
記住我

Pulmonary sarcomatoid carcinoma (PSC), an aggressive and poorly differentiated type of non-small cell lung carcinoma (NSCLC), which accounts for only 0.52% of NSCLC,1 has been found to be extremely insensitive to conventional antitumor therapies (surgery, chemotherapy, radiotherapy).2, 3 With rapid tumor growth, early metastasis, and limited efficient therapies, the prognosis for patients with PSC is much poorer than other NSCLC.3, 4 Recently, a growing number of studies have reported that PD-ligand 1 (PD-L1) is commonly overexpressed in PSCs,5-7 which might indicate a novel direction for PSC treatment.
As a humanized IgG4 monoclonal antibody, programmed cell death-1 (PD-1) inhibitor tislelizumab (BGB-A317) was designed to inhibit binding to FcγR on macrophages in order to abolish antibody-dependent phagocytosis and recover T cell clearance.8, 9 With high affinity and binding specificity for PD-1, the clinical efficacy of tislelizumab in NSCLC has gradually been explored in various studies and clinical trials.10-12 However, whether PSC patients can also benefit from tislelizumab therapy or not has not yet been reported. Here, this study reports the favorable outcome in a patient with advanced PSC and PD-L1 overexpression receiving PD-1 inhibitor tislelizumab monotherapy for the first time.
CASE REPORTA 65-year-old female with a history of hypertension sought medical help for cough and breathlessness in October 2020. Physical examination showed diminished breath sounds in the right lower lung fields without rales. Enhanced chest computed tomography (CT) demonstrated a large space-occupying lesion (6.6 x 4.9 cm) in the hilus of the upper lobe of the right lung, several nodules in the subpleural region of the right lung with the largest measuring 1.6 x 2.0 cm, a large pleural effusion on the right side, and enlarged hilar and mediastinal lymph nodes. Magnetic resonance imaging (MRI)-guided aspiration biopsy in the occupying lesion of the right lung was carried out. Immunohistochemistry (IHC) of lung puncture tissue showed Vimentin (+), TTF1 (+), Napsin A (−), CK (AE1/AE3) (+), SMA (−), desmin (−), S-100 (−), Ki-67+ (30%), CD68 (−), CD163 (+), CR (−), WT-1 (−), CK5/6 (−), P40 (−), LCA (−), D2-40 (−), CD56 (−), Syn (−), SOX10 (−), CK7 (−), CEA (−) (Figure 1), and the patient was pathologically confirmed with sarcomatoid carcinoma. Systemic examination did not reveal any metastasis in distant organs, apart from subpleural nodules.

Histopathological stains of the space-occupying lesion of right lung puncture biopsy (a–f). (a) Hematoxylin and eosin, (b) Vimentin (+), (c) TTF1 (+), (d) CK (AE1/AE3) (+), (e) CD163 (+), (f) Ki-67+ (30%)
While waiting for the results of next-generation sequencing (NGS) and PD-L1 expression, chemotherapy consisting of docetaxel 120 mg/d1 and nedaplatin 40 mg days 2–4 q. 21 days, together with intrapleural antiangiogenic endostar injection was commenced on November 6, 2020. One cycle later, although the pleural effusion had decreased, the occupying lesion had enlarged, and serious infection occurred with cough and aggravation of breathlessness.
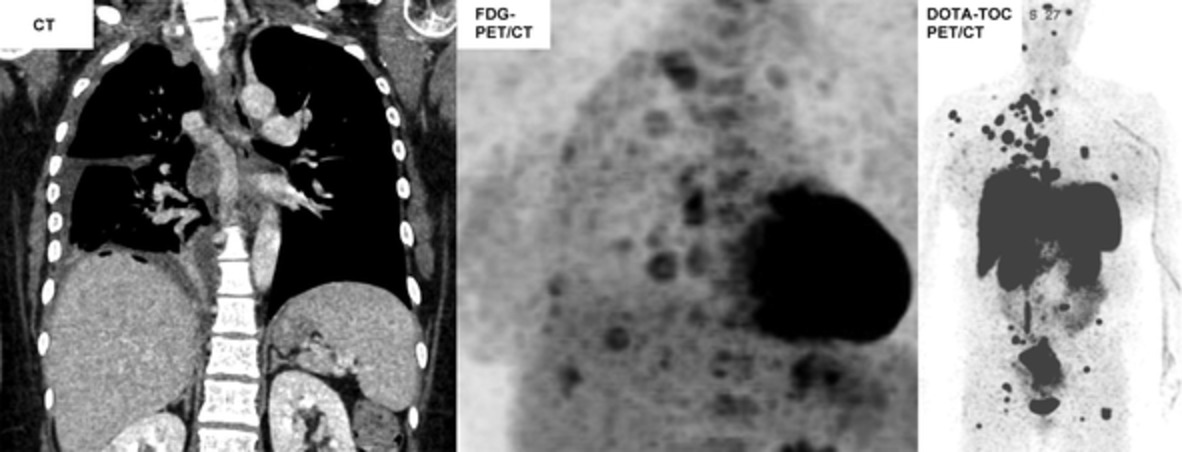
However, the NGS test of the lung puncture tissue and blood showed no druggable driver mutations. Fortunately, IHC showed that PD-L1 was strongly expressed (tumor proportion score [TPS]: 60%, combined positive score [CPS]:90) (Figure 2). The PD-1 antibody tislelizumab 200 mg q. 21 days was implemented on December 29, 2020. One cycle later, the patient's cough and breathlessness had reduced, and chest CT scan showed that the mass (4.1 x 3.9 cm) in the hilus of the right upper lobe of the lung and nodules in the subpleural region of the right lung had shrunk significantly, and the pleural effusion had disappeared. Tislelizumab monotherapy was maintained with a partial response (PR) achieved and no notable side effects occurred. Seven cycles later, the lesions had gradually shrunk to 1.6 x 1.3 cm and remained stable until now. 18F-fluoro-deoxy-glucose positron emission tomography/computed tomography (18F-FDG PET/CT) showed increased FDG uptake in the thyroid (immune-associated) after nine cycles of tislelizumab monotherapy. The results of thyroid function tests were normal. The chest CT scan changes are shown in Figure 3.

