ii) SpO2 decreased by less than 90%, (iii) the Borg scale,7 a scale of rate of perceived exertion, reached 17.
The definition of the incidence of heatstroke followed the Japanese Association for Acute Medicine heatstroke (JAAM-HS) criteria.8 That is, the incidence of heatstroke was diagnosed as any initial symptoms such as vertigo, headache, vomiting, disturbance of consciousness, convulsion, ataxia, and delirium, under hot and humid situations.
One subject was tested every week with different situations with or without a mask; therefore, one subject was tested three times in 3 weeks.
Before the experiment, the study aims and procedures were fully explained to each participant; after receiving a description of the experiment, they signed an agreement to participate in the study. Thus, a statement of consent was obtained from all participants. This study was approved by the Institutional Review Board of Nippon Medical School (A-2020-029).
Body water contentBody water content was measured twice (before and after exercise) by multifrequency bioimpedance using a four-paired electrode bioimpedance device9 (InBody 720). Additionally, several physical parameters, including total body water content, muscle mass, and body fat percentage, were measured.
Saturation of percutaneous oxygen and Pleth variability indexTo measure the respiratory status, the time of initial and end SpO2 were measured in each experimental trial. Additionally, the Pleth variability index (PVI) was measured for intravenous fluid volume estimation.10 Both SpO2 and PVI were measured using a Radical-7 monitor (Masimo).
Liver fatty acid-binding protein measurementTo estimate the level of dehydration, the urinary concentration of liver fatty acid-binding protein (L-FABP) was measured.11 In each subject, urinary samples (5 ml) were collected before and after exercise loading, and were stored at −80°C. Before batch analysis, urine samples were defrosted at air temperature. Urinary L-FABP concentrations were analyzed using an enzyme-linked immunosorbent assay with the Human L-FABP Kit (Sekisui Medical), according to the manufacturer’s instructions.
Statistical analysisA previous report stated that at least six participants are needed to estimate the relationship between mask wearing and physiological estimation.12 The numerical data are presented as median and interquartile range. Categorical variables were compared using Fisher’s exact test. The influence of time, face mask type, and their interactions on these human physiological and psychological responses were analyzed using repeated two-way measures ANOVA and the Wilcoxon signed rank test. StatFlex (Artech) was used to analyze the data. Statistical significance was set at p < 0.05.
Results Subject characteristicsSix young Japanese men were included in this study. Their median age was 19.5 years (interquartile range, 19.0–21.0 years) and median body mass index was 23.2 g/m2 (22.6 g/m2–24.1 g/m2). All patients had normal and stable physical status. Additionally, all vital signs were within normal range: baseline systolic blood pressure, 127.5 mmHg; baseline heart rate, 76.0 b.p.m.; baseline respiratory rate, 18.0 breaths/min; and baseline SpO2, 98.0% in room air (Table 1). None of the participants had any comorbidities. In addition, the physical data of all participants were similar. The detailed characteristics are shown in Table 1.
Table 1. Characteristics of human subjects (n = 6, male) in an experiment to determine whether wearing a face mask is a risk factor for heatstroke during increased exercise intensity Subject no. 1 2 3 4 5 6 Median (IQR) Age (years) 21 19 19 21 19 20 19.5 (19.0–21.0) Height (cm) 177 169 175 162 176 160 172.0 (162.0–176.0) Body weight (kg) 73.8 62.1 69.1 59.5 76.0 61.6 65.6 (61.6–73.8) Body mass index (kg/m2) 23.6 21.7 22.6 22.7 24.5 24.1 23.2 (22.6–24.1) Total body water contents (L) 44.3 38.4 44.4 36.2 43.6 32.8 41.0 (36.2–44.3) Muscle mass (kg) 57.0 49.5 57.2 46.6 56.2 42.3 52.5 (46.0-57.0) Body fat percentage (%) 17.9 15.6 12.2 17.0 21.3 27.5 17.5 (15.6–21.3)Initial systolic blood pressure
(mmHg)
111 125 111 141 144 130 127.5 (111.0–141.0)Initial diastolic blood pressure
(mmHg)
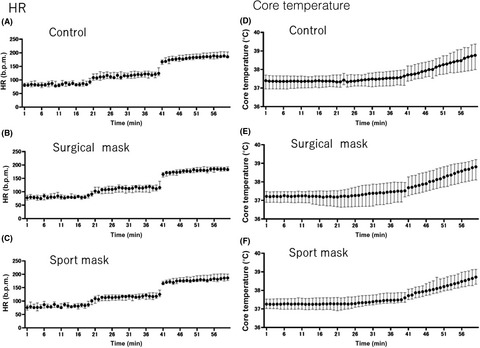
76 73 62 86 96 76 76.0 (73.0–86.0) Initial heart rate (b.p.m.) 59 55 55 73 72 70 64.5 (55.0-72.0) Initial respiratory rate (breaths/min) 17 18 18 18 22 24 18.0 (18.0–22.0) Initial SpO2 (%) 98 98 99 99 97 96 98.0 (97.0–99.0) Abbreviation: IQR, interquartile range. Change over time of core temperature and other vital signsCore temperature and heart rate was significantly increased when exercise intensity was increased (control, 37.4 °C–38.8 °C; surgical mask, 37.2 °C–38.7 °C; and fabric sport mask, 37.3 °C–38.7 °C; Figure 2). However, no significant difference was observed among the three groups (p = 0.74, Figure 3).

