
記住我

Non-small cell lung cancer (NSCLC) is the most common type of cancer with high mortality worldwide. Epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs) are important milestones in the development of tumor-targeted therapy and have greatly improved outcomes for NSCLC patients. Osimertinib, the first third-generation EGFR-TKI, was initially approved for NSCLC patients with EGFR T790M mutations after resistance to first-generation EGFR-TKIs.1, 2 The phase III FLAURA study revealed that NSCLC patients treated with osimertinib had a significantly prolonged progression-free survival (PFS) and overall survival (OS) than those treated with first-generation EGFR-TKI as first-line treatment (PFS: 18.9 months vs. 10.2 months; OS: 38.6 months vs. 31.8 months).3, 4 Based on these findings, osimertinib was also approved as the standard first-line treatment for all EGFR-mutation patients. Unfortunately, patients treated with osimertinib inevitably develop resistance.
Multiple mechanisms are involved in resistance to osimertinib, including EGFR-independent mechanisms and EGFR-dependent mechanisms,5 such as tertiary EGFR C797S mutation, bypass (c-MET, HER2) or downstream activation (RAS family mutation and amplification), and histological transformation (small-cell lung cancer transformation and epithelial-mesenchymal transition).6 The resistance mechanism for approximately 50% of patients is unknown.7 Thus, the precise mechanism of resistance to osimertinib is not yet fully understood. These make the optimal treatment strategy still controversial.
Immunotherapy targeting the programmed cell death protein 1(PD-1)/ligand 1 (PD-L1) pathway has transformed the standard treatment for NSCLC. Multiple studies have shown superior survival benefits for anti-PD-1/PD-L1 inhibitors plus chemotherapy compared to chemotherapy in NSCLC patients without EGFR or ALK alterations.8-11 In addition, the study IMpower150 has reported the clinical benefit of anti-PD-L1 inhibitors in patients with EGFR mutations,12 while no data is available for patients progressing on osimertinib. White et al. found that immunotherapy plus chemotherapy did not promote PFS or OS in NSCLC patients resistant to osimertinib.13 Considering the inconsistent results among studies, the role of immunotherapy in patients with oncogenic drivers is still controversial. Here, we aimed to assess the efficacy and safety of immunotherapy plus chemotherapy (IO+C) compared with chemotherapy (C) in EGFR-mutant NSCLC patients progressing on osimertinib.
METHODS Patients and assessmentAdvanced NSCLC patients who experienced progression on osimertinib in the Chinese PLA General Hospital between June 2015 and September 2020 were included. This study was approved by the institutional ethics committee and was conducted by the Declaration of Helsinki. The informed consent was waived due to the retrospective nature of the study.
The inclusion criteria were as follows: (1) Histologically- or cytologically-confirmed lung adenocarcinoma, (2) stage IIIB–IV (American Joint Committee on Cancer eighth edition), (3) documentation of EGFR mutation and previously receiving osimertinib, (4) systemic progression on osimertinib with at least one measurable lesion, and (5) treated with anti-PD-1/PD-L1 inhibitors plus chemotherapy or chemotherapy alone after progression on osimertinib. Exclusion criteria were: (1) continuous treatment with osimertinib after progression on osimertinib, (2) Eastern Cooperative Oncology Group Performance Status (ECOG PS) worse than 3, (3) uncontrolled infection, and (4) treatment with immunotherapy before osimertinib.
Demographic data and clinical characteristics, including age, gender, smoking status, baseline EGFR mutation status, previous EGFR-TKI treatment, ECOG PS, radiological and laboratory data were collected from electronic medical records. Follow-up data were collected up to May 31, 2021. The median follow-up time was 11.2 months (range: 1.5–29.8 months).