Immunohistochemical examination for PD-L1. (a) Positive control, (b) negative control, and (c) the space-occupying lesion of right lung puncture biopsy (tumor proportion score [TPS]: 60%, combined positive score [CPS]:90)

Sequence of chest computed tomography (CT) scan changes across the antitumor treatment timeline. ND, nedaplatin plus docetaxel
DISCUSSIONWith the exploration of cancer immunotherapy, PD-1 and PD-L1 inhibitors have become promising new options for various malignancies and have quickly changed the standard regimens and prognosis for patients with NSCLC .13 Immunotherapy for PSC has also gradually received attention from researchers in several recent case reports.14 In one case, a PSC patient not only benefited greatly from toripalimab monotherapy, but also improved under toripalimab combined therapy (combined with radiotherapy) after disease progression.7 In addition, in a PSC patient with low PD-L1 expression, pembrolizumab with platinum-doublet treatment was reported to have remarkable effects.15 Moreover, even in a PSC patient with resistance to radiotherapy and chemotherapy, pembrolizumab could be a beneficial therapeutic option.16 In addition, the tumor size in a PSC patient without PD-L1 expression decreased under nivolumab treatment, even without smoking cessation. However, immunotherapy for PSCs is still at a preliminary stage.
Tislelizumab was first approved in China for Hodgkin's lymphoma by the National Medical Products Administration (NMPA) in December 2019.17 By blocking PD-L1/PD-L2-associated cell signaling, tislelizumab promotes the production of cytokines, recovered the clearing ability of T cells, thus causing immune-associated tumor cell death.9 Previous studies have documented the high tolerance, high safety, and significant effect of tislelizumab among advanced NSCLC patients, regardless of PD-L1 status.11, 12 After progression, previously treated NSCLC patients acquired another 4 months median progression-free survival under tislelizumab treatment, with 18% (10/56) of patients achieving a partial response and 38% (21/56) patients remaining stable.11 The application of tislelizumab for NSCLC has been gradually approved by NMPA since 2020 (April and June for advanced squamous and nonsquamous, respectively).13 However, for the rarity of PSCs, the antitumor activity of tislelizumab among PSCs has not previously been evaluated. In this study, a PSC patient achieved successful results and no unexpected safety concerns from tislelizumab monotherapy. As a result of its differential PD-1 binding orientation, the off-rate of tislelizumab was 100-fold slower than pembrolizumab and 50-fold slower than nivolumab.11 However, the differences in therapeutic efficacy and side effects between tislelizumab and other PD-1 antibodies for NSCLC still need investigation. With higher affinity than other PD-1 inhibitors, tislelizumab is definitely a potent immunotherapy for PSCs, which deserves further investigation.
This case report does have several limitations. In this study, tislelizumab treatment was carried out as monotherapy, and it is unknown whether combined treatment with conventional antitumor therapies will achieve more or not. Moreover, this case was a patient with advanced PSC with high PD-L1 expression, and the therapeutic effect of tislelizumab among patients at different stages and PD-L1 expression is still unknown. Large cohort studies are urgently needed to elucidate the specific effect of tislelizumab among PSCs.
In conclusion, as far as we know, this is the first study of an advanced PSC case with high PD-L1 expression benefiting from treatment with PD-1 inhibitor tislelizumab monotherapy with a successful outcome, and may bring new hope to PSC patients.