Change of heart rate (A–C) and core temperature (D–F) in healthy young men during increased-intensity exercise while not wearing a mask (control), wearing a surgical mask, or wearing a mask for sport use. Heart rate (HR) and core temperature significantly increased; however, no significant difference was observed between the three groups.

Change of core temperature before and after exercise among healthy young men who were not wearing a mask (A), wearing a surgical mask (B), or wearing a sport mask (C). Core temperature significantly increased after exercise; however, no significant difference was observed between groups.
Saturation of percutaneous oxygen, respiratory rate, and PVISaturation of percutaneous oxygen significantly decreased in all six subjects (control, 98.0%–91.0%; surgical mask, 97.0%–94.0%; and fabric sport mask, 98.0%–93.0%; Figure 4A). However, no significant difference was observed regarding SpO2 decrease in the three groups (p = 0.31). Conversely, respiratory rate was increased. However, no significant difference was observed in the three groups (Figure 4B).

Change in the saturation of percutaneous oxygen (SpO2) (A) and respiratory rate (B) in healthy young men during increased-intensity exercise while not wearing a mask (control), wearing a surgical mask, or wearing a mask for sport use. The SpO2 decreased and respiratory rate increased significantly in all subjects; however, no significant difference was observed between groups.
The PVI, a measure of intravenous fluid volume (a high value of PVI indicates dehydration), significantly increased in all six subjects (control, 26.6 to 32.0; surgical mask, 17.5–21.0; and fabric sport mask, 21.6–29.5; Figure 5); however, no significant difference was observed among the groups (p = 0.43, Figure 5).

Values of the Pleth variability index (PVI, %) before and after exercise among healthy young men who were not wearing a mask, wearing a surgical mask, or wearing a sport mask. No significant difference was observed in the PVI values after exercise, or between groups. ns, not significant.
Liver fatty acid-binding proteinIn each subject, no significant increase was observed in the L-FABP pre- and postexercise loading. Furthermore, no significant difference was observed between the groups (median: control, 1.65 ng/ml; wearing surgical mask, 2.63 ng/ml and fabric sport mask, 2.16 ng/ml; p = 0.87; Figure 6).

Change in the concentration of urinary liver fatty acid-binding protein (L-FABP) before and after exercise among healthy young men who were not wearing a mask, wearing a surgical mask, or wearing a sport mask. No significant increase was observed and no significant difference was observed between groups regarding L-FABP levels. ns, not significant.
Incidence of heatstroke and the Borg scaleBased on the JAAM-HS definition, there was no incidence of heatstroke. The average of the Borg scale did not differ among the three groups (median [Borg scale]: no mask, 13.5; surgical mask, 15; and sport mask, 15; Figure 7).