The antitumor response was assessed by Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. PFS was defined as the duration time from therapy initiation to disease progression or death of any cause before disease progression; OS was defined as the time from the beginning of therapy to death. The rate of complete response (CR) and partial response (PR) was used to calculate ORR, and the rate of CR, PR, and stable disease (SD) was used to calculate DCR. Treatment-related adverse events (TRAEs) were graded using Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
TreatmentThe dosages of immunotherapy and chemotherapy for both groups were set according to the National Comprehensive Cancer Network or Chinese Society of Clinical Oncology guidelines. Specifically, the dosages of chemotherapy were 135–175 mg/m2 for paclitaxel, 75 mg/m2 for cis-platinum, AUC 5–6 for carboplatin, 500 mg/m2 for pemetrexed, and 75 mg/m2 for docetaxel on day 1 every 3 weeks. The dosage for etoposide was 100 mg/m2 on days 1 to 5 every 3 weeks. The dosages of immunotherapy were 240 mg or 3 mg/kg for nivolumab every 2 weeks, 200 mg or 2 mg/kg for pembrolizumab every 3 weeks. The dosage of bevacizumab was 7.5 mg/kg every 3 weeks.
Statistical analysisCategorical variables were analyzed using the chi-square or Fisher's exact test, and continuous variables were analyzed by Mann–Whitney U test or Student's t-test. Analysis of variance (ANOVA) was used to compare the difference among three or more groups. The Kaplan–Meier method was used to estimate OS and PFS. The univariate analysis between groups was assessed by a log-rank test. Cox regression was used to analyze the statistically significant factors according to the results of univariate analysis. All reported p-values were 2-tailed, and the difference was considered statistically significant at p < 0.05. Statistical analyses were conducted using IBM-SPSS Statistics version 20 (IBM Corp.). Univariate analysis and multivariate Cox regression hazard analysis were performed by R version 4.1.0.
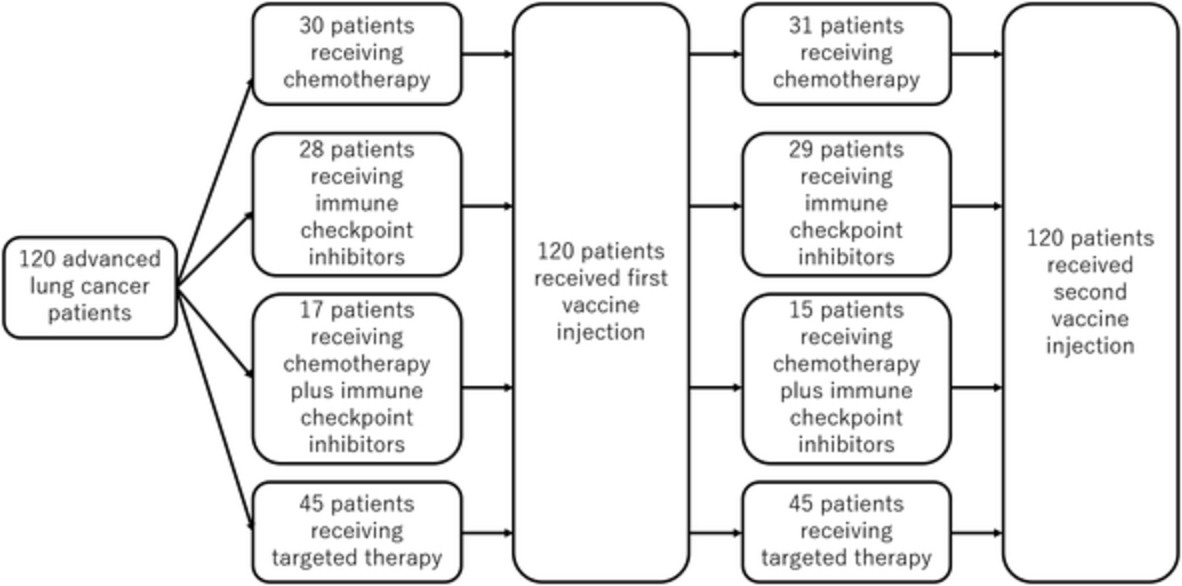
RESULTS Risk factors related to survival and baseline clinical characteristics in all patientsEighty-eight advanced NSCLC patients progressing on osimertinib were reviewed, and 40 patients met the inclusion criteria. The univariate analysis indicated that the therapeutic regimen was the only risk factor relevant with OS (12.8 vs. 10.5 months, HR: 0.39, 95% CI: 0.19–0.80, p < 0.01) (Supporting Information, Table S1). Hence, the 40 eligible patients were grouped according to the therapeutic regimen. Of the 40 patients, 20 were in the IO+C group, and the other 20 were in the C group. Figure 1 shows the workflow of this study.