ACKNOWLEDGMENTWe sincerely thank all who assisted with this study.
CONFLICT OF INTERESTAll authors have no conflicts of interest.
REFERENCES
1Rahouma M, Kamel M, Narula N, Nasar A, Harrison S, Lee B, et al. Pulmonary sarcomatoid carcinoma: an analysis of a rare cancer from the Surveillance, Epidemiology, and End Results database. Eur J Cardiothorac Surg. 2018; 53(4): 828– 34. 2Vieira T, Girard N, Ung M, Monnet I, Cazes A, Bonnette P, et al. Efficacy of first-line chemotherapy in patients with advanced lung sarcomatoid carcinoma. J Thorac Oncol 2013, 8(12): 1574– 1577. 3Li X, Wu D, Liu H, Chen J. Pulmonary sarcomatoid carcinoma: progress, treatment and expectations. Ther Adv Med Oncol. 2020; 12:1758835920950207. 4Chen M, Yang Q, Xu Z, Luo B, Li F, Yu Y, et al. Survival Analysis and Prediction Model for Pulmonary Sarcomatoid Carcinoma Based on SEER Database. Front Oncol. 2021; 11: 630885. 5Vieira T, Antoine M, Hamard C, Fallet V, Duruisseaux M, Rabbe N, et al. Sarcomatoid lung carcinomas show high levels of programmed death ligand-1 (PD-L1) and strong immune-cell infiltration by TCD3 cells and macrophages. Lung Cancer 2016, 98: 51– 58. 6Kim S, Kim MY, Koh J, Go H, Lee DS, Jeon YK, et al. Programmed death-1 ligand 1 and 2 are highly expressed in pleomorphic carcinomas of the lung: Comparison of sarcomatous and carcinomatous areas. Eur J Cancer 2015, 51(17): 2698– 2707. 7Jiao Y, Liu M, Luo N, Guo H, Li J. Successful treatment of advanced pulmonary sarcomatoid carcinoma with the PD-1 inhibitor toripalimab: a case report. Oral Oncol. 2021; 112: 104992. 8Dahan R, Sega E, Engelhardt J, Selby M, Korman AJ, Ravetch JV. FcγRs modulate the anti-tumor activity of antibodies targeting the PD-1/PD-L1 axis. Cancer Cell. 2015; 28(3): 285– 95. 9Zhang T, Song X, Xu L, Ma J, Zhang Y, Gong W, et al. The binding of an anti-PD-1 antibody to FcgammaRIota has a profound impact on its biological functions. Cancer Immunol Immunother. 2018; 67(7): 1079– 1090. 10Liu SY, Wu YL. Tislelizumab: an investigational anti-PD-1 antibody for the treatment of advanced non-small cell lung cancer (NSCLC). Expert Opin Investig Drugs 2020; 29(12): 1355– 1364. 11Shen L, Guo J, Zhang Q, Pan H, Yuan Y, Bai Y, et al. Tislelizumab in Chinese patients with advanced solid tumors: an open-label, non-comparative, phase 1/2 study. J Immunother Cancer 2020, 8(1), e000437. 12Desai J, Deva S, Lee JS, Lin CC, Yen CJ, Chao Y, et al. Phase IA/IB study of single-agent tislelizumab, an investigational anti-PD-1 antibody, in solid tumors. J Immunother Cancer. 2020; 8(1); e000453. 13Lee A, Keam SJ. Tislelizumab: first approval. Drugs. 2020; 80(6): 617– 24. 14Babacan NA, Pina IB, Signorelli D, Prelaj A, Garassino MC, Tanvetyanon T. Relationship between programmed death receptor-ligand 1 expression and response to checkpoint inhibitor immunotherapy in pulmonary sarcomatoid carcinoma: a pooled analysis. Clin Lung Cancer. 2020; 21(5): e456– 63. 15Taniguchi H, Takemoto S, Ozasa M, Honda N, Suyama T, Umeyama Y, et al. Remarkable response to pembrolizumab with platinum-doublet in PD-L1-low pulmonary sarcomatoid carcinoma: a case report. Thorac Cancer 2021; 12(7): 1126– 1130. 16Nishino K, Kunimasa K, Kimura M, Inoue T, Tamiya M, Kuhara H, et al. Favorable response to pembrolizumab after durvalumab failure in a stage III sarcomatoid carcinoma of the lung: a case report. BMC Pharmacol Toxicol. 2020; 21(1): 26. 17 BeiGene: China National Medical Products Administration approves BeiGene's tislelizumab for patients with classical Hodgkin's lymphoma who have received at least two prior therapies. [cited 2019 Dec 27]. Available from: http://www.beigene.com.
留言 (0)