Change in the values of the Borg scale in healthy young men during increased-intensity exercise while not wearing a mask (control), wearing a surgical mask, or wearing a mask for sport use. The value of the Borg scale, a scale of the rate of perceived exertion, did not differ between the intervention arms. There was no incidence of heatstroke, as defined by Japanese Association for Acute Medicine criteria.
DiscussionOur study provides evidence regarding the safety of wearing masks during intensity-controlled exercise under hot and humid conditions. There was no incidence of heatstroke, as defined by JAAM-HS criteria, and none of the participants had health problems. The value of the Borg scale, a scale of the rate of perceived exertion, did not differ between the intervention arms (i.e., control, wearing a surgical mask, and wearing a sport mask).
In this study, the temperature and humidity were controlled in an artificial weather room to create an environment conducive to heatstroke. Healthy young male volunteers were used in the experiment to investigate the physical effects of wearing a mask. To the best of our knowledge, this is the first study to evaluate the effects of wearing a mask in a hot environment on the body. We found similar results between mask-wearing and non-mask-wearing conditions regarding deep body temperature, vital signs, and dehydration level even in a hot environment set at WBGT of 28°C. When the physical load is strictly controlled, exercise can be undertaken safely while wearing a mask even in a hot environment, indicating that mask wearing is not a risk factor for exertional heatstroke.
Roberge et al. instructed healthy volunteers to perform exercise with low to moderate levels of exertion (5.6 km/h; 0° inclination) with and without surgical masks and measured changes in heart rate (9.5 b.p.m.) and respiratory rate (1.6 c.p.m.).13 However, they did not strictly control the temperature or humidity of the laboratory, which were set at 21.5 °C and 23.1%, respectively (WBGT 15°C), which is considered similar to a normal environment. In this study, we created an artificial weather room to recreate an environment of 28°C WBGT, which could contribute to heatstroke; this allowed successful establishment of a situation similar to a real environment.
A previous study found no relationship between mask wearing and core body temperature increase in a normal temperature environment,13 which is consistent with our finding of an increased risk of heatstroke in a hot and humid environment. Therefore, our study shows that wearing a mask is not a risk factor for heatstroke in a hot and humid environment, despite rest or exercise.
As stated earlier, Roberge et al.13 found that wearing a surgical mask at a low to moderate exercise intensity resulted in increased heart and respiratory rates. In contrast, our study found no significant difference in body temperature or vital signs between the mask-wearing and non-mask-wearing groups. This finding could be attributed to the Karvonen method, which strictly controlled exercise intensity; furthermore, our study was undertaken with young healthy volunteers, who may have stronger physical compensatory mechanisms.
Another significant finding of our study is the examination of the effects of fabric masks on the body during exercise. The US Centers for Disease Control and Prevention guidelines recommend the use of fabric masks in addition to surgical masks.14 In particular, multiple polyester masks have been recognized for their droplet control performance. Additionally, this study is significant to the current situation as it collected data regarding the current state of mask use in our country.
In this study, no significant difference was observed regarding the physical effects of wearing a surgical mask or a fabric mask. Few studies have evaluated the performance of fabric masks; however, so-called hybrid fabric masks made of multiple materials have been reported to have VFE of more than 80% and BFE of more than 90%,15 which could indicate similar performance of surgical and fabric masks.
This study was unable to prove that mask wearing was a risk factor for heatstroke. However, we believe that this study accurately measured exercise load and body temperature; therefore, this indicates the safety of performing exercise while wearing a mask in a hot environment.
In this study, we used a capsule-type internal thermometer to measure the deep body temperature. A previous study has reported the usefulness of ingestive thermometers for monitoring body temperature.16 In our study, it was possible to safely observe the deep body temperature for as long as 1 h. In future studies, we aim to use wearable devices and internal organs to measure heart rate and continuous body temperature to ensure the accuracy of measuring deep body temperature using the Karvonen method. This could be effective in preventing heatstroke while working and wearing a mask.
LimitationsThis study has several limitations. First, the number of cases in this study had to be limited due to the human and environmental limitations of the COVID-19 pandemic. Therefore, the detection power might be weak. However, there were no significant differences in body size, muscle mass, or vital signs among the six patients, indicating similar characteristics between patients. Therefore, we believe that the data obtained were more accurate and uniform compared to a large cohort with diverse characteristics.
Second, the experiment was undertaken in the sequence of exercise without mask, then polyester mask, and finally surgical mask; therefore, the possibility of biases, including mental anxiety and tension, could occur. Additionally, there is the possibility that the body load was reduced due to heat acclimatization, or that it was affected by the physical condition of the day or the time of the experiment.
Finally, this experiment included only young men. Therefore, the results might not be applicable to women, the elderly, or children. It is necessary to also consider the effects of blood loss and basal body temperature in women who are menstruating. However, a higher incidence of heatstroke has been observed in male individuals worldwide,17 and it can be said that we obtained practical data that address the current situation.
The elderly are at an increased risk for heatstroke.1, 2, 18 Therefore, further studies are necessary, particularly in monitoring exercise intensity.
ConclusionWe used an artificial weather chamber to create a hot environment conducive to heatstroke. Using this environment, an experiment was undertaken to investigate the effects of mask wearing on the body in healthy young men. Wearing a mask by itself was not a risk factor for exertional heatstroke, and accurate monitoring of exercise intensity based on heart rate could have the potential to reduce the risk of heatstroke.
AcknowledgmentsThis study was supported by a Health and Labor Sciences Research Grant 2020 in Japan (grant no. 20CA2057).
DisclosureApproval of the research protocol: This research protocol was approved by the Institutional Review Board of Nippon Medical School (A-2020-029).
Informed consent: Statement of consent was obtained from all study participants.
Registry and registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of interest: None.
留言 (0)