Workflow of the present study
All baseline characteristics between the two groups were well balanced. The majority of patients were female (60% vs. 65%), non-smokers (75% vs. 85%), and ECOG 0–1 (75% vs. 70%) in the IO+C group and C group. A total of 90% of patients were stage IV in both groups, and most patients suffered multiple metastases with bone metastasis being the most frequent. All patients in both groups received two or more lines of previous treatment. With regard to EGFR mutation before osimertinib treatment, 10 patients harbored exon 21 L858R mutation, nine patients harbored exon 19 del mutation, and six patients harbored exon 20 T790M mutation in the IO+C group, whereas in the C group, 11 patients had exon 21 L858R mutation, eight patients had exon19 del mutation, and seven patients had exon 20 T790M mutation. Detailed comparisons are shown in Table 1.
TABLE 1. Characteristics of patients included in the IO+C and C groups Subgroup IO + C (n = 20) C (n = 20) p-value Gender, n (%) 1.0 Female 12 (60) 13 (65) Male 8 (40) 7 (35) Age, median (range) 55 (40–84) 58.5 (44–87) 0.3 Age, n (%) 0.7 <=65 17 (85) 15 (75) >65 3 (15) 5 (25) Smoker, n (%) 0.7 No 15 (75) 17 (85) Yes 5 (25) 3 (15) ECOG PS, n (%) 1.0 0–1 15 (75) 14 (70) 2–3 5 (25) 6 (30) Pathological stage, n (%) 0.5 Stage IIIB 2 (10) 2 (10) Stage IV 18 (90) 18 (90) EGFR mutation, n (%) Exon18 G719X 1 (5) 0 1.0 Exon19 del 9 (45) 8 (40) 1.0 Exon20 T790M 6 (30) 7 (35) 1.0 Exon21 L858R 10 (50) 11 (55) 1.0 Platinum-based chemotherapeutic agents, n (%) 0.2 No 12 (60) 7 (35) Yes 8 (40) 13 (65) Metastasis, n (%) Liver metastasis 7 (35) 6 (30) 1.0 Brain metastasis 10 (50) 11 (55) 1.0 Bone metastasis 14 (70) 16 (80) 0.7 Adrenal metastasis 5 (25) 4 (20) 1.0 Number of treatment lines, n (%) 0.5 Third 12 (60) 13 (55) Beyond fourth 8 (40) 7 (35) Abbreviations: C, chemotherapy; ECOG PS, Eastern Cooperative Oncology Group Performance Status; EGFR, epidermal growth factor receptor; IO+C, immunotherapy plus chemotherapy. Clinical responseThe clinical response was compared between the two groups. Our results showed that ORR (45% vs. 25%, p < 0.01) and DCR (85% vs. 65%, p = 0.03) were significantly higher in patients in the IO+C group than those in the C group. In the IO+C group, nine (45%) patients achieved PR, eight (40%) patients gained SD, and three (15%) patients suffered progressive disease (PD). In the C group, the numbers of patients who experienced PR, SD, and PD were five (25%), six (30%), and nine (45%), respectively.
Comparison of PFS between patients in IO+C group and C groupThe median PFS was significantly longer in patients in the IO+C group than those in the C group (6.4 vs. 2.8 months, HR: 0.41, 95% CI: 0.20–0.82, p < 0.01) (Figure 2a). To identify the patients who most probably benefit from the addition of immunotherapy, subgroup analysis of PFS was performed. Our results indicated that patients age ≤ 65, liver metastasis, adrenal metastasis, and third-line treatment had significantly prolonged PFS in the IO+C group compared with those in the C group (Figure 3, Table 2). Notably, the number of patients in the adrenal metastasis and liver metastasis subgroups was relatively small. In addition, our results also showed that patients in subgroups of both sexes, bone or brain metastasis and exon 19 del or exon 21 L858R mutation showed a trend of longer PFS in the IO+C group (Supporting Information, Figure S1).

Survival comparison between patients in the IO+C and C groups. (a) Comparison of progression-free survival (PFS). (b) Comparison of overall survival (OS)

Subgroup analysis of PFS between patients in the IO+C and C groups. (a) Age ≤ 65 subgroup. (b) Liver metastasis subgroup. (c) Adrenal metastasis subgroup. (d) Third-line treatment subgroup
TABLE 2. Subgroup analysis of PFS and OS between patients in IO+C and C groups Subgroup PFS (months) OS (months) IO + C C IO + C C n mPFS 95% CI n mPFS 95% CI p-value mOS 95% CI mOS 95% CI p-value Gender 0.1 0.003 Female 13 6.0 5.2–6.8 12 3.9 1.4–6.4 12.8 3.2–22.4 11.6 8.2–15.1 Male 7 8.0 3.0–12.9 8 2.8 1.1–4.5 12.3 10.5–14.1 10.4 2.5–18.3 Age 0.04 0.003 <65 17 6.1 2.9–9.2 15 2.8 0–5.7 12.7 10.9–14.4 10.5 8.7–12.3 ≥65 3 7.3 5.8–8.8 5 3.9 1.2–6.6 19.4 6.9–32.0 6.2 0–20.0 Smoker 0.09 - No 15 6.4 4.7–8.0 17 2.8 0.5–5.1 12.8 10.6–15.0 10.5 8.6–12.4 Yes 5 8.0 2.9–13.1 3 9.1 NR 23.2 NR 7.8 NR ECOG 0.04 0.003 0–1 15 6.4 4.3–8.5 14 2.8 0.8–4.8 12.3 10.5–14.1 10.4 4.6–16.2 2–3 5 8.0 3.9–12.1 6 2.2 0–8.3 21.5 2.9–40.1 2.3 6.0–15.1 EGFR mutation Exon19 del mutation 9 8.0 1.0–14.9 8 2.8 1.9–3.7 0.07 19.7 2.5–36.9 10.4 8.2–12.6 Exon20 T790M mutation 6 5.6 5.2–6.1 7 4.3 3.3–5.3 0.08 11.0 10.3–11.7 10.67 0.8–20.5 Exon21 L858R mutation 10 6.4 4.5–8.3 11 3.9 0.02–7.8 0.09 11.6 9.6–13.6 10.5 5.0–16.1 Liver metastasis 0.02 0.004 No 13 7.3 5.0–9.6 14 4.3 1.3–7.3 12.7 1.9–23.5 10.7 9.2–12.1 Yes 7 6.4 1.6–11.1 6 2.0 1.7–2.3 12.8 9.1–16.5 6.8 0–13.7 Brain metastasis 0.2 0.006 No 10 10.1 4.6–15.6 9 3.9 0–8.6 19.4 5.3–33.6 10.5 2.1–18.9 Yes 10 5.6 5.0–6.3 11 2.8 0.5–5.1 12.7 10.2–15.1 10.7 9.0–12.4 Bone metastasis 0.09 0.006 No 6 8.0 0.1–15.9 4 2.0 0.2–3.7 29.8 3.3 0.6–6.0 Yes 14 6.1 5.4–6.7 16 2.8 0.02–5.6 12.7 11.0–14.3 10.7 9.1–12.2 Adrenal metastasis 0.03 0.002 No 15 6.1 5.1–7.0 16 3.9 1.2–6.6 12.8 3.5–22.1 11.6 9.6–13.6 Yes 5 10.1 5.6–14.6 4 1.7 0.8–2.7 12.3 10.3–14.3 3.1 0.4–5.8 Platinum-based regimens 0.01 0.009 No 12 6.1 5.4–6.7 7 2.0 1.9–2.1 11.6 9.6–13.6 11.6
留言 (0)